
Abstract
American Society of Anesthesiologists (ASA) has introduced a simple tool to assess the perioperative risk of surgery/anesthesia in patients with obstructive sleep apnea (OSA). We compared the surgical outcomes in patients at high risk of OSA with the matched controls. This was a case–control study conducted on 3593 surgical patients receiving a general anesthesia at a single institution. On the basis of a preoperative OSA scoring system using the ASA checklist, patients were classified as high-risk OSA (HR-OSA) or low-risk OSA (LR-OSA) groups. Apnea/hypopnea index of >5 h−1 during a formal preoperative sleep study was used to confirm or rule out the diagnosis of OSA. Receiver operating characteristic curves were plotted to determine the predictive values as well as sensitivity and specificity of the ASA tool in predicting HR-OSA. The HR-OSA group was matched with the patients in LR-OSA using the propensity scoring and logistic regression. Patients were analyzed for premorbid conditions, intraoperative course and postoperative events using cross tabulation, logistic regression model and paired t test. The development of a composite respiratory complication in the postoperative period was considered as the primary end point. The ASA risk tool was found to have 95.1% sensitivity and 52.2% specificity. At a prevalence of 10%, the negative predictive value was 98.5%. Of the 3593 patients, 306 were identified as HR-OSA. The HR-OSA group was found to have a higher incidence of hypertension and diabetes preoperatively when compared with LR-OSA. Postoperatively, the HR-OSA group had higher incidence of hypoxia, reintubation, postoperative use of continuous positive airway pressure and a longer stay in the recovery room. The ASA checklist offers a highly sensitive tool to identify the patients at a higher risk of OSA during the perioperative period. Patients at HR-OSA have a higher incidence of adverse events in the postoperative period when compared with those with LR-OSA.
Introduction
Obstructive sleep apnea (OSA) is a clinical syndrome characterized by repeated occlusions of upper airway during sleep, resulting in sleep fragmentation and nocturnal hypoxemia. Symptomatic OSA affects approximately 2% and 4% of women and men, respectively, but the overall prevalence of the sleep disorder was estimated to be 9% for women and 24% for men between the ages of 30 and 60 years. 1 In a survey study in elective surgical patients using Berlin questionnaire, 2 24% patients were found to be at risk of OSA. 3 Due to the associated airway pathology and depressive effects of anesthetic agents on respiration and pharyngeal muscle tone, patients with OSA are at a high risk of respiratory complications. 4 In addition, airway management of these patients has been shown to be challenging for the anesthesiologists in view of difficulty in securing the airway. 5,6
Of concern is the fact that the majority of surgical patients with OSA are undiagnosed. There are various screening tools for the diagnosis of OSA in surgical patients, but their validity for use in perioperative setting is still under question. The Berlin questionnaire is a widely used tool for the detection of OSA. 2,3,7 The American Society of Anesthesiologists (ASA) checklist 8 is a consensus of the task force to identify high-risk patients. This checklist consists of 12 items that include predisposing physical characteristics, history of apparent airway obstruction during sleep, daytime somnolence, snoring, tiredness, observed stop breathing and blood pressure. STOP questionnaire 9 is also a concise and easy-to-use tool to identify patients at risk of OSA.
An alternative scoring model combining both the STOP questionnaire and BANG 10,11 (body mass index (BMI), age, neck circumference and gender) further improves the sensitivity. Diagnostic sleep studies, however, remain the gold standard for the diagnosis of OSA, 12 but can be inconvenient and time consuming in the perioperative setting. Patients at high risk of OSA may not actually carry a diagnosis of OSA due to the lack of confirming sleep study and sometimes the subtle symptoms, which the patients may not recognize.
The primary objective of this study was to compare the surgical outcomes in patients at high risk of OSA with the control patients undergoing similar surgeries. We hypothesized that the tool developed by the ASAs’ task force 8 reliably predicts the high-risk OSA (HR-OSA), and thus, the incidence of postoperative complications was higher among the high-risk patients.
Methods
We conducted a retrospective case–control study on patients who underwent surgery during the period from September 2007 to September 2009. The study was reviewed and approved by the Institutional Review Board Committee at the VA Western New York Healthcare System (VAWNYHCS), Buffalo, New York. The approval number was 2010-00704.
Patient screening and risk assessment
All the ambulatory patients between the ages of 18 and 80 years arriving for an outpatient surgery or the same day admission and who received general anesthesia were included. Patients with regional anesthesia or more than one surgery during this period were excluded. At our institution, for the preoperative evaluation of all the patients, we incorporated a preoperative protocol for annotating the OSA history with the aid of a questionnaire based on the ASA checklist (Appendix A). This preoperative evaluation was carried out in a preoperative clinic by the anesthesia nurse practitioners or an anesthesiologist, routinely for the elective cases. In case of emergency surgeries, the anesthesia residents or the anesthesiologists did the evaluation before surgery. On the basis of ASA checklist, the patients were assigned a risk score. Patients with OSA risk score of ≥5 were identified as HR-OSA and those with a score <5 were categorized as low-risk OSA (LR-OSA). If a sleep study (polysomnography) had been performed within the past 5 years, the results were recorded and compared with the ASA checklist scoring system. Additionally, another sleep study was performed in symptomatic patients with recent weight gain. The diagnosis of OSA was confirmed if a patient had an apnea/hypopnea index (AHI) of >5 h−1. Patients who had a positive sleep study were recommended the continuous positive airway pressure (CPAP) therapy, but the compliance with this recommendation could not be guaranteed. The patients already prescribed CPAP were recommended to use their CPAP device during their hospital stay. The respiratory therapist guaranteed their compliance.
Clinical data were collected by a detailed review of the preexisting preoperative and clinical records by the members of the research team (anesthesia resident, a research associate and a trained anesthesiologist) from the Computerized Patient Record System database used at the VAWNYHCS. Demographic data, ASA physical status (ASA-PS), airway assessment on the basis of Mallampati et al. classification 13 and existing comorbidities were obtained. From the preoperative data, patients at HR-OSA and LR-OSA were also identified. Intraoperative data include type, invasiveness and duration of the surgical procedure, type of anesthesia, type of airway method used and the amount of opioids administered.
A composite respiratory complication includes hypoxia, defined as one or more incidences of pulse oximetry value of ≤90% on 2–3 L min−1 by nasal cannula, in which reintubation and requirement of mechanical ventilation during postoperative period were considered as the primary end points. Additionally, development of new onset atrial fibrillation for at least 3 min; cardiac ischemia defined as ST-T wave changes in the postoperative period; hemodynamic instability defined as systolic blood pressure <90 mm Hg or diastolic blood pressure <50 mm Hg or a change >20% from the baseline; and myocardial infarction, evident by electrocardiogram changes and angina and confirmed by elevation of cardiac enzymes, or evidence of cerebrovascular accident on the basis of a new onset of neurological deficit were recorded. Type of surgery was included in the questionnaire for calculating the OSA risk and hence was already considered for the classification of patients. Since there were significantly more patients in the ASA class 3/4 among the HR-OSA group compared with the LR-OSA group (p = 0.002), ASA-PS was included as one the matching variables.
Duration of postanesthesia care unit (PACU), 1hospital stay and readmission rate within 24 h of discharge from the ambulatory surgery unit were used as the secondary outcome variables. The patients were discharged from the PACU when they met the modified Aldrete scoring criteria. 14 The patients who were directly transferred to the intensive care unit (ICU) for recovery were excluded from the analysis for the duration of PACU stay but were included for other variables. The anesthesia providers performing the preoperative evaluation and assigning the risk score were blinded to the clinical outcome.
Data measurement and statistical analysis
The preoperative comorbidities, intraoperative and postoperative data were entered into the Microsoft Excel Spreadsheet 2007 Inc. The NCSS Version 2007 (NCSS, LLC., Kaysville, Utah, USA) software was used for the analysis. All continuous variables were expressed as mean ± SD and the categorical variables were expressed as the percentage of patients in the data. Receiver operating characteristic curves were plotted to determine the predictive values, sensitivity and specificity of the ASA tool in predicting HR-OSA, using sleep studies with an AHI of >5 as the gold standard diagnostic test. The complication rate was compared between the two groups and a primary outcome variable was defined as the occurrence of composite postoperative respiratory event. All the factors that had p < 0.1 on the basis of univariate analysis, age, airway surgery and ASA class were included in calculating the propensity score. HR-OSA patients were matched 1:1 with LR-OSA patients using the propensity scores. Statistical analyses were performed using Chi square test for categorical variables, and two-sample paired t test were performed for continuous variables before and after data matching. Binary logistic regression was used to find the predictive values of OSA in certain comorbid conditions. Hazard ratio was calculated for all comorbidities. A p < 0.05 was considered statistically significant.
Results
Of the 3593 patients studied, on the basis of patient characteristics, 306 patients were identified as HR-OSA and were compared with 3286 unmatched patients in the LR-OSA group. After matching, HR-OSA group was compared with an equal size of matched LR-OSA controls. There was no significant difference between the groups on the basis of gender, age or race (Table 1).
Patient demographicsa

HR: high risk; LR: low risk; CPAP: continuous positive airway pressure; ASA: American Society of Anesthesiologists; PS-1: physical status 1 – a normal healthy patient
a Data are presented as mean ± SD or N (%), as appropriate.
b Others indicate Asians, Pacific islanders and Native Indians.
c Airway indicates Mallampati classification of airway into four classes 13 .
In the HR-OSA group, 140 of 306 patients had an AHI of >5 h−1 compared with 32 of 306 matched LR-OSA patients with an AHI of >5 h−1. The area under the curve was measured as 0.8 ± 0.1 (p < 0.01). ASA risk assessment had 95.1% sensitivity and 52.2% specificity. At a prevalence of 10%, the positive predictive value of this tool was 19%, while the negative predictive value was 98.5% (Figure 1).

ROC curves were plotted to determine the predictive values, sensitivity and specificity of the ASA tool in predicting HR-OSA and its related complications. The area under the curve was measured as 0.8 ± 0.1(p < 0.01). ASA risk tool was found to have 95.1% sensitivity and 52.2% specificity. At a prevalence of 10%, the positive predictive value of this tool was 19%, while the negative predictive value was 98.5%. ROC: receiver operating characteristics; ASA: American Society of Anesthesiologists; HR-OSA: high risk obstructive sleep apnea.
HR-OSA patients had a higher prevalence of comorbid conditions, that is, coronary artery disease, hypertension and diabetes mellitus when compared with the LR-OSA group (Figure 2). The incidence of hypertension was 80.4% versus 68.6%, (p < 0.001) and diabetes mellitus was 44.1% versus 27.1%, (p < 0.001) in HR-OSA group when compared with the LR-OSA group (Table 2), respectively. However, no significant increase in the incidence of chronic obstructive pulmonary disease (COPD) among the HR-OSA patients was found. There were more patients with higher Mallampati airway class 13 (class 3 and 4) in the HR-OSA group compared with the LR-OSA group (p < 0.01). Intraoperative airway management was more likely to be attained by the tracheal intubation in the HR-OSA group than the matched LR-OSA group (73.4% vs. 62.2%; Table 3). Postoperatively, the patients in the HR-OSA group were found to have significantly higher incidence of hypoxia (16.8% vs. 10.2%) and more frequently in need of tracheal reintubation (4.9% vs. 0.9%) when compared with those in the matched LR-OSA controls (Table 4).
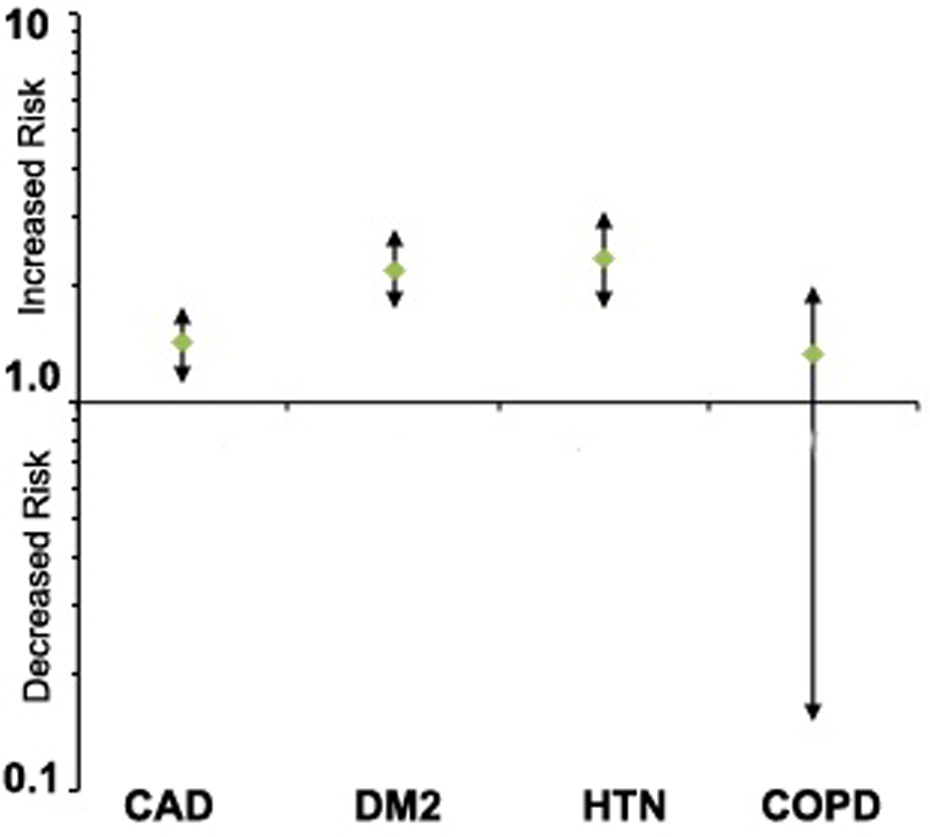
Binary logistic regression analysis for predictive value of OSA for different comorbidities with odd ratios and 95% confidence interval of OSA patients versus those with no OSA risk. CAD: coronary artery disease; CKD: chronic kidney disease; COPD: chronic obstructive pulmonary disease, DM: diabetes mellitus; OSA: obstructive sleep apnea.
Preoperative comorbiditiesa
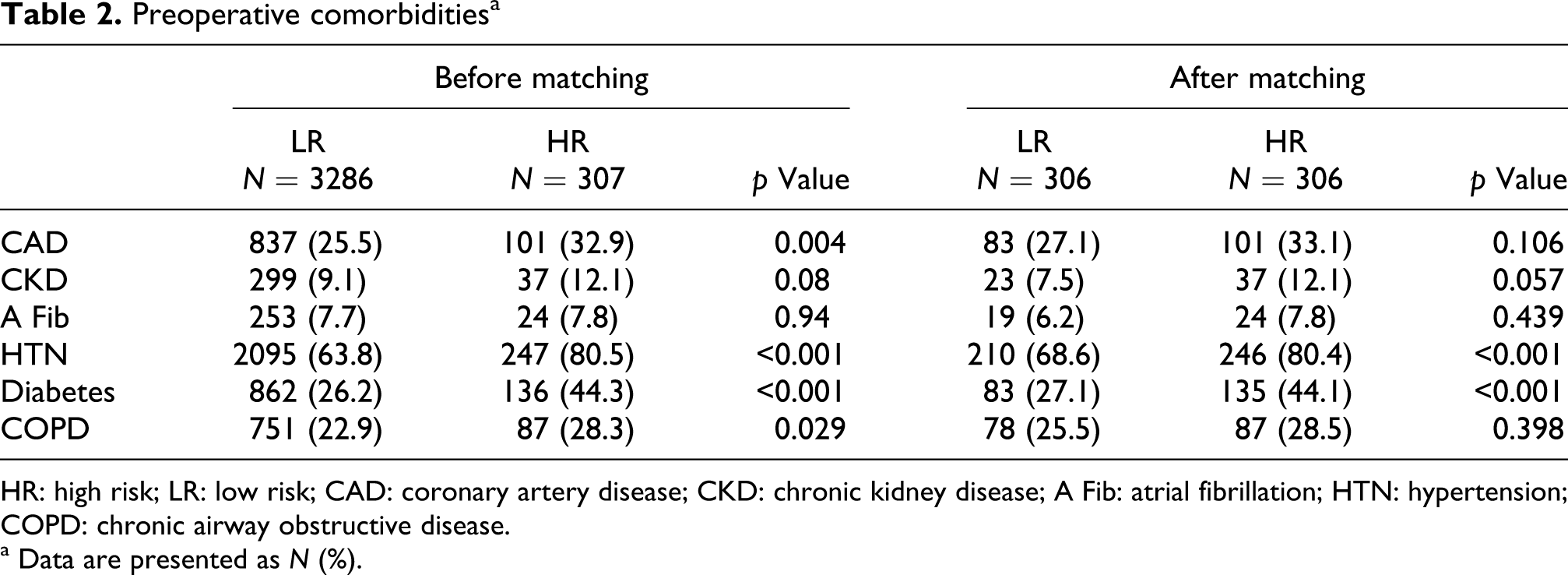
HR: high risk; LR: low risk; CAD: coronary artery disease; CKD: chronic kidney disease; A Fib: atrial fibrillation; HTN: hypertension; COPD: chronic airway obstructive disease.
a Data are presented as N (%).
Airway methoda

LR: low risk; HR: high risk; ET: endotracheal; LMA: laryngeal mask airway.
a Data are presented as N (%).
b In the unmatched data, more patients received tracheal intubation; this could be due to the assumption that anesthesiologists have a tendency for intubation in patients with anticipated difficult airway.
Postoperative complicationsa

HR: high risk; LR: low risk; CPAP: continuous positive airway pressure; MI: myocardial infarction; A fib: atrial fibrillation; CVA: cerebrovascular accident; ICU: intensive care unit; CMPEVENT: composite respiratory event; NC: not calculated.
a Data presented as mean ± SD or N (%), as appropriate.
b statistically significant.
Overall, the incidence of a composite adverse event was 25.4% in the HR-OSA group and 17.4% in the LR-OSA matched controls (p < 0.01). Multivariate analysis was carried out using the composite respiratory event as the primary outcome. We found that HR-OSA is an independent risk factor for the postoperative respiratory event and increases the risk by 50%. Other than the OSA risk, the presence of COPDs was also identified as an independent factor for the development of hypoxia, postoperatively (Figure 3). Fifteen patients from the HR-OSA group were reintubated, while only two patients from the LR-OSA group were reintubated in the postoperative period (4.9% vs. 0.7%, p < 0.001) and transferred to the ICU (Table 3). Additionally, there were more patients in the HR-OSA group who needed postoperative use of CPAP (7.2% vs. 1.3%, p = 0.0003).
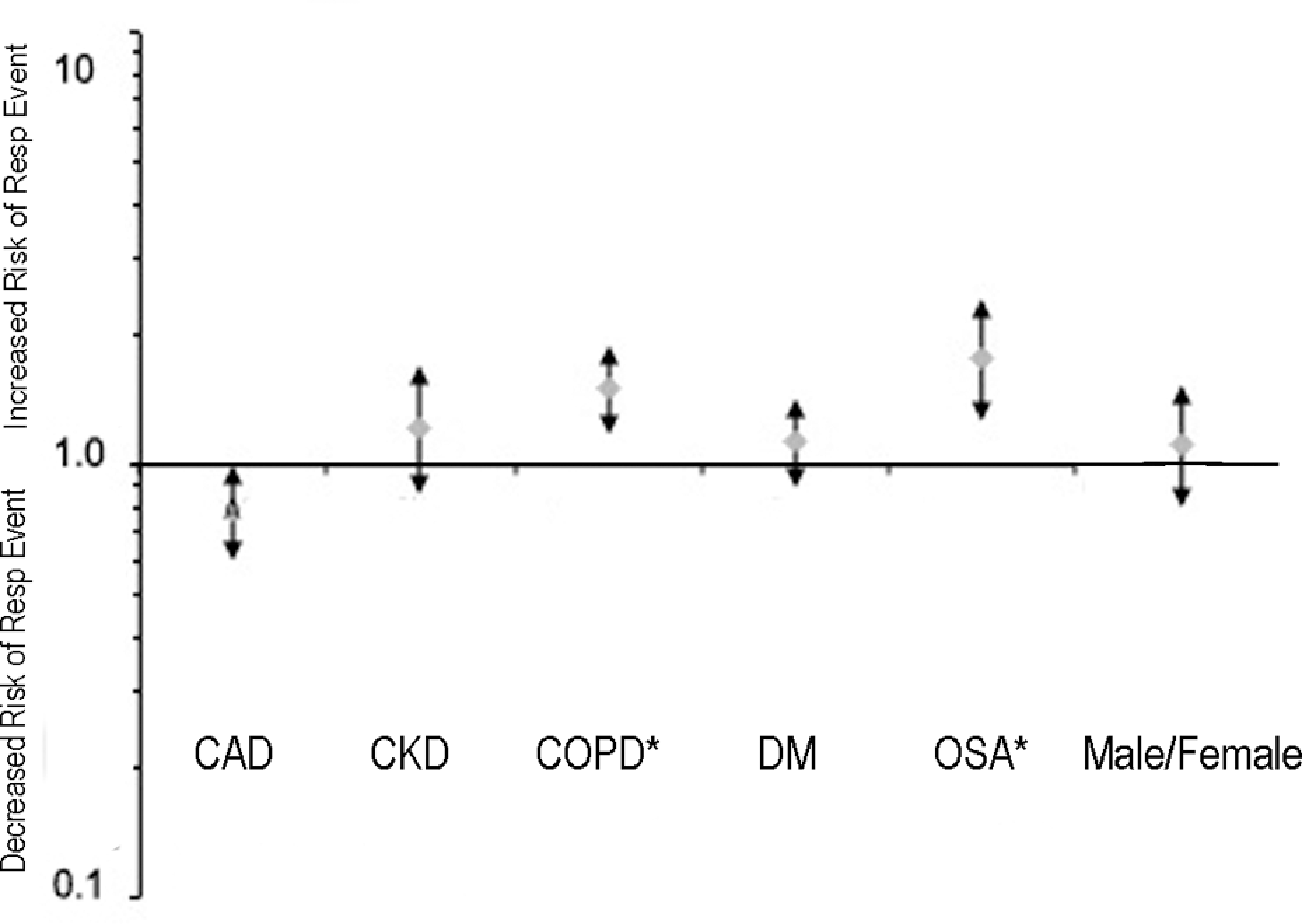
Hazard risk ratio for postoperative hypoxia with 95% confidence intervals. Note that OSA risk and COPD are independent factors for a composite respiratory event (hypoxia, hypoventilation, reintubation and mechanical ventilation) but not any other comorbidity. CAD: coronary artery disease, CKD: chronic kidney disease, COPD: chronic obstructive pulmonary disease, DM: diabetes mellitus; OSA: obstructive sleep apnea.
Patients in the HR-OSA group stayed in the PACU for longer duration (113 ± 54 min) when compared with their matched cohort in the LR-OSA group (99 ± 52 min, p < 0.01). The likelihood of hospital admission after surgery was similar in both the groups. There was no difference between the LR-OSA group and the HR-OSA group in overall mortality, admission to hospital and the overall lengths of hospital stay (11.3 ± 18.6 days vs. 13.7 ± 35.8 days).
Discussion
Our study demonstrates that the ASA checklist offers a highly sensitive tool to identify the patients at high risk of OSA during the perioperative period. This tool, however, has a relatively low specificity that may lead to false positive results. Our study showed that high perioperative risk OSA translates into a greater incidence of adverse events such as hypoxia in the postoperative period.
Additionally, the incidence of reintubation was higher in HR-OSA group. These patients were more likely to have a difficult airway, which has been reported previously by other studies. 6 This observation is probably due to the associated body habitus and other physical characteristics. These reports, however, failed to show any association with increased incidence of reintubation. In the unmatched data, more patients received tracheal intubation; this could be due to the assumption that anesthesiologists have a tendency for intubation in patients with an anticipated difficult airway.
We found that hypertension, diabetes mellitus and coronary artery diseases were more frequent among the OSA population, and overall, the ASA-PS was higher in OSA population due to the presence of these comorbidities; therefore, we could not include these in our matching criteria. Also with ASA-PS as a matching criterion, we collectively included the individual comorbidity variables. We also could not match for BMI, as it was obviously higher in patients at high risk of OSA. This is consistent with the literature as OSA has been linked to various comorbidities and BMI tends to be higher in the OSA risk patients.
There were two retrospective reviews on postoperative complications in patients with an established diagnosis of OSA. In a study by Liao and colleagues on known OSA patients who underwent elective surgery other than airway surgery, they found that patients diagnosed with OSA have an increased incidence of oxygen desaturation. 15 Gupta et al. studied patients with OSA undergoing orthopedic surgeries, and found that OSA patients had higher incidence of respiratory and cardiac complications in the postoperative period. The length of hospital stay and unplanned ICU admissions were also higher. 16 We were unable to demonstrate such an association among our patients. Gupta and colleagues demonstrated the length of stay at 6.8 ± 2.8 days and 5.1 ± 4.1 days for the OSA and the control groups, respectively. We found no difference in the length of stay between the HR-OSA and the LR-OSA groups. The study by Gupta et al. was performed on a smaller cohort of patients who only underwent orthopedic surgeries, whereas in our study we included all types of surgery including the airway. The study by Gupta et al. was a fully retrospective study, whereas we performed a retrospective review on prospectively collected data. These may account for a difference in the results attained.
Both the studies reported that the oxygen desaturation is the most common respiratory complication in the postoperative period. Sabers et al. showed that in patients undergoing nonairway surgeries, the diagnosis of OSA was not a risk factor for the unplanned admission. 17 Since this study included less invasive ambulatory procedures, projection of the results to the general surgical procedures cannot be carried out. In this study, we found that the patients at HR-OSA were more likely to be admitted as inpatients when compared with patients at LR-OSA; however, after matching for comorbid conditions, this observation was not significant.
Our study also supports the findings of Chung et al., in which they found higher correlation between the ASA checklist and the patients at high risk of OSA. 7 However, the majority of previous studies including Chung et al. study enrolled the patients with a confirmed diagnosis of OSA, 7,15,16 whereas we used the preoperative risk assessment tool developed by the ASA to identify the relative risk of OSA during perioperative period. We also observed that higher number of patients in the HR-OSA group received CPAP in the postoperative period. Considering the fact that a higher number of HR-OSA patients were using CPAP prior to their scheduled surgery, this observation was not surprising.
An important limitation was the predominance of male gender among the veterans. Preexisting literature suggests that OSA is a more prevalent condition in males when compared with that of females. 18 This gender distribution may have contributed to higher number of HR-OSA patients in our study. This was a retrospective observational study and hence there remain many limitations in the retrospective chart review like incomplete or missing documentation, poorly recorded information in certain cases and also difficulty to ascertain the cause and effect relationship. Another important limitation could be the fact that the anesthesiologist was aware of the HR-OSA patients preoperatively and therefore there is always a chance for treatment bias in favor of the HR-OSA patients regarding the postoperative CPAP use and increased duration of PACU stay. From the HR group, a higher number was already receiving CPAP in the preoperative period and therefore continued in the postoperative period.
We conclude that the patients with OSA have higher incidence of perioperative adverse events, which implies that we need to develop specific management strategies for OSA patients in the perioperative period to reduce the economic burden on the health care system. It is not feasible in the perioperative period to get sleep studies done on every patient due to the time constraints and inconvenience to the patients. In this setting, screening the patients at the time of preoperative visit, using simple questionnaires as suggested by the ASA practice guidelines can help identify the high risk patients and to take up specific measures like early diagnosis and treatment initiation and to reduced intra and postoperative opioid use; alternative analgesic therapies can also be taken beforehand to minimize the adverse perioperative outcomes. More prospective studies on the perioperative complications in OSA patients are needed. Also, the efficacy of CPAP has not been established in the perioperative setting. We speculate that the utilization of CPAP in high-risk patients will likely improve the outcome and are highly warranted.
Footnotes
Appendix A
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.