
Abstract
There is no conclusive evidence about the way to a promote behavior change in self-management programs for patients with chronic obstructive pulmonary disease (COPD). The latter is a significant knowledge gap as there is a need to promote a sustained effect in interventions like Pulmonary Rehabilitation or Supporting Programs. Embracing patient’s values seems to be a key ingredient to ignite genuine motivation for behavior change. This manuscript describes two pilot qualitative studies carried out in patients with severe COPD aimed to engage the patient inner experience and promote self-management: a trial testing motivational interviewing (MI) as one style of helping patients with severe COPD make changes in their behavior and second a trial testing a mindfulness-based intervention. The MI study consisted of a 3-month program of weekly coaching phone calls after one face-to-face visit. The following themes were outstanding: patients value the supportive communication with coach and believe the MI-based coaching created increased level of awareness and accountability. They perceived an increase in physical activity and reported “feeling better” or other benefits not directly related to exercise. The Mindfulness for Health Program was a mandatory 8-week program that consisted on 2-hour classes aimed to cultivate nonjudgmental attention in the moment (through different meditative practices and sharing) plus monthly face-to-face encounters aimed to sustain practice and sharing of life experiences for 1 year. The following themes (at 1 year) were outstanding: appreciating life by seeing hardships as opportunities, valuing the self through compassion and awareness, cultivating connectedness with others, acquiring joy, and adopting healthy behaviors. In the search for the “holy grail” for self-management programs that can promote a behavior change, mindfulness and MI seem promising for cultivating a way to live a life in which people are fully present and consciously agree with.
Keywords
Introduction
There is no conclusive evidence about the way to promote a behavior change in self-management programs for patients with chronic obstructive pulmonary disease (COPD). At the core of this crisis is a lack of patient engagement: that was recently suggested in a recent randomized study of COPD self-management. 1 In COPD care, we find ourselves spending most of their time solving the same problems over and over again. As a result, their ability to empower patients is limited. Embracing patient’s values seems to be a key ingredient to ignite genuine motivation for behavior change. New initiatives for self-management need to forge partnerships, and springboards projects to success by encouraging participants to share the core concepts of presenting and communication by pushing the limits of innovation/creativity in the very act of living learning from the very present moments as it emerges. Thus, program/practices that deeply touch the core of patients’ values and life experiences have the best chance to create the condition for change. Such programs can be complementary to exiting and established programs like Pulmonary Rehabilitation and Self-Management/Coaching Programs. The ultimate goal is to promote sustainable changes in people’s quality of lives and impact positively health care outcomes like hospitalizations, utilization, and end of life care.
We pilot tested two particular interventions aimed to deeply touch the core of people values to create the condition for creation/innovation/change in daily lives from observation, reflection:
Motivational interviewing (MI), which is one style of helping others, make changes in their behavior. It contrasts with the more typical directing helping style where the health-care provider tries to install knowledge or motivation. A health-care practitioner who uses an MI style goes beyond just guiding when he or she tries to solicit from people his or her desires and reasons for engaging in the health promoting behavior. Two key aspects of MI are Acceptance, responding to the client as a person who is competent rather than someone who needs to be rescued or is incapable of making health promoting decisions, and Compassion, MI is not something one does to someone, does in order to get to some goal of the health-care provider, or does as part of selling the client on something. MI is about opening the mind and the heart to people. 2
Mindfulness is a purposeful nonjudgmental attention to the moment that is formally learned through different meditative practices but aimed to be applied to every “mundane” task, like eating, walking, facing difficult and nondifficult emotions. Ultimately aims to be more present in life as it is: mindfulness is a deliberate attitude to face life no matter what is happening in life at the moment. Through mindfulness training, people learn to recognize and discriminate between components of experience, including thoughts, feelings, and sensations, and developing a nonreactive awareness of these. The mindfulness-based stress reduction (MBSR) is a widely available group-based mindfulness training program that reduces perceived stress, disease-related distress, and reported medical symptoms in a range of chronic diseases. 3–5
We set out to test the qualitative effect of the above interventions in patients with severe COPD as to establish foundation knowledge to guide well-designed studies
Methods
Study sample (both studies)
Participants were adult patients recruited between October 2009 and December 2011 from pulmonary care clinics at Mayo Clinic, Rochester, Minnesota, USA. Both studies were approved by the Mayo Clinic Institutional Review Board, and all patients signed consent before entering the study.
Inclusion criteria were physician-documented severe or very severe COPD, by smoking exposure and pulmonary function tests. Patients were excluded if they had exacerbations in the past month or if at the time of the consent were attending a pulmonary rehabilitation program to avoid contamination of the results. For the mindfulness trial, patients were also excluded if participated in MBSR and/or practicing meditation regularly.
Mindfulness study: mindfulness for health program
Mindfulness for Health Program was a modified version of MBSR 3,6 that consisted of 8 weekly 2-hour sessions, plus a monthly meeting for 1 year. The modification consisted in the lack of the all-day retreat and the addition of the monthly session to sustain the mindfulness practice and dialogues between the participants about using mindfulness in daily life. Formal mindfulness training was accomplished through the following techniques: body scan, when attention is systematically moved through the body to bring awareness to sensations; sitting meditation focusing on awareness of breathing, thoughts and feelings; and gentle stretching exercises to develop awareness during movement. The classes emphasized integration of mindfulness into everyday life to support coping with symptoms and stress. A CD containing guided mindfulness exercises was provided to be practiced for 30 minutes, 6 days/week. The 1-hour monthly session consisted in a 15-minute breathing awareness practice; a 15-minute gentle stretching exercises to develop awareness during movement and a 30-minute session of sharing the previous month progress.
MI-based coaching
Each patient received 10 telephonic health coaching calls of 15–20 minute duration over 3 months (weekly calls during 1st and 2nd month, bi-weekly calls during 3rd month). The health coach for the trial was a nurse trained in MI. A detail of the MI coaching training and method has been recently published. 7 The spirit of the MI (Figure 1): compassion and acceptance of the patient as competent and autonomous to make their own decision, evocation of the patients’ reasons to change or not, and collaboration guided the sessions. Using open-ended questions, and reflections, the interventionist explored awareness of physical activity, ambivalence toward exercise and lifestyle changes, and listened for opportunities in which the patient expressed the will to make a change in any behavior (change talk). Participants frequently raised COPD-related self-management questions during coaching sessions, and numerous strategies were offered including breathing awareness through slow pursed-lip breathing, pacing strategies for exertion, and the use of an emergency plan if appropriate.
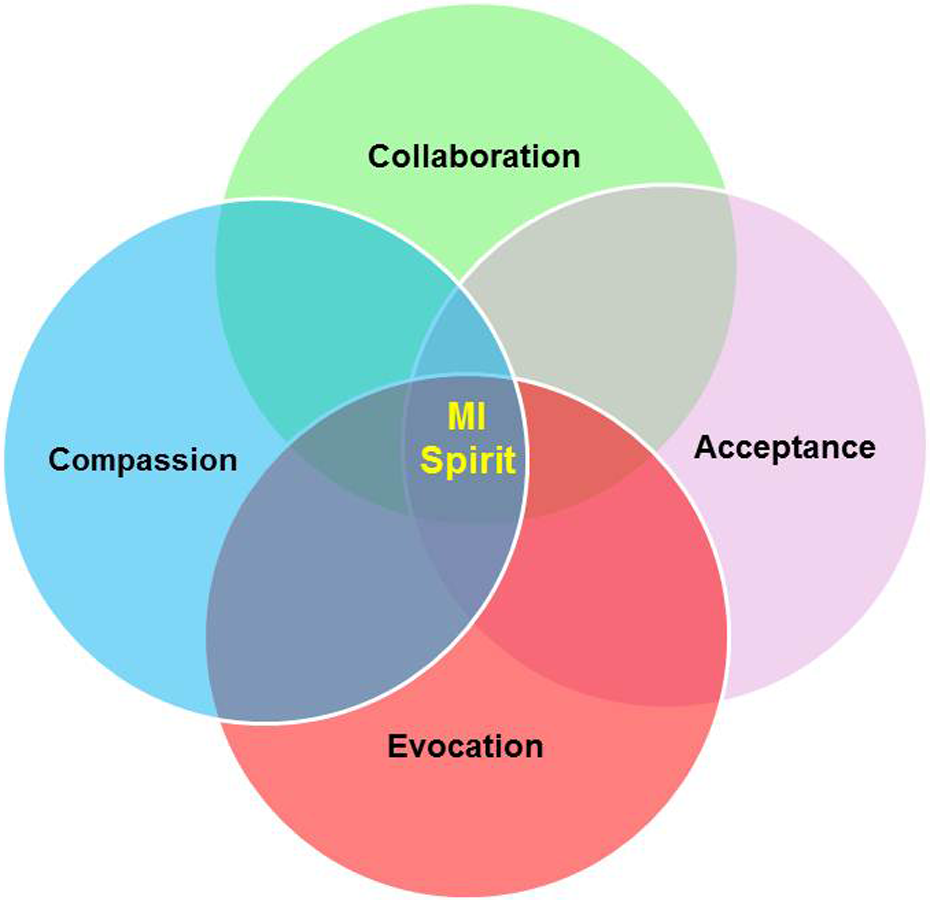
The spirit of motivational interviewing.
During the 3 months of coaching, participants were asked to complete a brief, daily log of their physical activity and symptoms (Figure 2). The completed log was made available to the coach and the information was used to provide feedback, engage the participant in a discussion about trends and impressions, and giving the participants opportunity to reflect on their efforts and feelings. The session usually, but always ended in a plan of action on the topic of choice to the patient. A menu of options (Figure 3) for every domain (physical activity, stress/emotions or breathing) was available if necessary to increase patients' options for a plan (if the patient wanted to make one). In the delivery of the intervention, we wanted to add a tool that measure (a) agreement between patient and provider on the self-management tasks (b) agreement on the goals of self-management, and (c) development of an affective bond between the interventionist and the patient. We choose the Working Alliance Inven-tory-Short Revised (WAI-SR), a recently refined measure of the therapeutic alliance that assesses all three key aspects mentioned and demonstrated good psychometric properties. 8 Based on the previous research, we hypothesize that higher working alliance will be associated with better patient outcomes. 9,10

Patient diary in the motivational interviewing intervention.

Sample of the menu of options for self-management in the motivational interviewing intervention.
Qualitative analysis (both studies)
All participants in both were interviewed by a study investigator who did not deliver the intervention. These interviews were conducted by telephone and were guided by a semi-structured interview guide, which included open-ended questions and rating scales. These questions assessed satisfaction with program content and delivery, perceived benefits of the program and behavior changes resulting from the program. Data from interview questions was analyzed independently by two study investigators using the methods of content analysis. The analysis followed standard qualitative methodology triangulated analysis, and the use of reflexive narratives aimed to maximize the transferability of interview data. Transcriptions were independently coded line by line by two and were then compiled into preliminary coding schemes. Following principles of grounded theory, a final set of themes and subcodes inductively emerged. 11–13
Results
MI-based coaching
Participants were 51 patients, of whom 29 (57%) were male, aged 68.5 + 7.7 years (mean + SD). Patients had moderate to severe disease with forced expiratory volume in 1 second (FEV1) 39.4 + 15.3% of the reference value. Of them, 44 patients (86%) completed the study intervention.
The interviews themes and selected quotes from the qualitative analysis are shown in Table 1.
Qualitative interviews themes from the Motivational Interviewing Intervention: common themes and selected quotes.

Working alliance
Patient ratings of their working alliance with the interventionist using the WAI-SR revealed positive perceptions of the relationship. The majority of patients rated “very often” or “always” true statements, reflecting positive aspects of their relationship with the interventionist. Most patients reported that “very often” or “always” 1 : the patient and interventionist agreed about strategies to improve the patient’s situation (88.5%) 2 ; the patient believed that the interventionist liked them (92.3%) 3 ; they had confidence that the interventionist could help them (84.0%) 4 ; they worked towards mutually agreed upon goals (84.6%) and agreed on what is important to work on (84.6%); and 5 the way they were working on the patient’s problem was correct (100%).
Mindfulness intervention
Ten patients, (57% male), aged 67 + 6 years (mean + SD). Patients had moderate to severe disease with FEV1 29 ± 8% of the predicted value. Modified Medical Research Council Dyspnea score 2 ± 1 (scale 0–4). The 1-year intervention was completed by 70%.
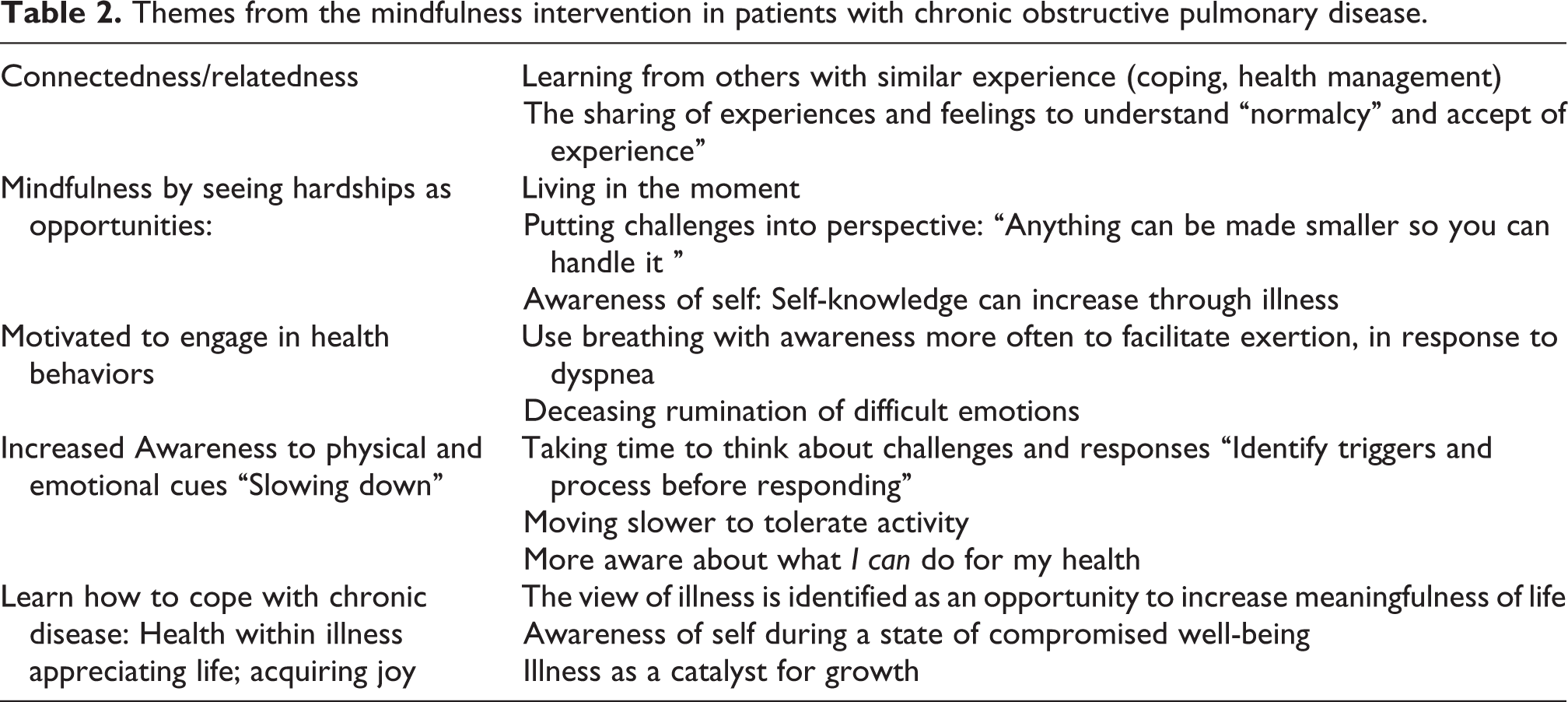
The interviews main themes and subthemes from the qualitative analysis are shown in Table 2.
Themes from the mindfulness intervention in patients with chronic obstructive pulmonary disease.
Discussion
The results from the two qualitative studies presented in this manuscript may shed some light into the “unknown” that we have in the field of COPD self-management: how to embrace patients and ignite inner motivation that may change behavior. We believe that now, in view of recent research, by accomplishing that change, we may not only improve people’s quality of life but also health related outcomes (less hospitalizations, more daily activity, exacerbation-related unscheduled visits).
The primary reason for exploring the above methods were in part their successes in other disease processes that were chronic and needed a significant behavior change: chronic pain, breast cancer for mindfulness interventions, 3,14 and addictions, diabetes, and heart failure 15–17 for MI.
Motivational interviewing
The spirit of MI include four strong foundations that may explain its impact and effectiveness in the context of suffering: Compassion (the desire to see others free from suffering), Acceptance (prizing the inner worth and potential of every human being), Evocation (people have within them what is needed to move forward), and Partnership (“MI is done for and with a person: it is an active collaboration between experts”). 18 The above spirit set the tone for an intervention that is certainly directed at embracing the individual at the very deep level.
The themes obtained in the in-depth interviews are indicative of meaningful topics that are at the core of rehabilitation and the promotion of self-management in COPD: effective and inspiring communications, self-determination for accountability, perception of improved physical activity, the comprehensiveness of the self-management intervention that goes beyond a prescription that in the view of a patient are clinically relevant (obesity and emotions). While far for being accomplished outcomes, provide a glimpse of what is possible with this intervention. A detailed method of training for MI-based interventions in COPD has recently been published by the Journal of the American Association for Cardiovascular and Pulmonary Rehabilitation. 7 Proper comprehensive training is critical for delivering an intervention based on compassion, acceptance, and with good listening skills.
The developers set a few guiding principles for the delivery of MI, 18 which are as follows:
Motivation to change is elicited from the client, and not imposed from without.
Direct persuasion is not an effective method for resolving ambivalence.
The counseling style is generally a quiet and eliciting one.
Readiness to change is product of interpersonal interaction more than a “patient trait”.
The therapeutic relationship is like a partnership or companionship than expert/recipient roles.
MI is not a technique or set of techniques that are applied to or (worse) “used on” people. If it becomes a trick or a manipulative technique, its essence has been lost.
A recent report of a patient-centered approach in COPD is also consistent to our findings. 19 Finally, we demonstrated a good working alliance between the patient and the provider, something that has been related to improved outcome 10 : our results from the MI intervention showed high scores in the WAI suggesting the degree of partnership that is intended in MI interventions. The latter has not been investigated in COPD self-management programs before and is perhaps a potential outcome to measure in future studies of self-management.
Mindfulness in COPD
The qualitative effect that this mindfulness intervention had in people suffering from COPD, if replicated in large well designed studies, could revolutionize the way we see treatment opportunities and communicate (particularly listen) with people with COPD during health encounters in rehabilitation and in chronic care.
Mindfulness has been described as a purposeful, nonjudgmental (labeling things as good or bad) attention to the present moment. 20
The tested mindfulness practices fostered meaning and the experience of feeling healthy for people living with a chronic illness by (a) valuing the self; (b) seeking and connecting with others; (c) seeing hardships as opportunities; (d) appreciating life; and (e) acquiring joy. The significance of these results is that they may be seminal for a reconceptualization of health and illness. Such a reconceptualization may ignite a transformation in chronic care and wellness promotion, from a problem focus and a deficit perspective, to one which focuses on the people’s capacity for promotion of their own health and healing. The effects seen by the mindfulness intervention has been postulated by the Health-within-Illness model. 21
Our promising qualitative results contrasted with a previous randomized study on mindfulness intervention in COPD that basically show no result. 22 However, a possible irremediable problem was present in that study (personal communication with the author) and it is that people were “randomized” to an intervention that require daily meditative practice (even if they like it or not), which may have been a significant barrier to the compliance of the intervention. Behavioral randomized clinical trials pose unique challenges and alternative designs in terms of their appropriateness to scientific and clinical goals that are a current matter of interest. Our intervention has a very important difference with the above trial and is the monthly encounter where people met and continued their practice for 1 year: that in the view of the author was the strongest factor to solidify a practice in the participants and likely need to be considering in future mindfulness trials in chronic disease. People still meet today after 2 years of finishing the study. In addition, a more recent and positive study of a mindfulness intervention in patient with chronic asthma support the equipoise in the topic of mindfulness in chronic lung disease and certainly more research is needed in this very topic to define its use and appropriateness. 6
One aspect that needs to be taken into account is that that the quality of a mindfulness intervention is only as good as the mindfulness instructor and his or her understanding of what is required to deliver a truly mindfulness-based program. There is certainly a need of a personal practice of mindfulness (that is usually rooted in a regular meditation practice) that may distill plainness and simplicity in the delivery of the intervention. It is amazing to see how the “mechanical teaching” of pursed lips breathing can be transformed in an illuminating and balancing “breathing awareness practice” when the right attention and intention is placed. The very same concept is applied to walking or any stretching exercise for that matter.
This intervention offers a different paradigm: illness is a potential catalyst for growth, which can provide the chance or circumstance for positive change and be an opportunity which increases meaningfulness of life. Connectedness or relatedness with the environment and awareness of self during a state of compromised well-being seem to be important components of this journey. 23
Final comments
A personal journey is probably necessary in the patient and the provider to deliver interventions as described above that are base in values such us compassion, acceptance (MI), and wholeheartedness and nonjudgmental attention (mindfulness). Those interventions by touching the very core of human values and promoting a different kind of listening (not only from the mind but also from the heart) can create the necessary condition to ignite motivation and a behavioral change that can be very transformative. Exploring new methods is a necessity in the field of behavior change and self-management in which the “holy grail” has not been found yet.
Footnotes
Conflict of Interest
The authors declared no conflicts of interest.
Funding
This work was supported by the National Institutes of Health (grant NIH NHLBI 1R01CA163293-01 (to R.P.B.)).