
Abstract
Tiotropium is an innovative intervention in chronic obstructive pulmonary disease (COPD). Early adherence to tiotropium remains inadequately explored, notably time from initiation to discontinuation (persistence). In patients with COPD, the factors associated with the risk of discontinuing the treatment with tiotropium within 12 months following initiation were identified (12-month persistence). Claim databases from the French Social Security were used. A random sample of patients (aged 50–80 years) who initiated tiotropium soon after launch was selected. Factors associated with the persistence were investigated (Log-rank test and multivariate Cox model). Of the 1147 newly treated patients (mean age 68 years, 33% women), 64% remained in the treatment of tiotropium for over a period of 12 months following initiation. More than 10% of the patients interrupted therapy after a single dispensing, most often those with mild COPD. Lower risks of discontinuing tiotropium within 12 months following initiation were observed when it was initiated by a private sector specialist (hazard ratio (HR) = 0.65, 95% confidence interval (CI) = (0.52–0.82)), by hospital-based physician (HR = 0.58, 95% CI = (0.42–0.78)), when ≥ 2 other respiratory drugs were associated (HR = 0.74, 95% CI = (0.58–0.95)) and in case of long-term disease status (HR = 0.78, 95% CI = (0.63–0.97)). Conversely, no clear effect appeared according to age or gender. In this population of patients with COPD, fewer early discontinuations of tiotropium were observed in patients having a severe condition.
Introduction
About 7.5% of French people suffer from chronic obstructive pulmonary disease (COPD), 1 and mortality has been steadily increasing for the last 20 years. 2 COPD is not curable, and treatment is intended to control symptoms, to prevent exacerbations and to improve the quality of life.
When dyspnea is not relieved by symptomatic treatment based on as needed short acting beta agonists (sufficient for mild COPD), a long-acting inhaled bronchodilatator is recommended in case of moderate to very severe COPD. Long-acting inhaled bronchodilatators (salmeterol, formoterol and tiotropium) are more efficient. 3 Tiotropium is an inhaled long-acting anticholinergic maintenance treatment with demonstrated efficacy in COPD. It was launched in France in May 2006. Besides as-needed short-term therapy, tiotropium is a first-line treatment for patients with moderate-to-severe COPD. 3,4 As a rule, adequate adherence to the treatment is needed to optimise outcomes 5 Nonetheless, observational studies suggest less than optimal compliance with recommended drug therapy treatment for patients with COPD based on Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, 6 while a good adherence to inhaled therapy is needed for COPD quality of care. 3 A better adherence to tiotropium when compared with other respiratory therapy has been observed. 7,8 Nevertheless, early adherence to tiotropium within the first 12 months following initiation remains inadequately explored. This is notably the case of persistence which reflects the duration of time under therapy, from initiation of therapy to discontinuation. It is unclear that to which extent the persistence to tiotropium during the first 12 months of treatment may be influenced by the characteristics of the patients and disease or management-related factors. Also, it should be of interest to investigate whether persistent patients have temporary interruptions of dispensing during this period.
The aim of the present study was to identify, in a sample of newly treated patients, the factors associated to the discontinuation of tiotropium within the 12 months following initiation. The study was conducted during the period following the launch of the drug, at the time of significant expectations from patients and clinicians regarding its effectiveness. The other objective was to study the proportion of days’ supply under tiotropium amongst persistent patients.
Methods
Data source
Data were obtained from the French Health Insurance claims database from the Rhone-Alpes Region, during the period from January 1, 2006 to May 1, 2008. No authorisation from an Institutional Review Board was needed, as this observational study was conducted on anonymous claims data.
Study population
A random sample (10%) of patients, with at least three reimbursements of dispensed prescriptions of a respiratory drug (R03 Anatomical Therapeutic Chemical Classification) in 2006 was preselected. Among them, only patients aged 50–80 years, who initiated tiotropium (no dispensing of the drug beforehand) between May 2006 and January 2007, were studied.
Data collected
For each beneficiary, the database contains information on age and gender, long-term disease status and reimbursed medical therapy. Long-term disease status enables the patients with specific chronic conditions to receive free care for that condition, without personal, out-of-pocket payment. This status is specific to a given chronic disease. It is attributed for a patient based on clinical criteria of disease severity after agreement of the National Health Service
Analyses
In France, all the prescribed units of tiotropium other than in hospital settings are for 30 days, with a standard dose of one capsule per day. Hence, patients were assumed to be dispensed for their treatment on a monthly basis. The following two dimensions of adherence were studied.
Twelve-month persistence
First, discontinuation of tiotropium occurring within 12 months following initiation (study period) was investigated. Patients were considered as nonpersistent when the last refill was dispensed within 12 months following treatment initiation (Figure 1, patient A), in the absence of censoring data beforehand. Follow-up was censored in case of death occurring between therapy initiation and 12 months afterwards or for any subsequent dates to this time interval. Persistence at 12th month was defined by the presence of at least one dispensing of tiotropium beyond the 12th month following initiation (Figure 1, patient B).
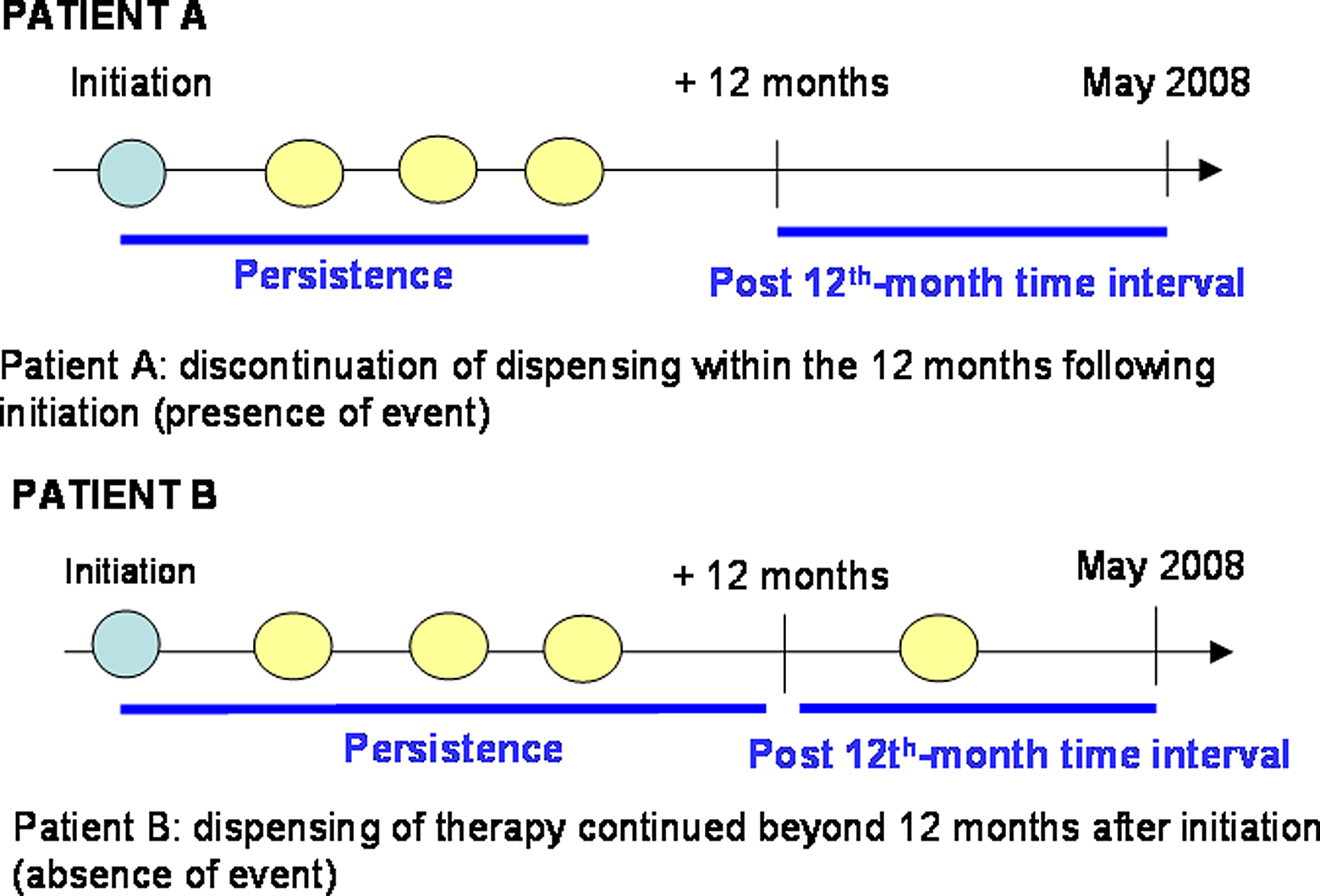
Definition of the 12-month persistence.
Twelve-month persistence to tiotropium was studied according to gender, age, long-term disease status, the number of other respiratory drugs prescribed with tiotropium at initiation and the speciality of the physician who initiated therapy.
Failure to achieve 12 months persistence was the event studied. Persistence interval was defined as the interval from tiotropium initiation until the date of the last dispensation or the occurrence of a censoring event, otherwise until the 365th day following initiation, whichever came first (Figure 1). Log-rank tests were used for the univariate analyses and Cox proportional hazard model for multivariate analyses. Multivariate model was systematically adjusted for age and gender. The time of treatment initiation was also included in the model. Other potential cofactors were included if they showed a statistically significant association in univariate analyses (p < 0.10).
Percentages of days of tiotropium supply during the first 12 months following initiation (persistent patients)
The percentage of days of tiotropium supply during the first 12 months following initiation was computed amongst persistent patients (patient B, Figure 1), based on the assumption of the standard dosing of one daily capsule. The aim was to verify whether temporary interruptions of therapy occurred during the first 12 months in this subgroup. The characteristics of persistent patients with less than 80% of days covered by tiotropium supply during the first 12 months were also examined, which corresponds to an usual cut-off value when studying adherence in pharmacoepidemiology
Results
We identified 1147 patients newly treated with tiotropium (mean age = 68 years, 33% females) who met inclusion criteria. Long-term disease status was common for nearly three quarters of patients. Tiotropium was prescribed at initiation with one or more other respiratory drugs for two out of three patients (Table 1).
Description of the 1147 newly treated patients.
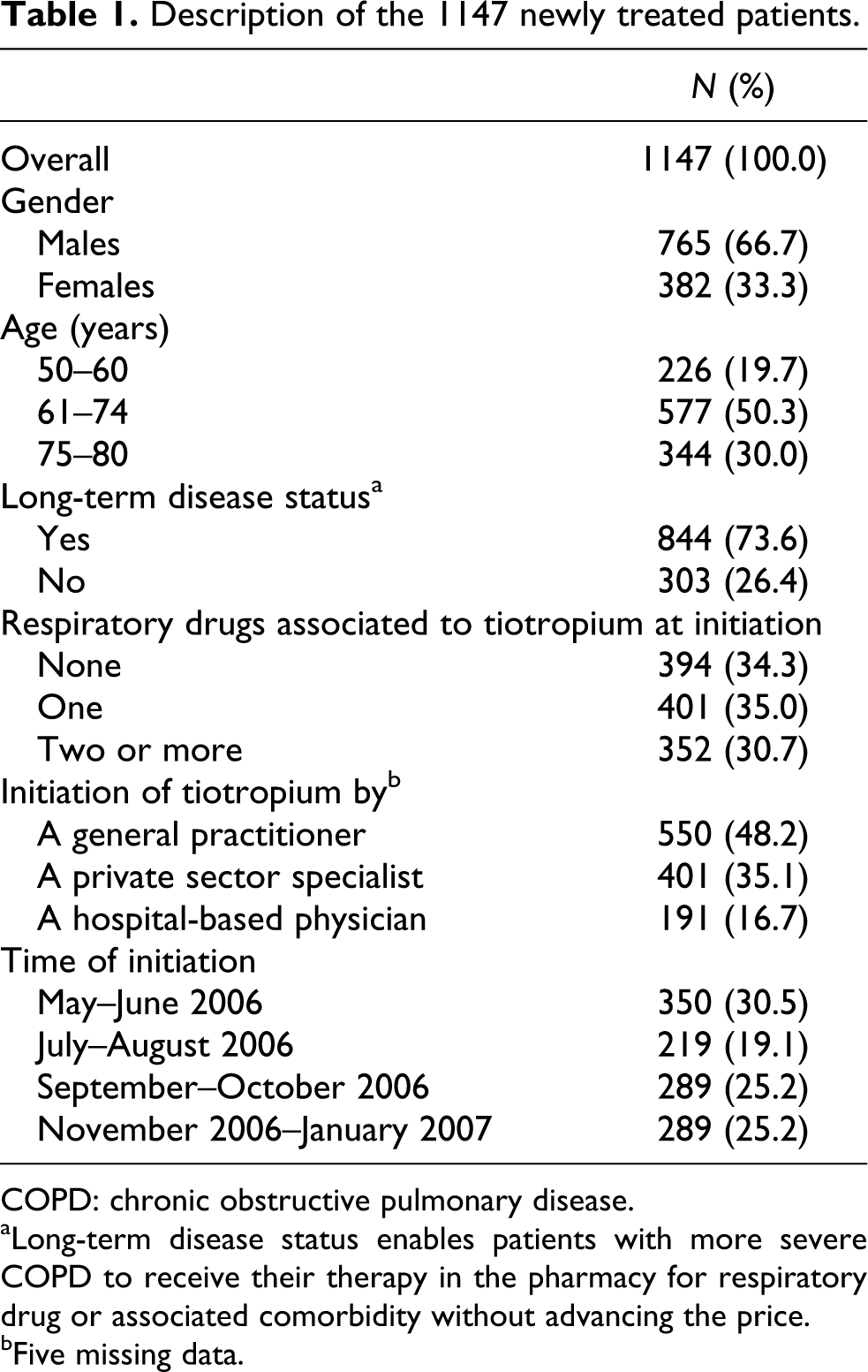
COPD: chronic obstructive pulmonary disease.
aLong-term disease status enables patients with more severe COPD to receive their therapy in the pharmacy for respiratory drug or associated comorbidity without advancing the price.
bFive missing data.
Twelve-month persistence to tiotropium
About 64% of the patients remained on tiotropium during the 12 months following initiation (Figure 2). Percentage of deaths during this period was 5.4%.

A 12-month persistence to tiotropium: Occurrence of any discontinuation of therapy within 12 months following initiation (n = 1147).
Figure 2 shows that a noticeable proportion of patients had only one dispensation of tiotropium (10.7%). These patients with only one dispensation of tiotropium were more often found amongst females (14.9% vs. 8.6%, p = 0.001) and patients without any long-term disease status (16.5% vs. 8.6%, p = 0.0002). They were also numerous when tiotropium was initiated by a general practitioner (14.4% vs. 7.3%, p = 0.0001), and when tiotropium was initiated without any other drugs (13.7% vs. 9.2% p = 0.02).
Univariate correlates of 12-month persistence to tiotropium
Higher 12-month persistence to tiotropium was observed in males and in patients with a long-term disease status. Similarly, patients were more persistent when tiotropium was initiated by a private sector specialist or a hospital-based physician, and when at least one other respiratory drug was also prescribed (Table 2). Conversely, no significant difference was observed with other factors.
Crude and adjusted HRs for discontinuation of tiotropium within 12 months following initiation.
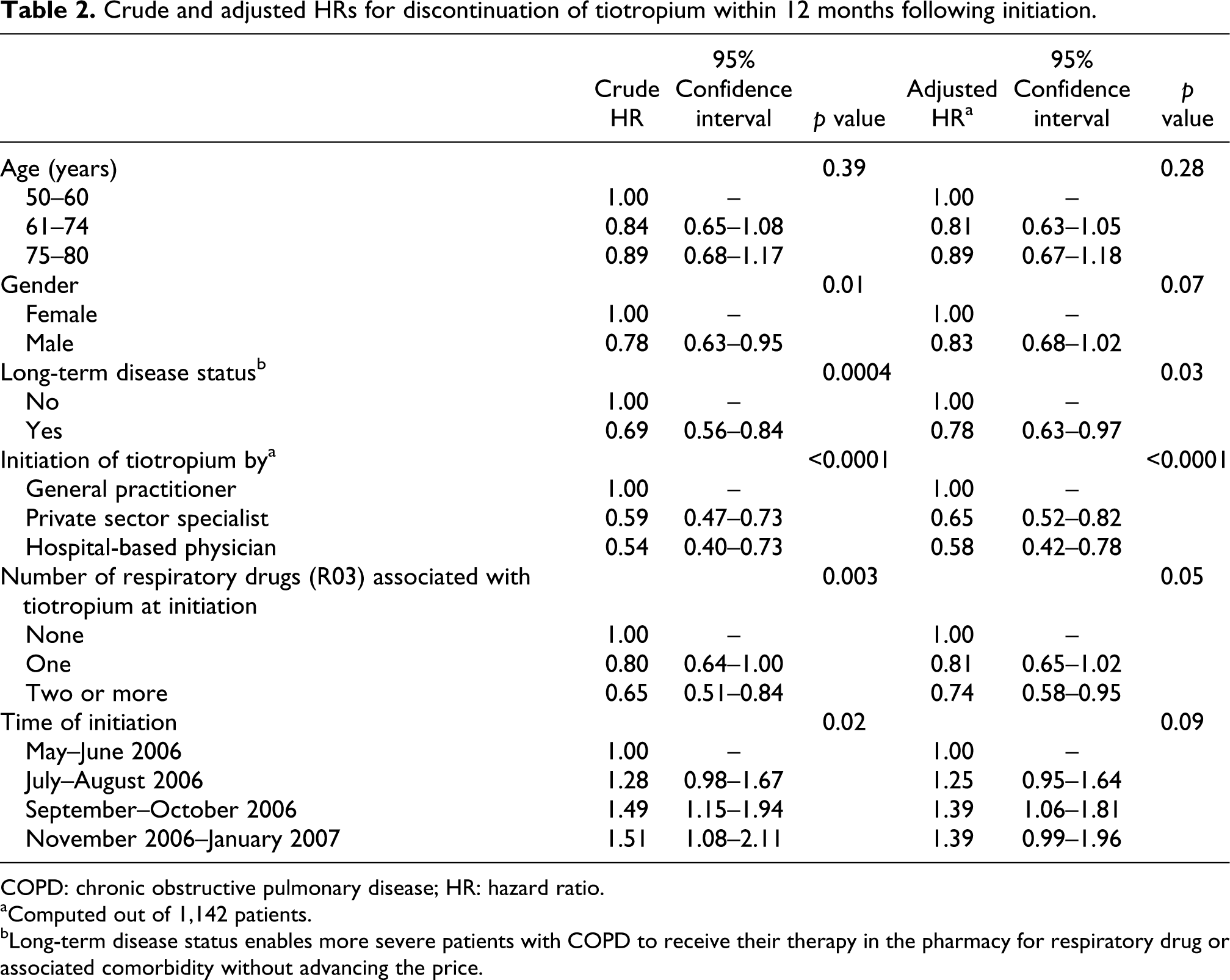
COPD: chronic obstructive pulmonary disease; HR: hazard ratio.
aComputed out of 1,142 patients.
bLong-term disease status enables more severe patients with COPD to receive their therapy in the pharmacy for respiratory drug or associated comorbidity without advancing the price.
Multivariate analyses
Cox proportional hazard multivariate model confirmed most univariate analyses. A better persistence was observed in case of long-term disease status and when more than one respiratory drug was prescribed with tiotropium at initiation. Furthermore, initiation of tiotropium by a private sector specialist or a hospital-based physician was associated with improved persistence (Table 2).
Dispensing adherence in persistent patients: percentages of days of tiotropium supply during the first 12 months following initiation
The median percentage of days’ supply of tiotropium in the 365 days following initiation covered by tiotropium was 89% amongst the 732 persistent patients, noticeable interindividual variations were observed (25th–75th percentiles: 57%–99%). Days’ supply exceeded 100% in about 20% of patients, suggesting an overlap of tiotropium dispensations for these patients.
Out of 10 patients, nearly four had less than 80% of days covered by the dispensing of tiotropium in the 365-day period. In these patients, tiotropium therapy was more likely to have been initiated by a general practitioner, while no other significant characteristics emerged (Table 3).
Factors associated with inadequate percentage of days covered by tiotropium (<80%) during the 12 months following initiation amongst the 732 persistent patients.

Discussion
About 64% of patients remained under tiotropium during 12 months following initiation, while about 10% had a single dispensing. As a rule, 12-month persistence to tiotropium tended to be higher in case of higher COPD severity, as assessed from long-term disease status, burden of therapy or initiation by a private sector specialist or a hospital-based physician.
Direct comparisons of our 12-month persistence rate to tiotropium with other studies are complex, given differences in definitions of adherence. Nonetheless, in Cramer et al.’s study, 53% of patients continued tiotropium 12 months following initiation. 8 A lower rate was observed by Breekveldt-Postma et al. for 12-month persistence (37%), even though this proportion increased to 61% in the cases of prior hospital admissions. 7 Our data also suggest that despite a high median percentage of days covered by tiotropium (89%), temporary interruptions of tiotropium dispensation were not exceptional amongst persistent patients, as measured by the proportion of the 12-month period covered by dispensations, notably when therapy was initiated in primary care (Table 3).
Patients with long-term disease status showed a better persistence (Table 2). Such patients are supposed to have more severe disease for respiratory symptoms or associated comorbid diagnoses. Given their higher level of severity, they might be more aware of the seriousness of their condition and so be more involved in the management of their disease. Additionally, in the absence of long-term disease status or any complementary insurance, French patients have to pay part of their medication costs out-of-pocket. Hence, this status for respiratory diseases could remove a potential economical barrier to adherence for some patients with low income and without complementary insurance.
Surprisingly, 12-month persistence increased with the number of respiratory drugs prescribed or filled with tiotropium (Table 2). As a rule, this finding does not agree with other studies where adherence declined with more complex regimens. 10 In a previous COPD study, we did not find any relationship between the burden of therapy and patients’ declared adherence. 11 In this sample, the presence of coprescribed respiratory drugs at the initiation of tiotropium must probably be considered as a marker of severity, and a better adherence could be explained by increased symptoms, as already emphasised.
Our findings suggest that the patients with more severe COPD had a better persistence. Previous studies have shown improved adherence in patients with COPD with higher disease severity as measured by forced expiratory volume in 1second (FEV1), 12 or use of oral corticosteroids. 7 Moreover, patients with severe COPD may better perceive the seriousness of their condition and the necessity of regular use of respiratory drugs, more so if they feel some benefits from therapy. Unlike asymptomatic chronic diseases like dyslipidemia, patients with COPD typically experience daily symptoms.
Patients who were initiated with tiotropium by a private sector specialist or a hospital-based physician were more likely to have a better persistence to tiotropium. Similarly, these patients had a better coverage of therapy during the 365 days following initiation (Table 3). As in other studies, 10,11,13 better adherence has been observed when treatment was prescribed by a private sector specialist when compared with a general practitioner. Patients managed in respiratory medicine or hospitals may have more severe disease even though this was not supported by some authors. 14 Adherence has been shown to improve when patients believe that daily health and activities are affected by their disease, or whether they anticipate potentially serious consequences resulting from nonadherence. 10 The quality of communication between patients and caregivers has been shown to improve the adherence, 15,16 by improving patients’ understanding of faith in therapy. 15 As a rule, specialists are presumed to spend more time than general practitioners in discussing respiratory diseases with patients. Interestingly, a more efficient use of inhaler devices has also been described amongst patients with COPD treated by specialists. 14
Patients who received tiotropium immediately after launch tended to be more persistent than those with a later initiation, despite no significant difference in multivariate analyses (Table 2). These patients with early initiation might be poor responders to former respiratory drug classes and more inclined to use this new drug regularly, at least during the first 12 months of therapy, all the more so as this new therapy was long awaited amongst the local patients with COPD. Patients with a unique dispensing of tiotropium tended to have less severe COPD, and therapy was more likely to have been initiated in primary care.
The present study did not show any difference according to patient’s age. Yet, increasing age has been associated with a better compliance in many studies conducted in COPD, 10,12,17 or in asthma, 16,18 Nevertheless, others did not confirm these findings. 13,19 Increasing age may result in a greater number of comorbid conditions, polypharmacy and cognitive decline, which may hinder adherence to treatment 10,20 in this population of elderly patients. Additional studies are needed to explore the impact of age on the adherence to respiratory drugs in patients with COPD .
The increased persistence that was observed in males in univariate analyses was not confirmed in multivariate analyses (Table 2). A slightly better adherence to combined fluticasone–salmeterol has been observed in males in a recent study, 21 although this finding was not confirmed by other authors, 13,19,22
Our study had some limitations. Databases comprise limited data on patients’ personal characteristics. Similarly, results of clinical and spirometric investigations were not available, limiting our investigation on the impact of disease severity. However, long-term disease status is attributed based on the presence of clinical severity criteria. Then, a number of respiratory drugs associated with tiotropium and initiation by specialists or hospital physician could indirectly reflect a higher disease severity.
As tiotropium has a specific indication for COPD, it can be assumed that our sample consisted of patients with COPD, although this could not be formally verified given the absence of diagnoses in the database.
Interruptions of tiotropium were assumed to be due only to patients. Nevertheless, cessation of therapy could also be decided by physicians, notably when patients did not tolerate the drug or when the drug did not deliver expected benefits. We did not know the reasons of cessation in our study. Additionally, patients’ actual use of dispensed therapy remains unknown. Another limit was that some severe patients with a prolonged hospital admission following tiotropium initiation may have received their therapy in hospital or interrupted it. As drugs dispensed to patients during hospital stays are not recorded in the database, lower adherence rates could be falsely observed amongst such patients. Nevertheless, such potential bias may not have affected our conclusions regarding persistence status. First, only prolonged admissions could have impaired our findings, as only one dispensing of tiotropium beyond the 12th month following initiation was sufficient to qualify a patient as persistent. Then, as mentioned above, our results and those of other studies are suggestive of a better adherence in patients with more severe COPD, who are precisely more at risk of prolonged hospitalisations. Finally, only short-term adherence was examined and other dimensions of adherence such as actual use of therapy by patients could not be explored and the causes of deaths were not documented in the database.
Our data have several implications. They suggest that adherence to tiotropium of patients with less severe COPD could be improved, although more severe patients tended to adhere better. The lower adherence amongst less severe patients is nonetheless of concern. Taken together, our results are consistent with other observational studies. 7,8 It should be underlined that this finding is not specific to tiotropium. Higher adherence levels in COPD were commonly observed for tiotropium compared with other respiratory drugs, 7,8,23 Nonetheless, the reasons for this inadequate adherence should be investigated in this subpopulation of patients with less severe COPD. The search for potential obstacles to the regular use of tiotropium would help optimising COPD management.
Conclusion
In real world settings, adherence to tiotropium can be improved in patients with less severe COPD. Our data also suggest a better adherence when disease was initiated by the respiratory physicians. The quality of communication and information regarding disease and therapy are the cornerstones of effective management. Further studies are needed to improve our understanding of the barriers to adherence in COPD.
Footnotes
Acknowledgment
The authors thank Mrs Ambrosi for her precious assistance in accessing the data. The data are graciously provided by the Regional Health Insurance Organization from Rhone-Alpes French Region.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
The authors declared no conflicts of interest.