
Abstract
Negotiated treatment plans are increasingly recommended in asthma clinical care. However, limited data are available to indicate whether this more patient-engaged process results in improved health outcomes. The aim of this study was to determine the associations between the presence of a negotiated treatment plan and the outcomes related to adherence to the medical regimen, symptom control, and health care use. The focus of the study was on women, the subgroup of adult patients, who are most vulnerable for negative asthma outcomes. Data were collected by telephone interview and medical record review from 808 women diagnosed with asthma at baseline, first year, and second year follow-up. Associations were examined between the presence of a negotiated treatment plan at baseline and subsequent asthma outcomes. Women with a negotiated treatment plan reported more adherent to prescribed asthma medicines (odds ratio (OR) = 2.41, 95% confidence interval (CI) = (1.82, 3.19)) and those with a plan and using oral steroids at baseline had less oral steroid use at follow-up (OR = 0.21, 95% CI = (0.05, 0.93)). Women with a negotiated plan also had more days (17%, 95% CI = (8, 27)) and nights (31%, 95% CI = (16, 48)) with symptoms than those without such a plan. No differences in hospitalizations, emergency department visits, or urgent physician office visits were noted between the groups. Patients with higher education levels were more likely to have a negotiated treatment plan. Negotiated treatment plans appear to have achieved greater adherence to prescribed asthma medicines and less need for oral steroids but were not related to fewer symptoms of asthma or reductions in urgent health care use. Additional strategies may be needed to reduce symptom and health services utilization outcomes.
Introduction and problem
Increasing attention in clinical practice is being paid to involving patients in the development of treatment plans that fit their clinical needs and are most manageable for them on a day-to-day basis. 1 –4 The term ‘negotiated treatment plan’ has been used to indicate a type of regimen that is based on patient engagement in decisions leading to the clinician’s recommendations. However, little evidence is available regarding the outcomes of negotiated treatment plans. A classic Cochrane Review showed that asthma education that included written action plans resulted in enhanced clinical status and reduced health care use for adults with asthma. 5 However, the features of a negotiated treatment plan and plans independent of asthma education were not tested in that study. Wilson et al. examined outcomes associated with a patient’s action plan when negotiated with a physician and found better adherence to use of asthma medicines. No differences in quality of life or health care use for asthma were observed. 6 The research presented here examined asthma outcomes regarding medicine use, symptoms, and need for urgent health care services for asthma in a sample of patients who did and did not engage in negotiation with their clinicians to arrive at a treatment plan for the condition. The focus of the study on women is especially important as these patients reflect the highest prevalence of asthma among adults and the highest level of health care use for the condition. 7 The hypothesis was that having a plan the patient, and the physician worked together to derive clinical recommendations that would be associated with higher levels of adherence to the treatment plan, lower levels of asthma symptoms, and less urgent health care use.
Methods
All procedures were approved by the University of Michigan Institutional Review Board.
Sample and data collection
The study enrolled 808 women receiving services at the University of Michigan Health System (UMHS), and they are identified through the UMHS data warehouse (a system wide mechanism to facilitate research and monitor consent). Participants’ physicians were blind to participation of patients in the study. Inclusion criteria were (1) 18 years of age or older; (2) diagnosis of asthma by a UMHS physician; (3) presence of active asthma symptoms in the past 12 months; (4) enrolled as a patient in one of the participating asthma-related clinics; (5) no extenuating medical or mental conditions (i.e. terminal illness and dementia); (6) not pregnant (women who became pregnant during the study continued participation but their data were excluded from analyses); and (7) access to a telephone. A total of 2336 women were sent study invitation letters and refusal postcards during the 3½ year recruitment period. Consent forms were mailed to 997 women who agreed to participate in the study, and ultimately, 808 respondents returned the completed consent forms by mail and provided data at baseline. Data were collected at baseline and 12 and 24 months later by trained telephone interviewers.
Measures
Interview items were developed based on previous work by the authors and others regarding interactions with the physician, medicine use, symptom experience based on National Asthma Education and Prevention Program (NAEPP) Guideline definitions of severity and health care use. 8 –10 Extensive queries were included regarding type and use of asthma medications. To assess the presence of a negotiated treatment plan, women were queried as follows: do you have a treatment plan or asthma care plan that you and your doctor worked together to develop for you to use to adjust your medicines when symptoms change? To evaluate adherence to medication recommendations, women were asked: how often do you take your asthma medications as prescribed by your physician, usually, sometimes, or rarely?
Data analysis
Statistical analyses were performed using the SAS System, version 9.2. Multiple imputation was performed using IVEware, a SAS-based software using a sequential regression approach to impute missing values that occurred from baseline to the follow-up periods. 11
To investigate whether having a negotiated treatment plan contributed to fewer asthma symptoms (annual symptom days and symptom nights) and less health care use (overnight hospitalizations, visits to emergency department, urgent physician visits, and regularly scheduled physician visits), we used the negotiated treatment plan value at baseline as the explanatory variable and symptom and health care use variables at 12-month follow-up as the response variable modeled by Poisson regression (SAS PROC GENMOD). In addition, proportional odds model was used for the multinomial variable of medication adherence, and logistic regression model was used for modeling use of oral steroid (SAS PROC LOGISTIC). We did not use data from all three time points because there was substantial missing information about whether having a negotiated treatment plan at follow-ups (25 and 35% were missing at 12- and 24-month follow-up, respectively). Moreover, having a negotiated treatment plan was a dynamic status that changed throughout the study period; thus, the effect of having a negotiated treatment plan could be hard to define. Adjusted models were used to control any possible confounding factors, including baseline asthma symptoms (frequency and severity), intervention (as some women participated in an asthma program as part of a large clinical trial), and number of major health problems in addition to asthma. 12 Parameter estimates from each multiply imputed data set were combined using the combining rules 13 to obtain point estimates and associated standard errors (SAS PROC MIANALYZE). Type I error rate was set at 0.05. Self-report data regarding use of urgent care for asthma were compared with medical record data for those patients enrolled in the University of Michigan Data Warehouse to verify health care use. Analysis illustrated no difference in results regarding health care use from both the sources of data.
Results
Table 1 illustrates the characteristics of 793 women who reported having and not having a negotiated treatment plan at baseline. In the baseline year, the mean age was 48.05 ± 13.68 years (range 20–91). On average, women were diagnosed with asthma at 29.90 ± 17.21 years old. The majority was overweight or obese, Caucasian, married, and employed. About half of the women (48%) had persistent asthma. Women who had a treatment plan did not differ from those who did not have a treatment plan by these characteristics, except by the number of prescribed medicines used (p < 0.01) and education (p = 0.06). Women with a negotiated treatment plan tended to have more prescribed medications (mean 4.26 ± 2.12) than women who had no such plan (3.12 ± 1.81). A greater proportion of women with a treatment plan appeared to have a higher education level than women without a treatment plan (73 vs. 67%). Among the 793 women, 82 (10%) were prescribed with oral steroid and most of them (N = 58, 71%) had a negotiated treatment plan.
Baseline characteristics of women in this study with asthmaa

aMean ± SD for continuous variables.
bPearson’s chi-square test was performed for Caucasian/white versus non-Caucasian/white.
cHaving college (or above) education.
The status of having a treatment plan on some of the 793 women changed over time, with 50 (6%) women moved from having a negotiated treatment plan to no treatment plan, 117 (15%) women moved from having no negotiated treatment plan to having one, 428 (54%) remained their treatment plan status, and 198 (25%) did not report whether they had a treatment plan during the follow-up period.
Medication adherence
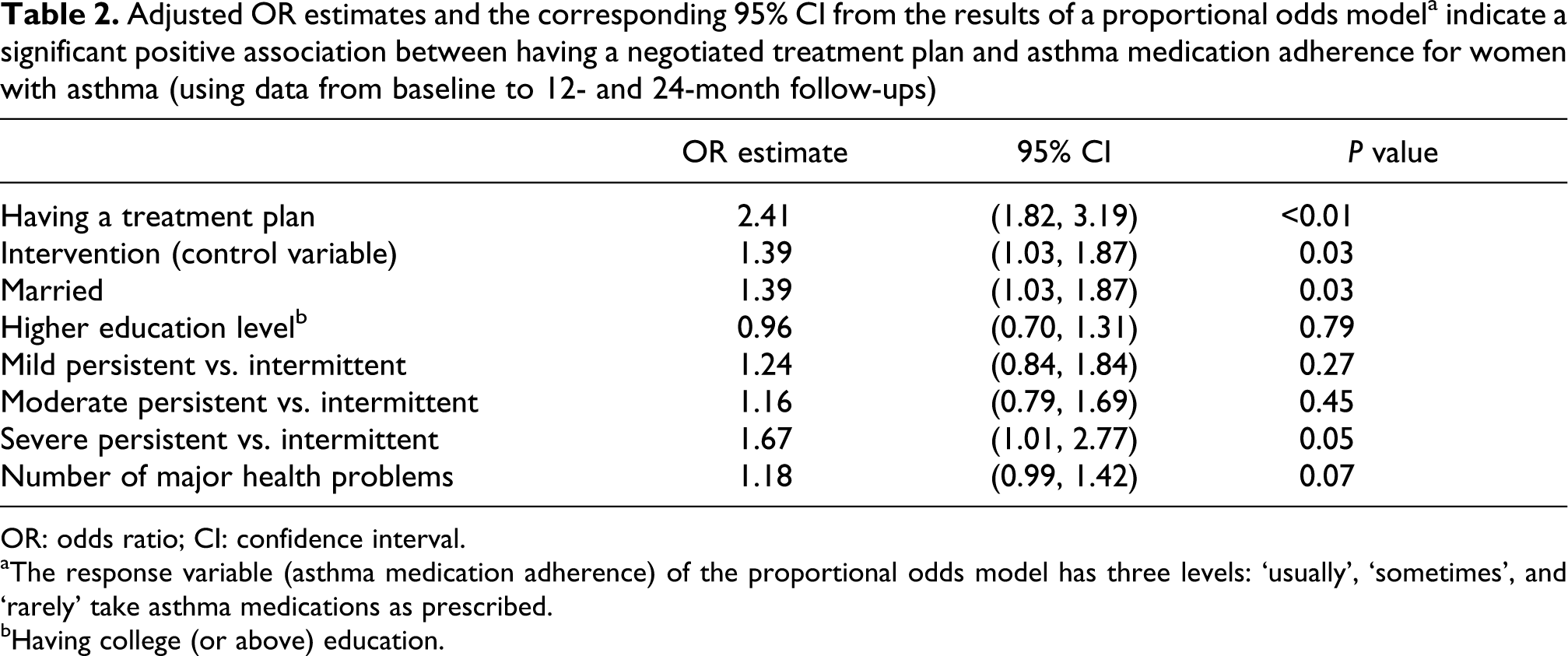
Table 2 illustrates that by follow-up, women with a negotiated treatment plan were more adherent to the prescribed medicine regimen than women without a negotiated treatment plan. The estimated proportional odds ratio was 2.41 (95% CI = (1.82, 3.19)), suggesting that the odds of ‘usually’ versus ‘sometimes or rarely’ taking prescribed asthma medications for women who had a negotiated treatment plan were 2.41 times the odds for women who did not have a treatment plan. In addition, asthma severity (severe persistent vs. intermittent) and marital status were significantly positively associated with adherence to prescribed medicine regimens (p = 0.05 and 0.03, respectively).
Adjusted OR estimates and the corresponding 95% CI from the results of a proportional odds modela indicate a significant positive association between having a negotiated treatment plan and asthma medication adherence for women with asthma (using data from baseline to 12- and 24-month follow-ups)
OR: odds ratio; CI: confidence interval.
aThe response variable (asthma medication adherence) of the proportional odds model has three levels: ‘usually’, ‘sometimes’, and ‘rarely’ take asthma medications as prescribed.
bHaving college (or above) education.
Oral steroid use
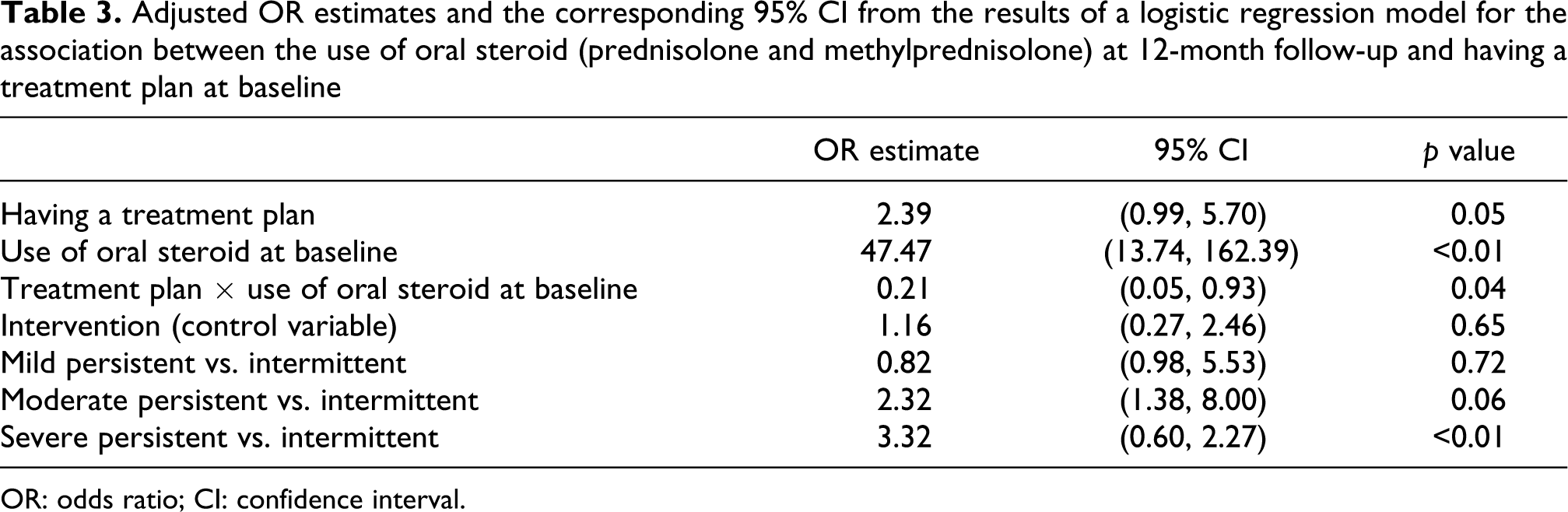
Because oral steroid use is an important marker of asthma exacerbation, we assessed the association between oral steroid use at follow-up and baseline presence of a treatment plan. Among 59 women who had oral steroid prescriptions at baseline, about half (N = 31) stopped taking oral steroid at 12 months: (of the 41 women, 23 (56%) with a treatment plan vs. 8 (44%) of the 18 women without a treatment plan). Among the 539 women who did not have an oral steroid prescription at baseline, the majority (N = 514, 95%) remained oral steroid free at follow-up. Of the 242 women, only 17 (3%) with a treatment plan and of the 297 women, 8 (1.5%) without a treatment plan took oral steroids during the 12-month follow-up period. Table 3 shows a significant interaction between oral steroid use at baseline and treatment plan, thereby indicating that the association between decline in oral steroid use occurred for those with baseline use and a negotiated treatment plan (p = 0.04). The odds of oral steroid use at follow-up were estimated to be reduced by 49% as a result of having a treatment plan at baseline.
Adjusted OR estimates and the corresponding 95% CI from the results of a logistic regression model for the association between the use of oral steroid (prednisolone and methylprednisolone) at 12-month follow-up and having a treatment plan at baseline
OR: odds ratio; CI: confidence interval.
Symptom days and symptom nights
Tables 4 and 5 show that annual symptom days and symptom nights from baseline to follow-up for women who had a negotiated treatment plan at baseline were significantly higher than for women who did not have a negotiated treatment plan at baseline. Women with a negotiated treatment plan at baseline were estimated to have 17% (95% CI = (8%, 27%)) more symptom days (Table 4) and 31% (95% CI = (16%, 48%)) more symptom nights (Table 5) than women without a treatment plan at baseline.
Adjusted estimated factor and the corresponding 95% CI from the results of a Poisson regression model for the association between annual average symptom days at 12-month follow-up and having a negotiated treatment plan at baseline

CI: confidence interval.
aAdjusting for baseline symptom days, study intervention, baseline asthma severity, and number of major health problems, the estimated count of symptom days for women having a treatment plan at 12-month follow-up increases by a factor of 1.17 (p < 0.01).
Adjusted estimated factor and the corresponding 95% CI from the results of a Poisson regression model for the association between annual average symptom nights at 12-month follow-up and having a negotiated treatment plan at baselinea

CI: confidence interval.
aAdjusting for baseline symptom nights, study intervention, baseline asthma severity, and number of major health problems, the estimated count of symptom nights for women having a treatment plan at 12-month follow-up increases by a factor of 1.31 (p < 0.01).
Health care use
Table 6 illustrates no significant difference in overnight hospitalizations at the one year follow-up point associated with having a negotiated treatment plan at baseline. Table 7 shows no association with the number of times the women in this study visited the emergency department, and Table 8 shows number of unscheduled, urgent physician visits.
Adjusted estimated factor and the corresponding 95% CI from the results of a Poisson regression model for the association between overnight hospitalizations at 12-month follow-up and having a treatment plan at baseline

CI: confidence interval.
aAdjusting for baseline hospitalizations, study intervention, baseline asthma severity, and number of major health problems, the estimated count of hospitalizations for women having a treatment plan at 12-month follow-up increases by a factor of 1.55 (p = 0.14).
Adjusted estimated factor and the corresponding 95% CI from the results of a Poisson regression model for the association between number of ED visits at 12-month follow-up and having a treatment plan at baseline

ED: emergency department; CI: confidence interval.
aAdjusting for baseline ED visits, study intervention, baseline asthma severity, and number of major health problems, the estimated count of ED visits for women having a treatment plan at 12-month follow-up increases by a factor of 1.46 (p = 0.15).
Adjusted estimated factor and the corresponding 95% CI from the results of a Poisson regression model for the association between urgent physician visits at 12-month follow-up and having a treatment plan at baseline

CI: confidence interval.
aAdjusting for baseline urgent physician visits, study intervention, baseline asthma severity, and number of major health problems, the estimated count of urgent physician visits for women having a treatment plan at 12-month follow-up increases by a factor of 1.13 (p = 0.82).
Discussion
A clear finding from this study is that women with a negotiated treatment plant report greater adherence to their asthma medicine regimen, and the subgroup using oral steroids at baseline had lower use at follow-up. Adherence is a difficult behavior to assess either through subjective self-report or more potentially objective means such as counters embedded in metered dose inhalers. 14 Whether adherence reports were completely accurate or not is less concerned in this study than differences in outcomes observed between those women with and without a negotiated treatment plan. Women who had negotiated plans were not different from those without regarding asthma severity, comorbidities, and other factors except education level and number of asthma medications used. It may be that such plans are considered by clinicians more important for patients handling several prescriptions. The plan may have aided adherence to multiple medicines, for example, made clearer a more complex regimen. Nonetheless, over a 1-year follow-up period having a negotiated plan was not associated with less health care use for asthma. It may be that such outcomes take time to evolve and would emerge over a longer time period of use of a negotiated plan. For example, we have previously discussed that accurate determination of health care use requires at least 18 months of data. 15,16 The numbers in our sample at follow-up time points did not allow us to test this speculation. In the 1-year shorter term, however, no reductions in symptom and health care use outcomes were observed. Furthermore, in fact, women with a negotiated plan had more symptoms at follow-up than women without. It may be that although symptom reports did not differ at baseline between the groups, women given treatment plans had more clinical features of asthma. This idea is supported by the fact that they were prescribed more asthma medications by their clinicians.
It may be that the greater adherence observed in this study reflects an enhanced relationship between patient and clinician. The physician’s effort to engage the patient in determinations about the treatment plan may increase the patient’s understanding of clinical expectations and confidence in the recommendations. Adherence has been shown to comprise a range of psychosocial and communication factors between physician and patient. 15,16 Improved interactions may result over time in better asthma health status outcomes, again, a speculation we could not test.
There are limits to this study. It involved only women. Outcome patterns for men may differ. However, women comprise a subpopulation of patients who are most vulnerable to negative asthma outcomes. Women enrolled in the research do not necessarily represent all women with asthma, although they are likely similar to women seeking care in similar health care facilities. Because we had no way to directly determine the representativeness of the sample, caution should be taken in extrapolating results to all women with asthma or other high risk subgroups of patients. Adherence data were self-reported and this mode of data collection comprises a limitation faced in virtually all asthma studies. We were not able to verify the accuracy of the reports of adherence. However, as noted, our main interest in the present study was detecting difference in adherence recognizing that self-reports may over-estimate actual behavior in both the groups, with and without a negotiated plan. 17 Similarly, presence of a negotiated treatment plan was self-reported. We were not able to verify that women had a negotiated plan through discussions with physicians, or reviewing the plan in person with the patient or checking medical records. We took at face value the statement of the study participant. It is possible that women reporting having a negotiated plan were ones who remembered the event of acquiring it and were more likely to use the plan. Our procedure did not guard against women being in the comparison group who acquired a plan but did not remember the event and/or were not interested in using the plan. The comparison group, therefore, could potentially comprise some patients not disposed to using any plan. Further, women in this study were asked whether they had worked with their physician to develop a treatment plan, but they did not provide information regarding whether they wanted to negotiate the elements of a plan with their clinician or whether the results of such a plan were satisfactory to them. Both may be the factors influencing subsequent asthma management behavior and outcomes. However, discussions of the utility of the negotiated treatment plan have emphasized that the opportunity for participation in decision making is a critical feature of future behavior and this study tapped this assumption.
Conclusion
Clinician and patient negotiating a treatment plan appear to achieve an important clinical goal: more adherence to physician’s recommendations. The subgroup of women using oral steroids may need less of this medicine, if they have such a plan. The effect of more engaged participation in evolving the plan on asthma outcomes such as symptoms and health care use was not evident in this study and deserves further investigation. Realizing these changes may require additional counseling and support. Involvement in a negotiated treatment plan may favor patients at higher education levels, and the ways to engage those with lower educational attainment appear to be necessary.
Footnotes
Funding
This study was supported by grants 1R18HL060884 and R18HL094272 from the Lung Division of the National Heart, Lung, and Blood Institute of the National Institutes of Health.