
Abstract
This article explores the structural and physiological changes that occur in the ageing lung, and the impact that lung disease and other co-morbidities may have on it. The major changes associated with ageing are reduced lung elasticity, respiratory muscle strength and chest wall compliance, all of which may be influenced by impaired lung growth in early childhood and adolescence. The resultant reduction in diffusing capacity may not be relevant in a fit older adult, but co-morbidities may interact to cause breathlessness and impairments in quality of life. Lung function declines with age, but forced vital capacity (FVC) begins to decline later than forced expiratory volume in 1 s (FEV1) and at a slower rate. This results in a natural fall in the FEV1/forced vital capacity (FVC) ratio which may result in overdiagnosis of chronic obstructive pulmonary disease, and hence the need to ensure the FEV1 is less than 80% before confirming the diagnosis. As older adults probably have a diminished response to hypoxia and hypercapnia, they become more vulnerable to ventilatory failure during high-demand states such as heart failure and pneumonia and therefore to possible poorer outcomes. Poor nutritional status is likely to be an important factor, as is cognitive impairment. It is important to assess older patients using a range of clinical and physiological parameters rather than on the basis of age per se which is a poor predictor of outcome.
Introduction
Respiratory disease is the second commonest cause of severe disability in older adults, second only to musculoskeletal disorders (and four times more common than stroke). Atypical presentations are more common in old age, and older patients may report less breathlessness 1 than younger adults despite similar physician-assessed severity. 2
There is still compelling evidence that older people are not treated purely on the basis of their physiological condition and their wishes but on age per se. The medical profession is unduly pessimistic about the outcomes in older people. It is never more true that patients in this age group are either overtreated when palliative care would have been preferable to the patient, or undertreated because of the physician’s expectation of a poor outcome.
There is a very good evidence regarding the futility of basing treatment decisions on the ground of age alone. In the 2007 COPD and Asthma Outcome Study (CAOS) of prognosis for patients with chronic obstructive pulmonary disease (COPD) in intensive care units, age was only a very small independent factor. 3 There was a marked deviation between physician-predicted survival and actual survival. In fact, the tenth of patients with the poorest clinician prognosis had a predicted 180-day survival of around 3% and an actual survival of around 36%. Eleven characteristics were found to have a significant independent association with increased hospital mortality in addition to age, such as the presence of severe respiratory disease, low pH, low serum albumin and multiorgan failure.
Premorbid physical and cognitive function should also be added to that list, something that is not well assessed and probably a better surrogate than age itself. The only thing that does increase with age is variability—from the marathon runner to the bed bound! Homeostatic instability is a hallmark of ageing—there is no homogeneous biomass called ‘the elderly.’ And so we have to distinguish between the fit and the frail.
Changes within the lung with age
Table 1 sums up the major physiological changes that are thought to occur with age. The major factor in the declining lung function with age is loss of lung elasticity, aggravated by increasing stiffness of the chest wall and reduced respiratory muscle strength. This results in airspace dilatation, increased collapsibility of small airways and a reduction in expiratory volumes. All these are consistent with emphysema or small airways disease and led to the coining of the somewhat poor term ‘senile emphysema.’ This increased tendency to collapse may be the cause of the poor reliability of bibasal crackles as a physical sign in old age. Total lung capacity remains unchanged, an important differentiation between ‘senile emphysema’ and actual emphysema. This is because as lung elastic recoil reduces, the reduction in vital capacity is associated with an increase in residual volume and chest wall stiffness.
Major changes in lung physiology with age

aNot conclusively proven. Adapted from reference 4 with permission.
And we also see a reduction in diffusing capacity with age, the transfer factor reducing to approximately one-half to two-thirds of the values predicted for young adults. This fall has been attributed to several factors including a reduced efficiency in ventilation, producing lower effective alveolar volume and reduced blood volume in pulmonary capillaries.
Gas exchange is good at rest, oxygen requirements are less as the basal metabolic rate is lower. However, there is an increased ventilation–perfusion mismatch during exercise, due to the closure of small airways and reduced alveolar surface area (which reduces by around 20%). This alveolar dead space affects arterial oxygen without impairing carbon dioxide elimination. Both inspiratory and expiratory respiratory muscle strength decreases with age, but its clinical implications have been poorly studied. It may impair effective cough, which is important for airway clearance.
Of course, these changes may be irrelevant in the otherwise healthy older adult but may explain the increased impact of lung disease with age. Undernutrition, common in older people and those with neurological and respiratory disease, is also likely to be a significant factor.
The loss of lung elasticity may be due to stretch or alteration in cross-linkage of elastin and/or collagen. The top right photograph in Figure 1 is a normal terminal bronchiole of a 42-year-old man. The lower right photo is an old but normal terminal bronchiole with a hugely dilated respiratory bronchiole/alveolar duct coming off it, illustrating the dilatation of the old bronchiole. On the left, we see normal visceral pleura with normal underlying lung parenchyma in the same young specimen and beneath the older lung demonstrating marked age-related dilatation of the alveoli.

Section of normal lung in a young and old subject. Pictures from reference 4 with permission.
Of course, the lung function will be heavily influenced by impairment of lung growth as Figure 2 illustrates. The lung matures by the age of 20–25 years, and thereafter ageing is associated with progressive decline in lung function. Many factors have been observed to influence lung growth and decline as outlined here. A recent article by Svanes et al. 5 has noted that maternal asthma, childhood asthma, maternal smoking and childhood respiratory infections are associated with lower forced expiratory volume in 1 s (FEV1).
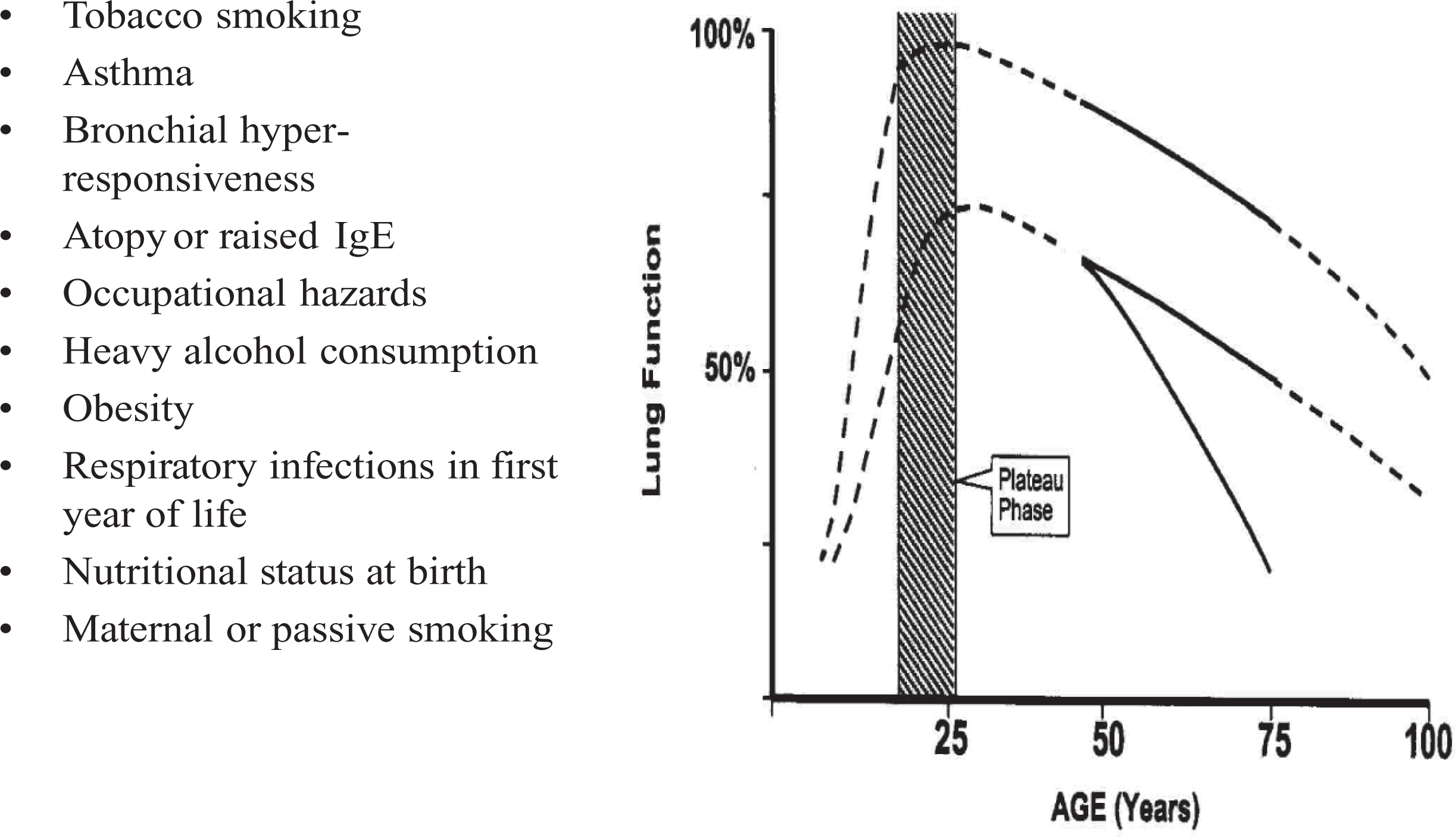
Factors related to age-associated decline in forced expiratory volume in 1 s (FEV1). Taken from reference 4 with permission.
Most lung function data are derived from cross-sectional studies, and good data are available up to the age of 85. The decline in lung function with age may be nonlinear, with some reports suggesting an acceleration in the rate of decline in FEV1 with increasing age. COPD in older adults as in all ages is underdiagnosed but the FEV1/forced vital capacity (FVC) criteria will also overdiagnose it. This is because FVC begins to decline later than FEV1 and at a slower rate. This results in a natural fall in the FEV1/VC ratio from about 75% to about 70% by the age of 70 years. This means that the threshold for the definition of airflow obstruction is likely to be met in many older people and hence is less discriminative. This has led to arguments concerning the use of lower limit of normal (LLN) or other measures. The UK National Institute of Health and Clinical Excellence states that currently there are no enough longitudinal studies using LLN to use it routinely.
Interaction of ageing and lung disease
Age itself, the passage of time, may interact with lung disease. There are higher levels of frailty, worse cognitive function and musculoskeletal changes such as kyphosis which may impair respiratory function and our ability to treat the symptoms. Such interactions are highlighted in Figure 3.

Interaction of age with lung disease.
It is important to differentiate a fit older adult from someone with multiple pathologies and frailty. Frailer patients may have a vague presentation and co-morbidities, fewer physical or laboratory signs and sometimes precarious social circumstances.
In common with changes in other bodily control mechanisms, a variety of age-related changes result in relative inefficiency in the monitoring and control of ventilation—older adults have decreased sensation of dyspnoea and may have a diminished ventilatory response to hypoxia and hypercapnia, making them more vulnerable to ventilatory failure during high-demand states such as heart failure and pneumonia and therefore to possible poorer outcomes.
Cognitive function is a vital area in the assessment of the older person. The UK national dementia strategy sets out several steps to improve the care for such people. As up to 70% of acute hospital beds are currently occupied by older people and up to a half of these may be people with cognitive impairment, consideration of this area is vital for physicians. Eighty-five percentage of elderly people can perform spirometry, 6 but this depends on cognitive function. Figure 4 shows the ability of 208 institutionalised elderly patients to perform spirometry versus a technically simpler respiratory impedence measurement in relation to their cognitive function. 7

Cognitive function and percentage completion of spirometry and forced oscillation using the Mini-Mental State Examination Score (MMSE) in institutionalised patients.
Conclusions
The ageing population presents us with many challenges and it is useful to understand the changes that occur with age in the lung. We should also be aware of the broader view in such patients and take into account issues of frailty, dementia and physical functioning.
Unfortunately some of the research conducted in this area is now approaching old age itself, and it is high time that we looked again at some of this data and get a better understanding of the consequences of ageing on the lung in health and disease. As much as we would like to, we cannot turn back the clock but we can perhaps try to make the latter years a better experience for our elders.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.