
Abstract
Patient with chronic obstructive pulmonary disease (COPD) has to become a partner and an active participant in his own care, that is, disease self-management. The goal of this article is to present successful and unsuccessful interventions using patient self-management and to propose a model of integrated care more suitable to the needs of COPD patients. This is a narrative review and an opinion article. Many systematic reviews have shown positive outcomes for patients with COPD. These studies have in common a self-management intervention including an action plan in the event of an exacerbation embedded in an integrated health-care system coordinated by a case manager for educational sessions and regular communication. Recently published trials have brought controversy with respect to the effectiveness of self-management programmes, especially in patients with high burden of disease and co-morbidities. It may be more challenging to make the patient with high burden of disease a partner and not without risk of serious adverse events. Finally, our health-care delivery has to be well integrated and more coherent, that is, strategic alliance between primary and secondary care, and supported by interdisciplinary teams for patients with high-risk and complex COPD. Clinical practice has to be structured to address COPD throughout the disease spectrum, that is, secondary versus primary, team work, partnership, self-management and continuity of care.
Introduction
Driven by an aging population, morbidity and mortality from chronic disease such as chronic obstructive pulmonary disease (COPD) will continue to grow. 1 COPD is a disabling disease characterized by repetitive exacerbations resulting in higher utilization of health resources, 2 especially among patients with advanced COPD and co-morbidities.
The sooner the patient with COPD can master his disease, the better it would be for him. This is possible by implementing a self-management programme while fundamental principles are followed, that is, with respect to patient needs and capacities. The patient’s expertise for achieving an optimal daily life with his disease has to be seen as a central component of care delivery. 3 For this to happen, the patient has to become more knowledgeable, and he has to develop the confidence, that is, self-efficacy, with respect to specific health behaviours and the recognized skills needed to cope on a day-to-day basis with his disease. 4 Patients with chronic illnesses also require the provision of continuity of care at the location where the patient lives. Then, we can expect real benefits on patient well-being and autonomy and on the health-care system, such as a reduction in emergency department visits and hospital admissions.
In this article, will to present successful and unsuccessful interventions using patient self-management and a real life situation from which we can learn. We are proposing a model of integrated care more suitable for the needs of patients with COPD.
Successful interventions using patient self-management
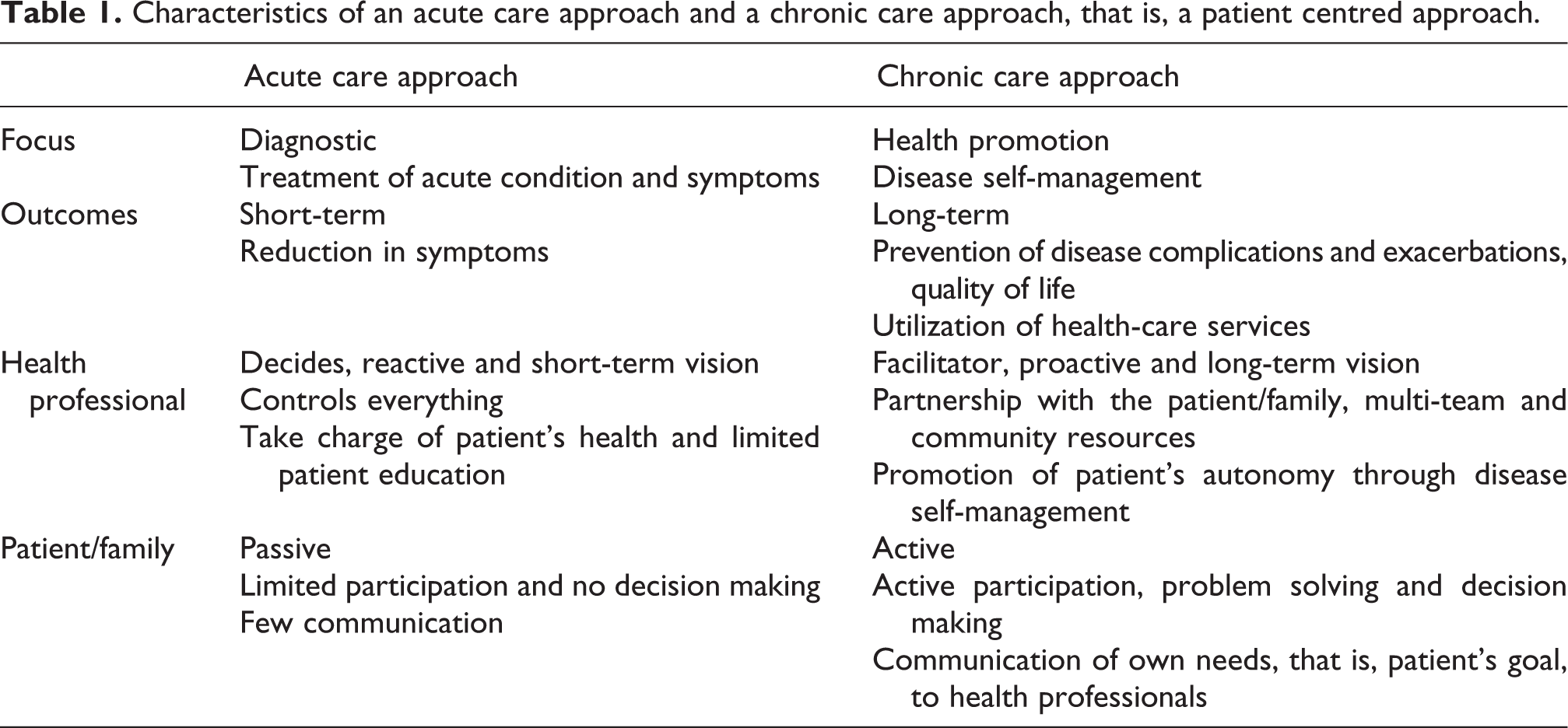
There is a fundamental need and both the health-care system and the health-care professionals have to move from an acute care to a chronic care approach (Table 1). The most successful and cost-effective interventions have used a patient self-management component. 5 With this realization, new care models have shifted towards a patient-centred approach where the patient is an active participant in the management of their own health. 6 The premise is that if individuals receive effective self-management support, they can be empowered to adopt behavioural need to cope with their disease on a day-to-day basis and many of the poor outcomes related to chronic disease can be averted. 4
Characteristics of an acute care approach and a chronic care approach, that is, a patient centred approach.
Many systematic reviews of self-management in COPD have been carried out and published. These reviews have shown positive outcomes for patients with COPD. In a Cochrane review,5 it was demonstrated that self-management programmes reduce the probability of COPD-related hospital admissions (odds ratio (OR): 0.64 and 95% confidence interval (CI): 0.47, 0.89) and improve health status (St George’s Respiratory Questionnaire: OR: −2.54 and 95% CI: −5.14, −0.02). This translates into a 1-year ‘number needed to treat’ of 10 (6 to 35) for patients with a 51% risk of exacerbation and of 24 (16 to 80) for patients with a 13% risk. This review included 14 studies from which six studies included the use of an action plan in the event of an exacerbation. The results from those six studies showed positive effect on health service utilization with a marked reduction in hospital admissions (OR: 0.60 and 95% CI: 0.42, 0.86). Another systematic review 7 demonstrated a significant reduction in health-care utilization (unscheduled/emergency centre visits, number of hospitalizations and length of hospital stay) in trials that implemented self-management with other components of the chronic care model compared with trials with self-management alone. This last review teaches us a lesson. Education alone is insufficient and self-management education has to be part of an integrated health-care system with communication and continuum of care. Results of another systematic review 8 indicated that disease-management programmes significantly improved exercise capacity (32.2 m, 95% CI, 4.1–60.3), decreased risk of hospitalization and moderately improved health-related quality of life.
On the basis of these reviews, one question that is often raised is which specific component of the interventions is needed to bring benefit such as improved patient well-being and reduced hospital admissions? The real question should not be only which component but by which process a self-management programme will have the best chance of success. All the individual trials that have shown benefits,9,10 including two more recent trials,11,12 have in common a self-management intervention including an action plan in the event of an exacerbation embedded in an integrated health-care system coordinated by a case manager for educational sessions and regular communication for empowerment (monthly visits or telephone calls). This reinforces the premise that if patients receive effective self-management support then they can be empowered to adopt healthy behaviours and many of the poor outcomes related to chronic disease can be averted. There are still many challenges trying to understand why some programmes succeed where others fail. The answers to this question will not be found in simply adding up the successful programmes and subtracting the unsuccessful one. This is not about winning or losing.
Self-management unsuccessful, failing to intervene
Some very recently published trials have brought controversy with respect to the effectiveness of self-management programmes, especially in those patients with high burden of disease and co-morbidities. We can learn from these studies that have shown negative results. The devil is in the details.
Bucknall et al. from their Glasgow supported self-management randomized clinical trial 13 could not show any difference between the intervention group and the control group in the primary (hospital admissions) and secondary outcomes. However, they showed that a significant minority of patients did benefit from the intervention. As a secondary analysis, the authors demonstrated that patients who adhere more to the training sessions and the nursing support, that is, the successful self-manager, had significantly lower hospital admissions than those who are not successful self-managers. Although the specific intended behaviour of self-managing COPD exacerbations was not directly measured in the trial, these results imply that to be successful, the patients have to adopt the intended behaviour.
A self-management programme should aim at behaviour change as a first target outcome. The examination of the process leading to change remains an important area of study. Changing and maintaining the patient’s behaviour are the only ways through which we can expect to improve patient’s health and reduce health service use such as hospital admissions. Recently, studies have started to look at behavioural change as an intermediate outcome in COPD self-management. In a study by Bischoff et al., 14 patients who were adherent to their written action plan had a reduced exacerbation recovery time with statistical (p = 0.0001) and clinical (−5.8 days) significance. It could not be demonstrated that it affected unscheduled health-care utilization (OR: 0.94, 95% CI: 0.49 to 1.83), although the study was not powered to show a reduction in emergency department visits or hospital admissions. Factors associated with an increased likelihood of adherence were influenza vaccination, cardiac co-morbidity, young age and lower forced expiratory volume in 1 second as percentage predicted. Many of these studies needed us to know to whom we need to give much attention, that is, patients who are at higher risk of being non-adherent to the intended behaviour.
Disappointment has been experienced recently with the results of a very large multisite randomized clinical trial, the Breath trial, by Fan et al. 15 In this study, the investigations were unable to show a reduction in hospital admissions as a primary outcome, and to everyone’s surprise, there was an increase in mortality (all causes and respiratory specific causes) in the self-management when compared with the standard care group. In this trial conducted in the US veterans with severe COPD, patients in the comprehensive care management programme almost a week before taking medications for an exacerbation against what was recommended by the action plan and did not take medications any sooner than the usual care group. An average of 2.5 exacerbations per patient-year were treated with prednisone in the intervention arm compared with 2.1 with usual care (p = 0.011), and the average delay in prednisone treatment after symptoms began was 6.4 days in the intervention group and 7.7 with usual care (p = 0.48). An average of 2.7 exacerbations per patient-year were treated with an antibiotic compared with 2.5 in the usual care group (p = 0.118), and the average delay in antibiotic treatment was 7.0 days in the intervention group and 6.8 days in usual care (p = 0.84). These results on how patients were prompt to access antibiotics and/or prednisone in the event of an acute exacerbation demonstrate clearly that patients in the comprehensive care management programme did not take medications any sooner than the usual care group. In other words, by not adopting the intended behaviour, this is a failure to intervene.
However, it is unclear why more patients in the comprehensive self-management group died than those in the standard care group. Here are potential explanations although they remain unproved. The study case managers who instructed the cohort had various backgrounds, including nurses, respiratory therapists, study coordinators and medical assistants. Their background and skill in managing ill patients with complex COPD under a variety of conditions is unclear. We know that the patient with high burden of disease needs special and quick attention. Another potential key finding is that many patients in the interventional arm had fatal COPD-related events but had less urgent visits to emergency department, suggesting less intense treatment received by the comprehensive care management group. These data suggest that in the trial, the comprehensive care management plan failed in its intent to provide timely care for patients with worsening symptoms of an exacerbation. Finally, we may not be able to claim generalizability with the results of this trial. However, the Breath trial sends us an important message. There is no such thing as benign intervention, especially when we are dealing with patient with high burden of disease.
Is it possible and safe to make the patient with high burden of disease a partner, that is, participant in his day-to-day monitoring and management? There are indications from a real life study that it is possible. 16 In patients with severe COPD, many were prone to exacerbations and were able to increase their ability to properly self-manage their acute exacerbations and this was associated with further reduction in emergency hospital visits and/or admissions. In order to be successful and harmless to the patient, this study highlights the necessity for detailed, easily accessible and frequent interactive communication (increased telephone call) with highly skilled and experienced self-manager.
Management by the patient has to vary within the continuum of the disease. Self-management will not suit all patients. Patient care and medical decisions may need to be taken over by the health professionals at a certain time of the patient’s disease trajectory or under certain conditions. This could be justified because patient presents with disease instability or co-morbidities, which may interfere with his capacity of making decision and being at unacceptable risk of mortality. However, these adjustments can only happen in an integrated system of care well adapted and centred on the needs of the patient (Figure 1). 17

Disease management adapted and centred on the needs and the capacities of the patient. Reference 17.
Integrated care model with good primary and secondary care
The overriding focus of self-management programmes in COPD has been primarily on secondary and tertiary care, with less attention to primary care, that is, these programmes can be effectively integrated into wider primary health-care services. Increasingly, many countries have recognized and endorsed the need for self-management programmes within national standards of care. However, with few exceptions, COPD self-management programme in primary care does not have a great uptake yet. Furthermore, we have given very little thought to how and when they should be offered to patients.
The current reality is that most self-management education occurs during brief sporadic clinical visits or through referral to a one-time series of education classes 18 and is rarely integrated into the usual medical treatment provided to the patient. 19 More than that, most of these programmes educate patients, while the programme should aim at changing and adopting new behaviours. People who tried to simplify the self-management programme by limiting the intervention to education without proper communication, support and empowerment by a case manager or a resource person have been unsuccessful in showing patient well-being and health service benefits. 20 Self-management is likely to be the most effective when education is combined with feedback and reinforcement from the health-care team on an ongoing basis. Moreover, change in behaviour evolves over time, with different patterns and timelines for different individuals. This requires that information be tailored to the patient’s needs, knowledge level and clinical profile and be accessible by the patient when they need it most; when action in response to changes in disease condition is required (e.g. a sudden increase in symptoms, i.e. COPD exacerbation).
We need a model of care delivery that is well integrated and more coherent, that is, with good primary and secondary care. Figure 2 shows a care model that emphasizes the distinctiveness of individual chronic diseases, aiming to increase efficiency and a reduction in duplication. In this model, there is a strategic alliance between primary and secondary care on a given territory, and delivery of care is provided according to disease stratification. Chronic disease management and patient self-management will vary within the continuum of disease. Health-care plan and service have to be adapted to patient needs. Patients with less severe disease and those with capacity to manage their disease will need minimal supervision. Primary care has to be able to make an early diagnosis and to promote a healthy lifestyle (e.g. smoking cessation and physical activity). In primary care, a team approach, that is, an interdisciplinary team with dedicated resource person, will also be needed for patients with high-risk COPD, that is, patients with moderate-to-severe disease and those having exacerbations. More complex cases need the expertise and follow-up in secondary/tertiary care. For example, in secondary/tertiary care, pulmonary rehabilitation that includes self-management is the most intensive method to increase self-help skills and healthy lifestyle better adapted to the daily needs of patients with COPD. 21

Integrated care model with strategic alliance between primary and secondary care and delivery of care according to disease stratification.
Conclusions
Patient’s self-management should be an important goal in the physician practice and in our health-care systems. Clinical practice has to be structured to address chronic conditions throughout the disease spectrum, that is, secondary versus primary, team work, partnership, self-management and continuity of care. Yet, political attention to our health-care system continues to primarily focus on the delivery of episodic, acute care, while chronic care, which should be delivered in an organized, consistent manner, is still too often highly fragmented and inefficient. Decent care starts with thoughtful programmes, good primary and secondary care, involving patients in their care, and it should also include a willingness to measure performance and insist on quality improvement.
In research, we still have many needs to be able to better customize self-management programmes of COPD. To be broadly applicable, further research need to include larger, higher quality studies using proper and well-described self-management interventions aimed at behavioural change. Behaviour change should be required as an outcome measure and follow-up also needs to be realistic and sufficiently long. We also need studies to better define the use of professional ‘case manager’ and non-professional interface, that is, computerized telephone system, COPD portal, and so on. Finally, we need studies that demonstrate applicability and effectiveness in primary care practice.
Footnotes
Conflict of Interest
The authors declared no conflicts of interest in relation with this topic.
Funding
This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.