
Abstract
Weaning patients from mechanical ventilation has been compared to a cardiac stress test. Weaning failure (WF) from a cardiac origin can be common in patients with limited cardiac reserve. Diuretic and vasodilator therapies are indicated for WF due to excessive preload, afterload, or myocardial ischemia. Alteration in intrathoracic pressure and lung volumes may also impact weaning process in a patient with poor cardiac function. Noninvasive ventilation decreases cardiac stress load and should be utilized in weaning patients with poor cardiac reserves. In fact, positive pressure therapy is now the standard of care for treating a patient with acute pulmonary edema and to decrease afterload (Frazier et al. Biol Res Nurs 2000; 1(4): 253–264; Pinsky MR. Chest 2005; 128(5 Suppl 2): 592S–597S.). Recently, biomarkers and echocardiography have been utilized to assess weaning success during spontaneous breathing trials. In this article, we describe the physiological alterations in cardiac and pulmonary systems during the weaning process and its impact on weaning outcome.
Introduction
Mechanical ventilation (MV) accounts for 800,000 hospitalizations in the United States alone. Use of MV is common and consumes a significant amount of health care resources in the elderly patients. 1 The increased incidence of MV will ultimately exceed population growth. In the current health care system where MV patients use a significant portion of critical care resources, planning for this continued growth is crucial. 2
Weaning and minimizing the duration of MV in critically ill patients is an important task for critical care physicians. Discontinuation of MV should be considered as soon as the patient is able to follow commands and maintain appropriate minute ventilation. 3 In addition, airway reflexes should be intact and the patients’ clinical and mental status must have improved. The current practice for sedation interruption and spontaneous breathing trials (SBTs) results in better outcome in mechanically ventilated patient in the intensive care unit (ICU). 4 The recommendations regarding the management of weaning process are based on early weaning from MV, and SBT should be initiated as early as possible for at least 30 minutes of either tracheal tube breathing or low levels of pressure support. Assist-control ventilation modes should be favored in patients failing an initial trial/trials, and noninvasive ventilation techniques should be considered in selected patients to shorten the duration of intubation. 5 Weaning failure (WF) from MV may be due to altered mental status, increased tracheal secretions, inability to cough, critical illness, muscle weakness, and heart failure.
Unfortunately, weaning trials are usually performed with minimal attention to cardiovascular reserves. Therefore, weaning and extubation attempts can fail due to the patient’s limited cardiovascular reserves. 6 Consideration for baseline cardiac function may be an important factor in the selection of an appropriate mode of spontaneous ventilation following controlled MV. 7
Relationship of oxygen consumption and cardiac output to work of breathing
There are many studies reflecting on the concept of breathing as an exercise. 8 –12 Initial study by Coast and Krause looked at loaded breathing and voluntary hyperpnea while ventilatory work, cardiac output, and oxygen consumption were measured. He was able to demonstrate that loaded breathing and hyperpnea increased cardiac output and oxygen consumption. 13 To define the importance of hemodynamic performance and global tissue oxygenation in determining weaning outcome, Jubran et al. recorded mixed venous oxygen saturation (SvO2) continuously in 8 ventilator-supported patients who failed a trial of SBT and 11 patients who tolerated a trial and were successfully extubated. Immediately before the SBT, SvO2 was not statistically different in the two groups (p = 0.28). On discontinuation of the ventilator, SvO2 fell progressively in the failure group (p < 0.01) and remained the same in the success group. The success group demonstrated an increase in cardiac index (p < 0.05) and oxygen (O2) transport (p < 0.02). The failure group did not increase O2 transport, partly because of elevations in right- and left-ventricular afterload but, instead, demonstrated increased O2 extraction ratio (p < 0.02) with a consequent fall in SvO2. 14 Alternatively, gastric mucosal ischemia may develop in patients during unsuccessful attempts to wean them from mechanical ventilation because blood flow from nonvital organs is diverted to meet the increased demands of the respiratory muscle. Mohsenifar et al. demonstrated that gastrointestinal acidosis may be an early sign of WF from low cardiac output states. 15
Hemodynamic consequences of weaning trial
The initiation of and weaning from MV with extubation causes significant changes in intrathoracic pressure (ITP) that have profound consequences for the cardiovascular function. 6,16 As a result, hemodynamic compromise can occur during the weaning process in critically ill patients. Many ICU patients have subclinical or undiagnosed cardiac disease, and cardiovascular compensation is frequently hampered by the underlying critical illness. Therefore, in a significant proportion of patients, weaning and extubation attempts fail due to the patient’s limited cardiovascular reserves. 6
The original study by Lemaire et al. studied the hemodynamic effects of 15 patients rapidly weaned from MV with severe chronic obstructive pulmonary disease (COPD) and cardiovascular disease who were recovering from acute cardiopulmonary decompensation. In each patient, 10 minutes of spontaneous ventilation (SV) with supplemental O2 resulted in reduction of mean esophageal pressure and increase in cardiac index and systemic blood pressure. Most importantly, transmural pulmonary artery occlusion pressure (PAOP) markedly increased, mandating a reinstitution of MV. In four patients with left ventricular (LV) catheters, PAOP correlated with the LV end-diastolic pressure during both MV and SV. Gated blood-pool imaging showed no change in the LV end-diastolic volume index with LV ejection fraction. Patients were treated for a mean of 10 days with diuretics, resulting in a reduction of blood volume and body weight. Subsequently, of the 15 patients, 9 were weaned successfully from MV with unchanged PAOP (Figure 1). 17

Physiologic alteration leading to weaning failure. HPV: hypoxic pulmonary vasoconstriction; CO: cardiac output.
Similarly, Routsi et al. assessed the hemodynamic, respiratory, and clinical effects of nitroglycerin infusion in difficult-to-wean patients with severe COPD. Twelve difficult-to-wean COPD patients, who presented with systemic arterial hypertension during WF, had systemic and pulmonary artery catheters in place. Patients were studied in two consecutive days, that is, the first day without (control day) and the second day with (study day) nitroglycerin continuous intravenous infusion starting at the beginning of the spontaneous breathing trial and titrated to maintain normal systolic blood pressure. Hemodynamic, oxygenation, and respiratory measurements were performed on MV and during a 2-hour T-piece SBT. He concluded that nitroglycerin infusion can expedite the weaning by restoring weaning-induced cardiovascular compromise. 18
Alteration of lung volumes and ITPs and its impact on hemodynamic parameters
PVR changes
To explain the changes in pulmonary vascular resistance (PVR) with positive- and negative-pressure inflation, Hakim et al. conducted an experiment with an isolated canine lung in 1982. He demonstrated that lung inflation results in a volume-dependent increase in the resistance of both alveolar and extra-alveolar vessels. At lower lung volumes, alveoli collapse and hypoxia stimulate the pulmonary vasomotor tone by the process of hypoxic pulmonary vasoconstriction. 19 In contrast, at higher lung volumes, the PVR 20 and right ventricular afterload increases due to the increase in transpulmonary pressure. 21
Pinsky also demonstrated that the changes in lung volume alter the autonomic tone and PVR. Hyperinflation increases the PVR and pulmonary artery pressure, impeding right ventricular ejection fraction. 22,23
Similarly, Brower et al. demonstrated that during SBT, hyperventilation can lead to increased PVR, 20 and patients with lung disease are at increasing risk of hyperinflation and hemodynamic changes. 24,25
Venous return and afterload effects
Variations in ITP generated by different ventilator weaning modes may significantly affect hemodynamic and cardiovascular stability. 26 The heart is an intrathoracic organ; hence, any changes in ITP can lead to changes in LV afterload and venous return. 27,28
In 1984, Pinsky elegantly demonstrated in his study that spontaneous inspiratory efforts decrease ITP. Since diaphragmatic descent increases intra-abdominal pressure, these combined effects cause decrease in right atrial pressure and increase in venous pressure in the abdomen, markedly increasing the pressure gradient for systemic venous return. 29 As a result, the venous return is augmented and can impede LV ejection. Furthermore, the greater the decrease in ITP, the greater the increase in LV afterload for a constant arterial pressure and right ventricle stroke output increases. 30 Therefore, it is not surprising to see changes in hemodynamic parameters and development of pulmonary edema in patients with poor cardiac reserve (Figures 2 and 3). 31 –35

Hemodynamic alteration contributing to weaning failure. SBT: spontaneous breathing trial; ITP: intrathoracic pressure; RV: right ventricle; HTN: hypertension.

Spontaneous inspiration will decrease Ppl and intravascular AP, but the fall in Ppl is relatively greater than the fall in systolic AP. Therefore, transmural pressure (systolic AP-Ppl) actually increases, resulting in an increased LV afterload and a reduction in LV stroke volume. Additionally, during spontaneous inspiratory efforts, diaphragmatic descent increases intra-abdominal pressure leading to decreased right atrial pressure and increased venous pressure in the abdomen by compressing EGV and by markedly increasing the pressure gradient for systemic venous return. On the contrary, positive pressure ventilation increases ITP, right atrial pressure, and decreases transmural LV systolic pressure. This will reduce the pressure gradients for venous return and decrease LV ejection resulting in lower thoracic blood volume. EGV: extra-thoracic vessels; LV: left ventricle; RH: right heart; LH: left heart; Ppl: pleural pressure; AP: aortic pressure; ITP: intrathoracic pressure.
Other investigators have shown that increases in ITP result in the increases in right atrial pressure and decreases in transmural LV systolic pressure. This will reduce the pressure gradients for venous return and decrease LV ejection resulting in lower thoracic blood volume. This hemodynamic alteration usually generates a change in autonomic tone, so that cardiac output can be maintained. Hence, individuals with autonomic and/or cardiovascular dysfunction are at risk of WF. 26
Assessment of cardiac function during weaning
Natriuretic peptides
Brain natriuretic peptide (BNP) and atrial natriuretic peptide (ANP) are structurally similar peptides that are produced in cardiac myocytes. 34 In healthy patients, ANP is produced primarily in the atria and BNP primarily in the ventricles. Plasma BNP predominates over ANP under pathologic conditions and production of BNP rises strongly in both atria and ventricles. 35 Pre-proBNP is a peptide of 134 amino acids and is cleaved into proBNP (108 amino acids) and a signal peptide of 26 amino acids. ProBNP is subsequently cleaved into BNP (32 amino acids) and the inactive N-terminal proBNP peptide (NT-proBNP; 76 amino acids). 36,37 ProANP is a 126-amino acid peptide, which is cleaved by a serine protease into an active ANP (amino acids 99–126) and the inactive N-terminal fragment N-ANP (amino acids 1–98). 38
BNP levels have greater sensitivity and specificity for both systolic and diastolic dysfunction. 39,40 The release of BNP into the circulation is directly proportional to the ventricular expansion and volume overload of the ventricles and therefore reflects the decompensated state of the ventricles. 41,42
Initial observational pilot studies have addressed several potential indications in the ICU such as identification of cardiac dysfunction, risk stratification in severe sepsis and septic shock, evaluation of patients with shock, 43 and weaning from MV. 44
Multiple studies have addressed the question of whether BNP or NT-proBNP could be used to identify patients who fail to wean for cardiac reasons. 41,42,45 –50 The study by Zapata et al. evaluated and compared BNP and NT-proBNP concentrations to predict WF from MV due to heart failure (HF) before an SBT and to identify whether HF is the cause for WF. His group conducted a prospective observational study of 100 patients on MV for over 48 hours who underwent an SBT. Echocardiography and sampling for natriuretic peptides were performed immediately before and at the end of SBT. HF was diagnosed by PAOP > 18 mmHg or signs of elevated filling pressures in echocardiograph. A total of 32 patients failed the SBT, of which 12 were due to HF and 20 were due to respiratory failure (RF). Before SBT, BNP and NT-proBNP were higher in patients failing due to HF than RF or in successfully weaned patients. Cutoff values using receiver operating characteristic (ROC) curve analyses to predict HF were 263 ng/L for BNP (p < 0.001) and 1343 ng/L for NT-proBNP (p = 0.08). BNP and NT-proBNP increased significantly during SBT in patients failing due to HF. Increases in BNP and NT-proBNP of 48 and 21 ng/L, respectively, showed a diagnostic accuracy for HF of 88.9% and 83.3% (p < 0.001). BNP performed better than NT-proBNP for HF prediction (p = 0.01) and diagnosis (p = 0.009). 51 Mekontso-Dessap et al. prospectively studied 102 patients during a 1-hour weaning trial. Weaning was considered successful if the patient passed the trial and maintained spontaneous breathing for more than 48 hours after extubation. Plasma BNP was measured just before the trial in all patients and at the end of the trial in the first 60 patients. Overall, 42 patients failed the weaning process. Logistic regression analysis identified high BNP level before the trial and the product of airway pressure and breathing frequency during ventilation as independent risk factors for WF. BNP values were not different at the end of the trial. In nine of the patients in whom the weaning process failed initially, it succeeded later after diuretic therapy. Their BNP levels before weaning decreased between the two attempts (517 vs. 226 pg/mL, p = 0.01). 47 A total of 19 patients in whom weaning with COPD was difficult, Grasso et al. prospectively evaluated the utility of serial measurements of plasma NT-proBNP to detect acute cardiac dysfunction during WF. Of the 19 patients, 8 (42%) were identified with acute cardiac dysfunction at the end of the weaning trial. Baseline NT-proBNP levels were significantly higher (median 5000, interquartile range 4218 pg/mL) in these patients than in patients without evidence of acute cardiac dysfunction (median 1705, interquartile range 3491 pg/mL). Plasma levels of NT-proBNP increased significantly at the end of the spontaneous breathing trial only in patients with acute cardiac dysfunction (median 12,733 pg/mL, interquartile range 16,456 pg/mL, p < 0.05). The elevation in NT-proBNP at the end of the weaning trial had a good diagnostic performance in detecting acute cardiac dysfunction, as estimated by area under the ROC curve analysis (area under the curve, 0.909; standard error, 0.077; 95% confidence interval (CI), 0.69–0.98; p < 0.0001; cutoff = 184.7 pg/mL). 50 Chien et al. studied the role of BNP in patients who passed a 2-hour SBT. To determine the predictive value of BNP, 52 patients recovering from acute RF were enrolled as the testing group. The predictive value of BNP was validated in a second independent cohort of 49 patients. Then, both the groups were combined for final analysis. In the testing group of 52 patients, 41 passed SBT and were extubated. Of them, 33 patients (80%) were extubated successfully (extubation success) while 8 (20%) were reintubated within 48 hours (extubation failure). There were no differences in the baseline BNP levels, but the extubation failure group had significantly greater increases in BNP at the end of SBT than the extubation success groups (32.7%, 25–75 percentile = 25.7–50.8% vs. 0.69%, 8.8–10.72%, p < 0.001). The area under the ROC curve for the BNP change was 0.93 and an increase in BNP of <20% during SBT had the best combination of sensitivity, specificity, positive and negative predictive values, and diagnostic accuracy for predicting extubation success (91, 88, 97, 70, and 91%). The median BNP levels after the 2-hour SBT showing BNP levels were 461 (168–1202) pg/mL, 418 (218–1085) pg/mL, and 224 (112–660) pg/mL in the SBT failure, extubation failure, and extubation success groups, respectively. 46 Gerbaud et al. prospectively evaluated echocardiographic indexes and NT-proBNP as markers of acute cardiac dysfunction before and after SBTs to assess their ability to predict subsequent successful extubation. Forty four patients who underwent their first SBT were included. Plasma levels of NT-proBNP and transthoracic echocardiography (TTE) were recorded immediately before commencing and just before the end of SBT. NT-proBNP levels (8199 (3106–10,949) vs. 4200 (1855–7125) pg/mL, p = 0.004) increased significantly in those who failed the SBT (Table 1). 48
Prediction of weaning outcomes using BNP and proBNP.

HF: heart failure; WO: weaning outcome; BNP: brain natriuretic peptide; NT-proBNP: N-terminal proBNP peptide; ng: nanogram; pg: pictogram.
Echocardiography
There is growing evidence that TTE and transesophageal echocardiography (TEE) should be used to categorize the cardiac origin of WF. 52 Echocardiography provides a detailed cardiovascular assessment, based on the combination of real-time two-dimensional evaluation of cardiac structures and function as well as hemodynamic information provided by Doppler measurement of blood flow velocity. Echocardiography is a noninvasive tool for detecting LV filling pressure elevation or any undetected cardiac pathologies during SBT. Additionally, echocardiography is useful for functional hemodynamic assessment in ventilated patients with circulatory failure. 53 Although TTE remains the primary choice, TEE can provide additional value for better visualization of cardiac structures in the intensive care setting. TEE is superior to TTE in patients with suspected aortic dissection or aortic injury and in diagnosing suspected cases of endocarditis or source of emboli. 54
Tissue Doppler imaging (TDI) is a relatively new echocardiographic technique that uses Doppler principles to measure the velocity of myocardial motion. Doppler echocardiography relies on shift in the frequency of ultrasound signals from moving objects. With this principle, conventional Doppler techniques assess the velocity of blood flow by fast-moving blood cells. TDI uses the same Doppler principles to quantify the lower velocity signals. The analysis of transmitral flow measuring the peak Doppler velocities of early diastolic myocardial relaxation velocity (E a) below the baseline as the annulus ascends away from apex and myocardial velocity associated with atrial contraction (A) can be performed. The lower case “a” is for annulus or “m” for myocardial (E a or E m), and the superscripted prime symbol (E′) is usually used to differentiate tissue Doppler velocity from conventional mitral inflow (Figure 4). 55 TDI measurement of the E a′ reflects the load-independent measure of myocardial relaxation. The combination of TDI and pulsed Doppler transmitral flow allows calculation of the E/E a′ or simply E/E′ ratio (normal ratio <8) and correlates well with PAOP (Figure 4). 29,56 The study by Gerbaud et al. mentioned above looked at the weaning trials in HF patients by analysis of the transmitral Doppler inflow E velocity to annular tissue Doppler (E/E′) ratio measurement. He concluded that TTE could not predict the outcome of SBT but he noticed cardiac index increased significantly at the end of SBT in patients who passed the weaning trial. 48 In contrast, Moschietto et al. studied 68 patients on MV for 48 hours with a measurement of E/E′ using TTE. Of them, 20 patients failed the weaning process and the other 48 patients succeeded. Before the SBT, the E/E′ ratio was higher in the failed group than in the successful group. The E/E′ measured during the SBT was also higher in the failed group. E/E′ ratio of 14.5 provided a sensitivity of 75% and specificity of 95.8%. The LV ejection fraction did not differ between the two groups, whereas E′ was lower in the failed group. He concluded that diastolic dysfunction with relaxation impairment was strongly associated with WF. 57 Papanikolaou et al. evaluated 50 critical care noncardiac patients who met predetermined criteria for weaning and underwent Doppler echocardiography before and at the end of SBT. “Conventional” mitral inflow analysis and TDI parameters were used to assess the LV diastolic filling pressures. Weaning was considered successful if patients had been extubated after successful SBT and sustained spontaneous breathing for more than 48 hours. Of them, 20 patients failed SBT and 5 required reintubation within 48 hours. WF was associated with the degree of LV diastolic dysfunction at preSBT (p = 0.01). Patients who failed weaning presented with higher LV filling pressures at preSBT. PreSBT values of lateral E/E′ greater than 7.8 predicted WF. The area under the ROC curve was 0.86 with the sensitivity and specificity of 79 to 100%, respectively. Lateral E/E′ was the only factor independently associated with WF before SBT; odds ratio (95% CI) 5.62 (1.17–26.96), p = 0.03. He concluded that an E/E′ ratio greater than 7.8 may identify patients at high risk of WF. 58 Schifelbain et al. conducted randomized cross over clinical trial of 24 patients to analyze changes in cardiac function, using Doppler echocardiogram, in critical patients during weaning from MV. He used two different weaning methods: pressure support ventilation and T-tube. He did not find any differences between Doppler echocardiography and cardiorespiratory variables during pressure support ventilation and T-tube. However, cardiac structures were smaller, isovolumetric relaxation time was larger, and oxygenation levels were greater in successfully weaned patients. 59 It is probably safe to say that Doppler echocardiography and TDI have a place for assessment of WF due to cardiac origin if performed routinely in the ICU. Some of the major limitations for TTE, TEE, TDI, and deceleration time include lack of staff training and poor image acquisition in the critically ill patient; TDI only measures the vector of motion that is parallel to the direction of the beam, and it poorly differentiates between passive motion or tethering from active motion (fiber shortening or lengthening; Table 2.) 28,60,61
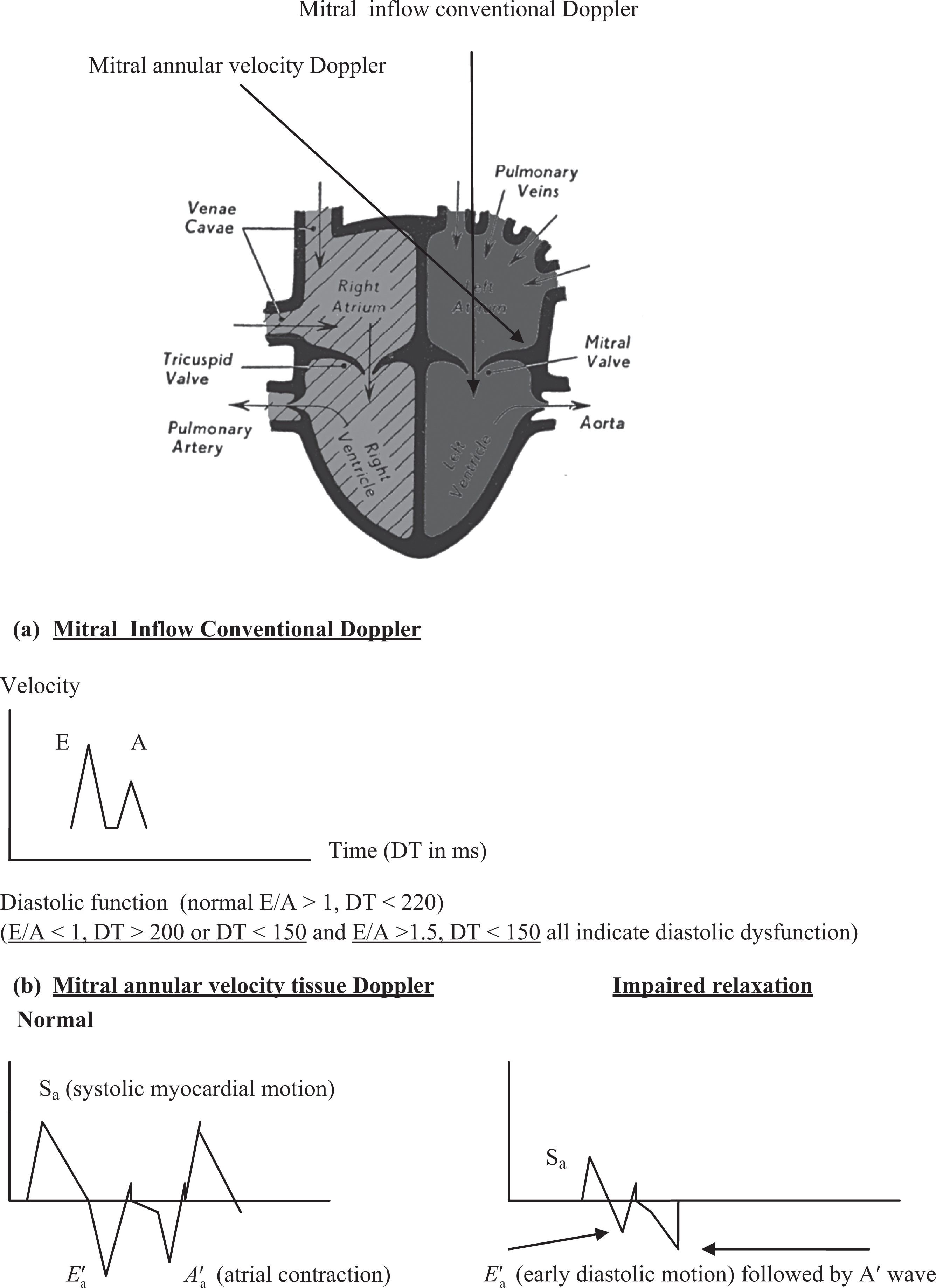
Two flow velocities can be seen during diastole: the E-wave, representing the early, passive filling of the left ventricle, and the A-wave that happens late in diastole, representing the active filling, the atrial contraction. (a) Mitral inflow conventional Doppler. (b) Mitral annular velocity tissue Doppler impaired relaxation normal.
Prediction of weaning outcomes using echocardiography.

E a′ or E′: early diastolic myocardial relaxation velocity below the baseline as the annulus ascends away from the apex; E: early diastolic (motion) mitral annular velocity flow.
Conclusion
Assessment and prediction of WF from cardiac origin remains complicated. The current prediction models are difficult to put into practice at the bedside. Point of care echocardiography by intensivist remains a valuable noninvasive tool when planning weaning strategies in the ICU. TTE, TEE, and Doppler echocardiography should be readily available and critical care physicians should be trained in its focused emergency use for these situations. In addition, serum BNP and NT-proBNP appear promising to identify patients with weaning difficulties due to cardiac disease.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.