
Abstract
The aim of the present study was to describe the perspectives of individuals with chronic obstructive pulmonary disease (COPD) who participated in a minimally supervised maintenance exercise intervention and identify the barriers and facilitators associated with participation. The intervention was delivered in a community center and was designed to maintain exercise capacity and quality of life following discharge from pulmonary rehabilitation. This study utilized qualitative focus groups (FGs) involving individuals with COPD (n = 12) who had been attending the maintenance community program for at least 6 months. All individuals who met the inclusion criteria for the FGs consented to participate. Four themes were identified: (1) issues around attendance; (2) perceived benefits of the program; (3) perceived burdens of the program; and (4) recommendations for program improvement. Participants expressed more benefits than barriers, stating that their experience of improved function and quality of life facilitated their attendance. Barriers included exacerbations, fatigue, access to transportation, and weather. Participants endorsed the benefits of a community-based maintenance exercise program after pulmonary rehabilitation. Minimally supervised community-based programs with access to a case manager may provide a useful approach to enhancing adherence to exercise.
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive condition that is optimally managed using an interprofessional approach to care. 1 Pulmonary rehabilitation (PR) consists of exercise training, education, psychological, and social support and has been shown to result in short-term improvements in exercise capacity and health-related quality of life in individuals with COPD. 1,2 However, these benefits deteriorate over time with outcomes often returning to preintervention levels within 1 year. 3,4 Therefore, PR programs must consider strategies to promote an effective transition from hospital-based care to long-term maintenance in the community.
The most common reason for the diminution of effects of PR is nonadherence to the home exercise program, particularly after exacerbations. 5 Consequently, there is growing interest in maintenance exercise interventions after PR. In a recent meta-analysis, Beauchamp et al. 5 noted that although supervised post-PR exercise programs were more effective than usual care at maintaining exercise capacity at 6 months, this difference was not sustained at 12 months, and there was no effect on health-related quality of life. In light of these findings, the authors emphasized the need for identifying barriers to adherence in order to optimize post-rehabilitation programs.
Low levels of objectively measured physical activity are the strongest predictors of all-cause mortality in individuals with COPD. 6 Unfortunately, maintaining consistent levels of physical activity is a challenge for individuals with COPD as they experience dyspnea with exertion. A recent systematic review highlighted changing health status, personal issues, lack of support, external factors, ongoing smoking, and program-specific barriers as commonly identified barriers to sustaining physical activity. 7 Social support, professional support, personal drivers, personal benefit, control of condition, specific goals, and program-specific enablers were cited as enablers. 7
Individuals with COPD feel that ongoing, structured exercise programs following discharge from PR are essential in order to maintain activity levels. 8 Professional and peer support are key elements in this transition, as the exercise facility itself may precipitate feelings of intimidation or embarrassment. 8 In preliminary studies on factors that promote participation in maintenance exercise among patients with COPD, encouragement, professional support, goal setting, the company of others, positive personal attributes, and the availability of relevant exercise programs 9,10 were identified as enablers. Barriers included health status, fear, cost, lack of support, the environment, and travel time. 9,11 These patient perspectives are important for guiding the development of new approaches to maintenance exercise and for understanding why certain programs are more effective than others.
We have recently reported on the effects of a novel post-rehabilitation community-based exercise program for individuals with COPD. 12 After completion of institutionally based PR, patients were transitioned to a community-based exercise program with the assistance of a case manager. Trained fitness instructors provided minimal supervision for the exercise program, and the case manager remained available to patients for providing support during exacerbations. We demonstrated sustained improvements in exercise capacity and health-related quality of life, at 6 months and 1 year after PR. The current study builds on these results by describing perspectives of the individuals with COPD who participated in this maintenance intervention with an emphasis on determining the barriers and facilitators associated with the program.
Methods
Study design
Three focus groups (FGs) were conducted, each with three to six individuals with COPD. The qualitative aspect of the study involved four phases: development of the FG guide; structured FG sessions; transcription of content; and data analysis. The protocol was approved by the Joint Bridgepoint/West Park/Toronto Central Community Care Access Centre Research Ethics Board.
Participant recruitment
Inclusion and exclusion criteria
Inclusion criteria for the community-based program has been considered based on the study by Beauchamp et al. 12 ; individuals with COPD were considered eligible for the community-based program if they were clinically stable and had successfully completed inpatient or outpatient rehabilitation. During a 2-year period (September 2009–September 2011), 293 patients enrolled in PR at our center were screened for study eligibility. Of these, 200 (68%) did not meet inclusion criteria based on distance from the community center (n = 90), diagnosis (n = 66), or medical instability (n = 44). Therefore, a total of 93 patients were approached for inclusion of whom 29 (31%) consented to enroll in the study. As part of the written informed consent process for the overall exercise program, all 29 participants in the community-based program consented to participate in the FGs, should they be invited.
The first 12 individuals who completed at least 6 months of the community-based program were invited to participate in FGs. This criteria was selected to ensure that FG participants had sufficient experience in the program and optimizing their ability to provide recommendations.
Community-based maintenance exercise program
The community-based maintenance exercise program was developed in partnership with the City of Toronto, Parks, Forestry and Recreation Division, a municipal-level not-for-profit governmental organization. It was offered at a single community recreation center. Prior to program initiation, a single education session regarding issues pertinent to supervising patients with COPD during exercise was conducted with fitness instructors from the participating community site.
The case manager, a registered physiotherapist, attended the first exercise session in order to introduce the participant to the fitness center staff and to provide support and encouragement to them. The maintenance intervention was for 1 year for a minimum of two, 1-hour sessions per week. The specific content of each exercise program varied according to the individual’s specific needs. A staff fitness consultant was always available to assist participants with exercise progression, but provided minimal formal supervision unless specifically requested.
FG sessions
We conducted a total of three FGs, each with 3 to 6 participants (total n = 12), between April and November 2010. FGs were conducted by an experienced facilitator, who was not a member of the research team, using a semi-structured FG guide. Participants were encouraged to describe their perceptions of the exercise program, to reflect on their involvement in the process, and to identify the barriers and facilitators to their participation in the program. FGs were audio-recorded and were approximately 1 hour in duration and occurred when participants had completed at least 6 months of the year-long intervention.
Data analysis
An experienced transcriptionist was hired to transcribe all the audiotapes verbatim and review the transcripts to ensure accuracy. All data were imported into the NVivo 8 qualitative data analysis software 13 for data management. The data were analyzed according to thematic content analysis to categorize the recurrent or common “themes.” For the first cycle of analysis, data were organized into initial deductive codes derived from the research aims and questions and therefore captured barriers and facilitators to program participation. During the second cycle of analysis, it became evident that some of the initial deductive codes could be collapsed, resulting in a total of four themes. The third cycle involved inductive coding that allowed codes to emerge from the data in order to identify unanticipated subthemes. The criterion for identifying recurring themes was based on the number of participants across FGs who mentioned it. The fourth and final level of analysis involved the summary of each of the four themes, including definitions and a description of subthemes. Multiple coding cycles facilitated greater levels of abstraction and the identification of patterns and recurring themes. Two coders individually coded the first transcript, comparing the results, and revising as needed.
Results
Participants
A total of 12 individuals with COPD were eligible to participate in the FGs at time of the study. All 12 consented, with three each in FG1 and FG2, and six in FG3. Table 1 shows the participant characteristics. Of the 12 participants, 6 (50%) were female and 4 (33%) were receiving supplemental oxygen. The average age of participants was 68 ± 9 years. The mean forced expiratory volume in 1 second (FEV1%) predicted was 44 ± 18% and the mean percentage of FEV1/forced vital capacity (FVC) predicted was 43 ± 14%, consistent with severe COPD (Stage III) as defined by Global Initiative for Obstructive Lung Disease classification criteria. 14 The average improvement in 6-minute walking distance (6MWD) following completion of PR was 26 ± 53 m. After being enrolled in the program for 6 months, the mean 6MWD was 374 ± 80 m, with a median value of 3 on the Medical Research Council dyspnea scale.
Characteristics of focus group participants.

FEV1: forced expiratory volume in one second; FVC: forced vital capacity; PR: pulmonary rehabilitation; 6MWD: 6-minute walk distance; BMI: body mass index; F: female; M: male.
Themes
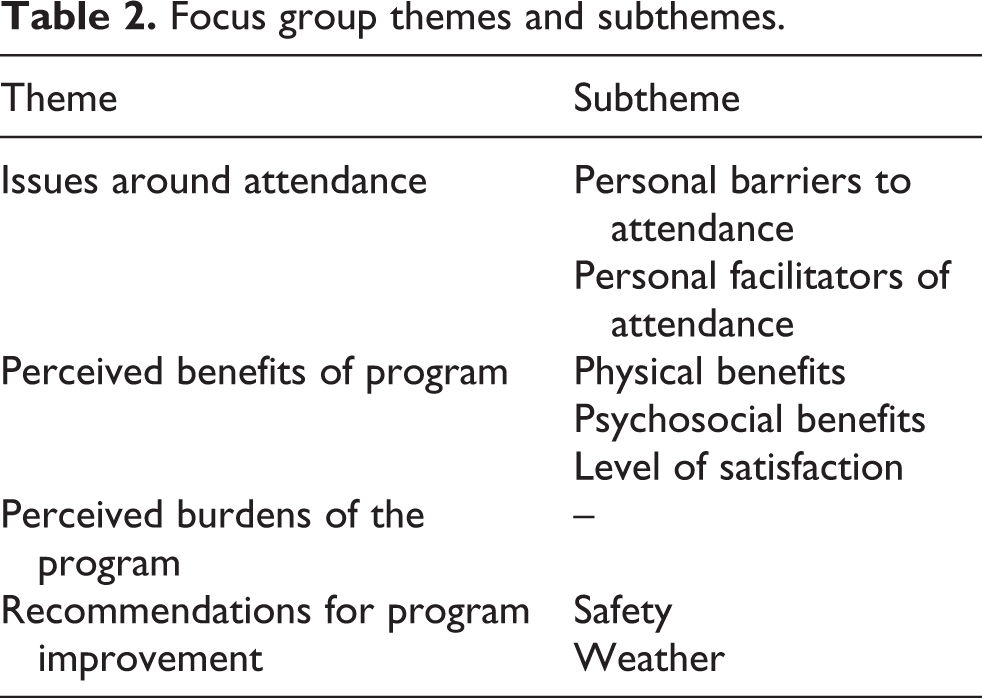
Analysis revealed a total of four themes with associated subthemes (Table 2). Themes included: (1) issues around attendance; (2) perceived benefits of the program; (3) perceived burdens of the program; and (4) recommendations for program improvement.
Focus group themes and subthemes.
Issues around attendance
Issues around attendance were based on participant comments about attending the program, circumstances that impeded attendance and those that facilitated it.
Personal barriers to attendance
A total of 18 references were made regarding barriers to attendance with specific reference to physical and psychosocial barriers. Barriers were comments related specifically to attending the program and circumstances that got in the way of participant attendance. Physical barriers were related to sickness, exacerbations, over performing, fatigue, comorbidities, and the weather. Participants described their post-exacerbation experiences as follows: I know when I was sick for 2 weeks and then went back, holy mackerel! I couldn’t do what I was doing before! (FG1, P3)
Oh yeah, that (an exacerbation) knocks you on your ass for sure. I managed to keep myself out of hospital this time. (FG1, P3)
Psychosocial barriers that impacted participants’ program attendance centered around emotions, including depression, loneliness, lack of motivation, and social isolation. Sometimes you get depressed, regardless … It’s terrible sometimes, it’s very lonely … And you don’t have people to talk to. (FG3, P1)
Other barriers that influenced attendance related to the distance some participants had to travel to get to the community center, as well as the costs related to transportation.
Personal facilitators of attendance
A total of 10 references were made regarding facilitation of participant attendance, including improved functioning, improved quality of life, program availability, and program structure. Participants expressed that having a program with a structured time and place, including access to exercise equipment, encouraged attendance. The consistency and structure allowed participants to look forward to attending and establish a routine. Participant’s experiences of improved physical functioning translated into personal motivation and improved quality of life, which was further enhanced by the social aspect of the program. Tired of being sick all the time. Want to get better, try to improve myself. More quality of life. Just to get out, and meet different people. (FG1, P3)
Perceived benefits of the program
Perceived benefits were the most frequently cited theme with 37 references, including 25 relating to level of satisfaction. Participants overwhelmingly endorsed the benefits of the program, whether described in physical or psychosocial terms. Several participants commented on the excellence of the facility’s equipment and reinforced that the accessibility of the program was highly valued.
Physical benefits
Participants across the FGs talked at length about the physical benefits of participating in the program with 14 references highlighting improved physical function. They emphasized the importance of continuing with their exercise in order to avoid setbacks. Many participants commented on the daily activities they could do with greater ease as a result of the program. I don’t need oxygen to shower now. (FG1, P3)
Improvement for me was that when I started … I only walked 3 or 5 times, 3 I think so, around the track. Now I walk 16. (FG1, P2) Participants also referred to improvements in physical functioning in terms of their relationship to others, observations made by others, and avoidance of hospitalization. Participants experienced an improved ability to walk with their children and less shortness of breath when spending time with friends. Some explained that they no longer required frequent trips to the emergency department and felt as though they no longer noticed the impact of their COPD. Besides that, you know like, when I first got this COPD, it was a big problem. I couldn’t breathe. I was going to Emergency pretty near every second, third day … and now I’m pretty near free of the … I don’t even feel the COPD at all… (FG2, P3)
Psychosocial benefits
Psychosocial benefits were referenced 14 times across the FGs. The majority of psychosocial benefits were related to participants’ interpersonal relationships with the instructors. Participants continually spoke of the positive interactions and supportive presence and flexibility of the instructors and case manager, which contributed to their sense of safety, and comfort within the program. So that I liked, the fact that I can go in there, and they’ve showed me what I should be doing. And I can do as much or as little of that as I want to … It meant, I like the fact that they allowed you to learn or go at your own pace. Nobody’s pushing or pulling. (FG3, P2)
Several participants discussed the psychosocial benefits they experienced from the support of their peers. For many participants, psychosocial benefits were related to increased feelings of accomplishment, achievement, and motivation, which are all important aspects of self-esteem. When I see them there, it gives me, you know, incentive, encouragement. Because we suffer from the same thing, and that is, where the hell do I get my next breath. (FG1, P1)
Participants recognized the importance of an integrated program, not only in the community but also the members of the community center itself. Experiencing social connection with regular gym members assisted the participants in feeling socially included and valued. That it’s in the community … I like being with other people. So it’s not all, um, walkers and oxygen tanks. (FG2, P1)
Perceived burden of the program
A total of 11 references to the burden of the program were identified across the FGs. Burdens related to the negative aspects of the overall design of the community program itself. There was significant overlap between program burdens and recommendations, as participants foresaw ways to overcome these burdens. Commonly perceived burdens included costs and proximity to the program. … I have to go a little bit of a distance to get there, which I’m quite willing to do, if it isn’t going to cost me money. But I want something closer to home if I have to do this on a regular basis, which I do. (FG3, P1)
Concerns were also expressed relating to access during the winter months, as parking filled up faster, road conditions were unpredictable, and ice was not always completely removed from the parking lot, making some participants feel unsafe.
One participant found doing the exercises themselves a burden as and another participant had been attending the program for 6 months and felt that they were not improving or progressing as they had missed the 3-month checkup with their respirologist.
Recommendations for program improvement
Participants were invited to make recommendations for improvements to the program. The most frequently sighted recommendation was for expanding the number of locations in which the program was held, in order to facilitate access and reduce the burden of travel with respect to both time and money. If you’re very close to it, you could walk or take TTC [city of Toronto public transportation system]. But when you’re far away – I’m not saying I’m far away, but far enough. I couldn’t take, TTC would take too, too long, I’d have too many transfers. (FG3, P3)
Several recommendations were made to enhance the patient safety of the program. Participants suggested an oxygen tank and oxygen saturation monitor be on-site as a safety measure for them. Additionally, they suggested instructors be knowledgeable about using both pieces of equipment in order to assist in supervising the patients. Participants expressed that having more handicapped parking spaces and keeping parking spots free of ice in the winter would assist those with breathing difficulties to access the building.
Participants felt strongly that future patient membership costs should be subsidized, as many were unable to work or reported being on a fixed income. They should pay for it, really. It keeps us out of hospital. How much is a visit to the hospital? (FG1, P3)
Another participant had the benefit of her husband attending the program with her even though he did not have COPD. He paid full membership fees, but did have access to the support of the instructors, and this participant recommended that other people’s spouses be encouraged to attend as paying participants as well. Joint participation in the program was perceived as supportive and encouraging with respect to long-term adherence.
Discussion
This study was designed to understand the experiences of individuals living with COPD who participated in a post-PR community-based exercise program previously demonstrated to be successful in improving exercise capacity and quality of life. Exploring the participants’ experiences through FGs highlighted their positive perceptions surrounding the unique structure of the maintenance program and uncovered the barriers and facilitators associated with program participation.
The primary barriers to participation were consistent with previous literature 7 –9 and included the effort to overcome a change in health status secondary to an exacerbation and seasonal weather patterns. Encouragement and social support were the primary facilitators, which have been highlighted by previous COPD studies. 8,10 This study is unique as it examines the perspectives of patients who participated in a minimally supervised program that was delivered outside of a health care institution. Furthermore, individuals enrolled in the program had moderate to severe COPD (Table 1) and participated successfully with no adverse events without direct supervision from a health-care professional. 12 Participants expressed many positive experiences relating to community center staff and reported feeling safe as a result of their presence, in addition to other members of the community center. As the case manager was affiliated with the PR institution, the participants still felt part of the hospital community although they had successfully transitioned to a community setting, overcoming previously cited gaps in maintenance care. 10 This program design may represent a transition between the more closely supervised initial rehabilitation program and a minimally supervised self-management model.
Participants highlighted the physical benefits of the program, citing improved function and quality of life as facilitators of participation, in addition to the existence and structure of the program. These results are consistent with the patient’s enthusiasm for structured maintenance following discharge from PR. 8,9,11 Participants overwhelmingly endorsed the benefits of the program and consistently identified more facilitators than barriers or burdens, reflecting their positive experience in the community-based exercise program. Barriers were primarily unrelated to the program itself and included exacerbations, fatigue, mood, and weather. Participant’s positive experiences in the program were further reflected in their recommendations, which addressed the majority of program burdens that were expressed.
Limitations
When interpreting these observations, it should be considered that participants for this study were recruited from a single center and therefore the results may not be reflective of clinical populations from other institutions. Furthermore, as all participants had successfully completed a formal hospital-based rehabilitation program, the results cannot be extrapolated to environments where individuals enter a community-based fitness center without having first completed an institutionally based intensive program.
Conclusion
Participants endorsed the benefits of a minimally supervised community-based maintenance exercise program after PR. They expressed more benefits than barriers and stated that improved function and quality of life facilitated their attendance. The existence and structure of the program, feelings of accomplishment, and social support encouraged their participation. Barriers included respiratory exacerbations, fatigue, access to transportation, and weather. The most frequently cited recommendations were to expand the number of program locations and to subsidize the cost. When participants expressed program burdens they often provided recommendations to address them to enhance future program implementation.
Footnotes
Appendix 1: Patient Focus Group Outline
Does anyone have any questions before we begin?
What did you like best about the program? What did you like least about the program? Do you think the program was beneficial? Why or why not?
Is there anything else I haven’t asked that you think we should know?
Acknowledgement
The authors would like to thank Dr Barb Gibson for her guidance and constructive feedback with regard to study design.
Funding
This project was funded by grants from the Centre for Urban Health Initiatives; the Ontario Thoracic Society; and the Care to Know Centre of Saint Elizabeth Health Care. MB is supported by the Canadian Institutes of Health Research and DB is supported by a Canada Research Chair.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.