
Abstract
Objective:
Age-related hearing loss (ARHL) and age-related cognitive decline (ARCD) are leading causes of disability in older adults. ARHL may increase ARCD risk and cause depression development. This study aimed to explore the associations of ARHL with ARCD and depression in Chinese centenarians and oldest-old adults.
Methods:
A household survey was conducted on 859 centenarians and oldest-old adults residing in 16 cities and counties in China. Basic information was collected using interview questionnaires, physical examinations, and blood tests conducted by systematically trained local doctors and nurses.
Results:
In total, 501 (58.3%), 649 (75.6%), and 211 (24.6%) participants had ARHL, ARCD, and depression, respectively. The prevalence of ARCD and depression was significantly higher in participants with ARHL than in those without ARHL (all p < 0.05). Participants with ARHL had significantly lower Mini-Mental State Examination (MMSE) scores indicative of more cognitive decline, and significantly higher 15-item version of the Geriatric Depression Scale (GDS-15) scores suggesting greater levels of depression, than those without ARHL (all p < 0.05). Multivariate logistic regression analyses (Stepwise) indicated that ARHL was significantly and positively associated with ARCD [odds ratio (OR): 1.594, 95% confidence interval (CI): 1.132, 2.245] and depression (OR: 1.623, 95% CI: 1.139, 2.314; all p < 0.05). Multivariate linear regression analyses (Stepwise) indicated that ARHL was significantly and inversely associated with MMSE scores (B: −2.520, 95% CI: −3.356, −1.684) and significantly and positively associated with GDS-15 scores (B: 0.713, 95% CI: 0.328, 1.098; all p < 0.05).
Conclusion:
ARHL is independently associated with ARCD and depression in Chinese centenarians and oldest-old adults.
Keywords
Introduction
Age-related cognitive decline (ARCD) is a leading cause of disability worldwide, affecting approximately 6.5% of the population aged > 65 years. 1 ARCD develops from aging-related decline in cognitive function and characterized by reduced memory, learning, thinking, and language. 2 The 2016 World Report predicted that the incidence of ARCD will double every 20 years. 3 Age-related hearing loss (ARHL) refers to a gradual loss of hearing, typically caused by aging-related irreversible degeneration of structures in the inner ear or auditory nerve. Approximately one-third of adults aged > 65 years have ARHL, with the rate being 75% in adults aged > 80 years.4,5 Recently, the Livingston in the Lancet Commission on Prevention, Intervention, and Care for Persons with Dementia highlighted that managing hearing loss may reduce the risk of developing dementia. 6 A recent cohort study of older men (mean age, 72.5 years) found that those with ARHL have a higher risk of ARCD than do those without significant ARHL. 7 Moreover, a previous cohort study found that ARHL is associated with an increased prevalence of ARCD. 8
While ARCD and ARHL may be comorbid, communication difficulties can also aggravate behavioral problems, including depression. 9 ARHL is associated with a wide range of health issues, such as increasing social isolation, self-esteem loss, depressive symptoms, disease burden, and hospitalization risk. There is increased awareness of this condition as a critical public health concern.10–13 ARHL may be an effective and modifiable biomarker for ARCD, thus supporting further consideration of ARHL as a risk factor for this condition. 14 The population-based GreatAGE Study showed that ARHL is associated with depression in later life among Italian community-dwelling older adults.15,16 However, most studies on the associations between ARHL, ARCD, and depression are from Western countries.
As a representative population of healthy longevity and successful aging, centenarians are generally believed to have a low prevalence rate and specific protective mechanisms against age-related diseases.17,18 Centenarians have been suggested to have a delayed or escaped onset and interaction with age-related illnesses, such as ARCD and ARHL. Some centenarians may experience a delayed onset of age-related illnesses (delayers), whereas others may not succumb to any age-related illnesses (escapers). 19 The prevalence and associations among ARHL, ARCD, and depression may have their own characteristics and need further research in Chinese centenarians and oldest-old adults. The Hainan Province is an area with high longevity and also has the highest population density of centenarians in China. The China Hainan Centenarian Cohort Study provides a considerable population-based sample of centenarian adults. 20 This study aimed to explore the associations of ARHL with ARCD and depression in Chinese centenarians and oldest-old adults.
Methods
Study participants
This cross-sectional study conducted a household survey on all the centenarians and oldest-old adults aged 80–99 years residing in 16 cities and counties in Hainan Province, China, from June 2014 to June 2016, according to the list of centenarians and oldest-old adults provided by the Department of Civil Affairs of Hainan Province. 21 A survey sample of 1863 participants included 966 centenarians aged > 100 years and 897 oldest-old adults aged 80–99 years. After excluding participants with missing variables (596 centenarians and 408 oldest-old adults), 859 participants (370 centenarians and 489 oldest-old adults) were finally included in the study (Figure 1(a)). All the 859 participants had no missing data for each variable. This study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Ethics Committee of Hainan Hospital of the Chinese People’s Liberation Army General Hospital (301hn11-206-01). All participants provided written informed consent prior to participating in the study.
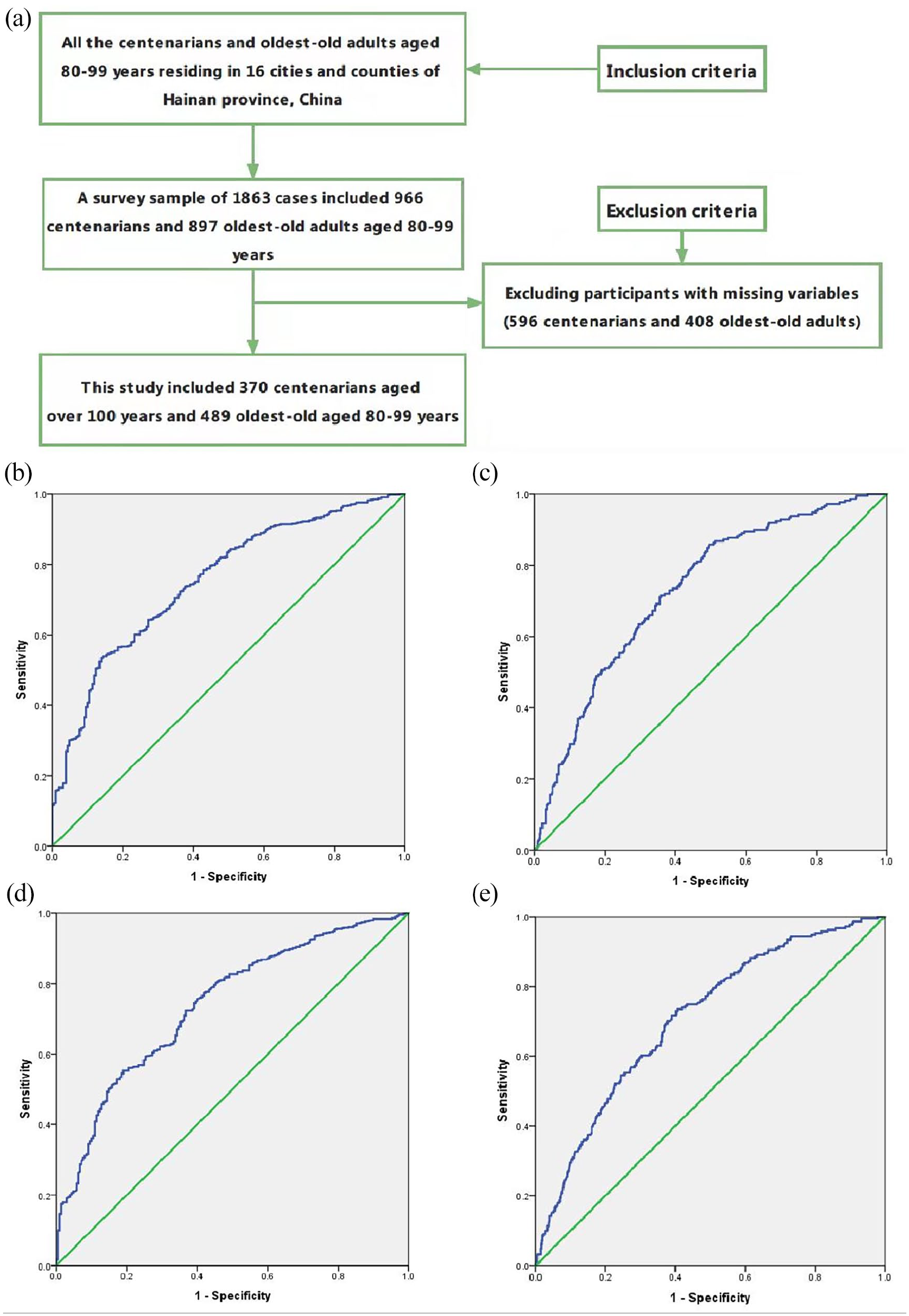
(a) Participant inclusion flowchart. (b) Receiver operating characteristic (ROC) curve of the multivariate regression model (Enter) for identifying ARCD. (c) ROC curve of the multivariate regression model (Enter) for identifying depression. (d) ROC curve of the multivariate regression model (Stepwise) for identifying ARCD. (e) ROC curve of the multivariate regression model (Stepwise) for identifying depression.
Survey protocol
The household survey method was used to collect basic information through interview questionnaires, physical examinations, and blood tests. The survey was conducted according to standard procedures by systematically trained local doctors and nurses of Hainan Hospital of the Chinese People’s Liberation Army General Hospital, who could communicate in the local language. The research team included otolaryngologists, internists, geriatricians, cardiologists, endocrinologists, nephrologists, and nurses. 22
Study variables
The presence of ARHL was determined through physical examination and hearing questionnaire administered by trained staff from the Medical Hearing Research Institute of the Chinese People’s Liberation Army General Hospital. The staff were familiar with hearing screening procedures, determined no obstructed external auditory meatus, and identified an intact tympanic membrane with landmarks. All evaluations were conducted in a quiet room with a controlled background noise.
The primary assessment tool was the Mini-Mental State Examination (MMSE), which is a well-known method for evaluating cognitive function. The Georgia Centenarian Study also confirmed that age and education can significantly affect MMSE performance. 23 The cutoff points for identifying ARCD varied according to the level of education: illiteracy, 17 points; elementary school level, 20 points; and junior high school level, 24 points. 24 Depressive symptoms were screened using the 15-item version of the GDS-15, with the cutoff for clinically critical depressive symptoms set at ⩾6 points. The GDS-15 has been validated as a screening tool for depressive symptoms among older adults.25,26 A cutoff point of ⩾6 has a pooled sensitivity of 79% and specificity of 77% for diagnosing depression in older adults. 27
The study variables included age, sex, body mass index, living alone, mental work, smoking, drinking, education degree (i.e. illiteracy, elementary school level, and junior high school level), hypertension, diabetes, cardiovascular diseases, red blood cells, hemoglobin, iron, sodium, potassium, calcium, phosphorus, and magnesium. Age as a continuous variable and sex as a categorical variable were determined from national identification cards. Based on recommendations from the World Health Organization, weight was measured twice on a digital scale with the participants in light clothing without shoes. Height was also measured twice using a wall-mounted tape with participants standing without shoes. 28 Body mass index, as a continuous variable, was calculated as the weight in kilograms divided by the square of the height in meters. Living alone and mental work (yes or no) as categorical variables were determined by asking the participants, their relatives, and neighbors and verified using related population records and medical information.
Hypertension as a categorical variable was defined as systolic blood pressure ⩾140 mm Hg, diastolic blood pressure ⩾90 mm Hg, or the use of antihypertensive drugs. 29 Diabetes as a categorical variable was defined as fasting blood glucose ⩾7.0 mmol/L or the use of antidiabetic drug/insulin. 30 Cardiovascular diseases as a categorical variable was defined based on medical history, symptoms, cardiac markers, and tests (e.g. electrocardiogram, echocardiogram, computed tomography, and coronary arteriography) according to the American College of Cardiology/American Heart Association/European Society of Cardiology guidelines.31–33 Venous blood samples were drawn and transported in chilled biotransport containers (4°C) to our central laboratory within 4 h. Serum levels of red blood cells, hemoglobin, iron, sodium, potassium, calcium, phosphorus, and magnesium as continuous variables were tested by qualified technicians blinded to the clinical data.
Statistical analysis
Normally distributed continuous data were described as the mean ± standard deviation and compared using the independent sample t test. Non-normally distributed continuous data were described as the median (interquartile range) and compared using the Mann–Whitney U test. Meanwhile, categorical data were described as number (percentage) and compared using chi-square test. To determine definite relationships in different methods, multivariate logistic regression analyses were used to assess the associations of ARHL and other variables with ARCD and depression (categorical variables). Meanwhile, multivariate linear regression analyses were used to assess the associations of ARHL and other variables with MMSE and GDS-15 (continuous variables). Odds ratios (ORs) > 1.00 indicated increased odds of ARCD and depression with every unit increase in ARHL and other variables, whereas ORs < 1.00 indicated lower odds of ARCD and depression. Statistical analyses were performed using Statistical Package for Social Sciences version 19.0 software package. All tests were two-sided, and p < 0.05 was considered significant.
Results
In total, 501 (58.3%), 649 (75.6%), and 211 (24.6%) participants had ARHL, ARCD, and depression, respectively. As shown in Table 1, participants with ARHL were significantly older; had lower BMI; lower proportion of mental work; lower levels of red blood cells, hemoglobin, iron, sodium, and calcium; and higher levels of potassium and magnesium than those without ARHL (all p < 0.05). The prevalence of ARCD and depression was significantly higher in participants with ARHL than in those without ARHL (all p < 0.05). Participants with ARHL had significantly lower MMSE scores indicative of more cognitive decline, and significantly higher GDS-15 scores suggesting greater levels of depression, than those without ARHL (all p < 0.05).
Characteristics of all the centenarians and oldest-old adults.
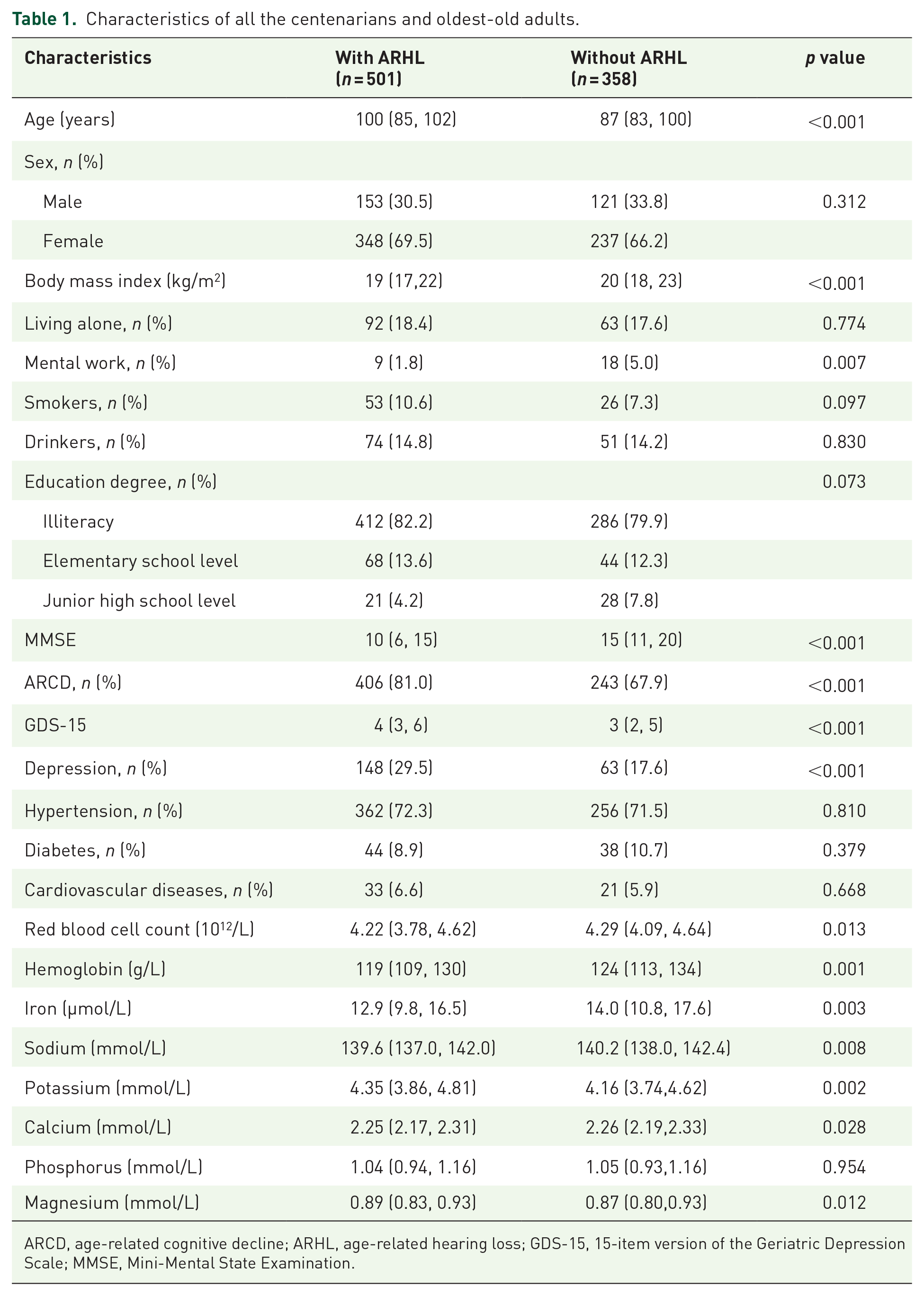
ARCD, age-related cognitive decline; ARHL, age-related hearing loss; GDS-15, 15-item version of the Geriatric Depression Scale; MMSE, Mini-Mental State Examination.
As shown in Tables 2 and 3, multivariate logistic regression analyses (Enter) indicated that ARHL was significantly and positively associated with ARCD [OR: 1.637, 95% confidence interval (CI): 1.147, 2.336] and depression (OR: 1.575, 95% CI: 1.096, 2.265; all p < 0.05). As shown in the receiver operating characteristic (ROC) curves, the areas under the curve (AUCs) for these regression models were 0.755 (0.718–0.791; p < 0.001, Figure 1(b)) for identifying ARCD and 0.730 (0.692–0.767; p < 0.001, Figure 1(c)) for identifying depression. In addition, multivariate linear regression analyses (Enter) indicated that ARHL was significantly and inversely associated with MMSE scores (B: −2.610, 95% CI: −3.453, −1.767) and significantly and positively associated with GDS-15 scores (B: 0.642, 95% CI: 0.252, 1.033; all p < 0.05).
Multivariate analyses (Enter) of association of ARHL with ARCD or MMSE in centenarians and oldest-old adults.
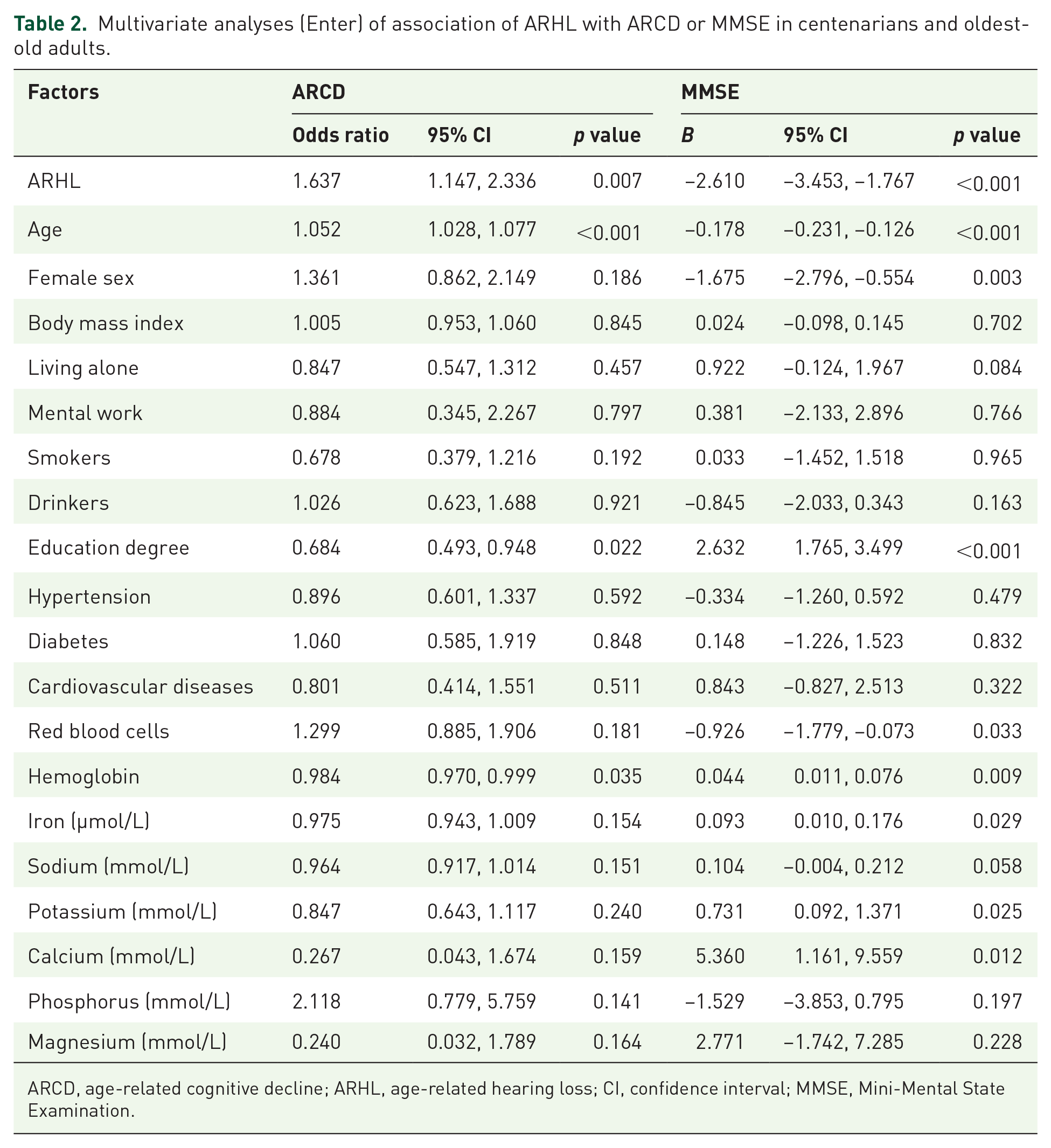
ARCD, age-related cognitive decline; ARHL, age-related hearing loss; CI, confidence interval; MMSE, Mini-Mental State Examination.
Multivariate analyses (Enter) of association of ARHL with depression or GDS-15 in centenarians and oldest-old adults.

ARHL, age-related hearing loss; CI, confidence interval; GDS-15, 15-item version of the Geriatric Depression Scale.
As shown in Tables 4 and 5, multivariate logistic regression analyses (Stepwise) indicated that ARHL was significantly and positively associated with ARCD (OR: 1.594, 95% CI: 1.132, 2.245) and depression (OR: 1.623, 95% CI: 1.139, 2.314; all p < 0.05). As shown in the ROC curves, the AUCs for these regression models were 0.739 (0.702–0.777; p < 0.001, Figure 1(d)) for identifying ARCD and 0.707 (0.668–0.746; p < 0.001, Figure 1(e)) for identifying depression. In addition, multivariate linear regression analyses (Stepwise) indicated that ARHL was significantly and inversely associated with MMSE scores (B: −2.520, 95% CI: −3.356, −1.684) and significantly and positively associated with GDS-15 scores (B: 0.713, 95% CI: 0.328, 1.098; all p < 0.05). In all multivariate analyses (Enter and Stepwise) of different electrolytes, blood calcium levels were negatively associated with depression and GDS-15 scores (all p < 0.05). Meanwhile, blood calcium and iron levels were positively associated with MMSE scores (all p < 0.05).
Multivariate analyses (Stepwise) of association of ARHL with ARCD or MMSE in centenarians and oldest-old adults.

ARCD, age-related cognitive decline; ARHL, age-related hearing loss; CI, confidence interval; MMSE, Mini-Mental State Examination.
Multivariate analyses (Stepwise) of association of ARHL with depression or GDS-15 in centenarians and oldest-old adults.

ARHL, age-related hearing loss; CI, confidence interval; GDS-15, 15-item version of the Geriatric Depression Scale.
Discussion
ARHL is one of the most common chronic conditions occurring in later life. A recent study reported that approximately 25% of the population aged 65–75 years and 70–80% of those aged ⩾75 years have hearing loss. 34 Current lifespan has improved owing to advances in medical and living conditions, with an increasing number of people living beyond 80 years of age. In this study of 859 centenarians and oldest-old adults aged > 80 years, ARHL occurred in 58.3% (501 participants) of these long-lived older adults. This study had a higher age but lower prevalence of ARHL than the studies by Chien and Lin 35 and Li-Korotky 36 wherein 40–66% of older adults were aged > 75 years and 70–90% were aged > 85 years. This difference in the results may be due to the generally lower prevalence rate and specific protective mechanisms against age-related diseases in centenarians as a representative population of healthy longevity and successful aging.17,18 Centenarians have been suggested to have a delayed or escaped onset and interaction with age-related illnesses, such as ARCD and ARHL. Some centenarians may experience a delayed onset of age-related illnesses (delayers), whereas others may not succumb to any age-related illnesses (escapers). 19 Meanwhile, a previous study demonstrated that the prevalence of depression among older adults in Asia ranges from 7.8% to 34.8%.37,38 This study showed that 211 participants (24.6%) had depression among 859 centenarians and oldest-old adults aged ⩾80 years.
As the leading causes of disability in older adults, ARHL and ARCD are associated with global social and economic burdens.39,40 The risk of ARCD significantly increases as the degree of hearing loss increases in older adults. 41 Hearing difficulties may increase the risk of ARCD and cause social isolation and depression. A cohort study of older men suggested that men with hearing loss are more likely to develop dementia than those without hearing loss. 7 Lin et al. reported that ARHL is independently associated with ARCD in community-dwelling older adults aged 70–90 years. 42 However, although ARHL is associated with ARCD, the exact mechanisms for this association remain unclear. Possible underlying mechanisms include widespread neural degeneration, sensory degradation/deprivation, cognitive resource depletion, and social isolation/depression. 43 A recent study supported that hearing loss may account for up to 9.1% of cognitive decline worldwide, and efforts to reduce this adverse effect should continue to be further explored. 7 Meanwhile, approximately 11.4–19.1% of adults with hearing loss have depression in the United States. A meta-analysis reported that hearing loss is a common disease associated with depression in adults aged ⩾65 years. 9 A Norwegian population-based study found that hearing loss is significantly associated with increased depression. 44
Hearing aids are the most commonly used equipment to treat ARHL. Technological advances in hearing aids may enable effective rehabilitation, even in older adults with profound hearing loss. However, most patients with ARHL are not adequately treated with hearing aids. The use of hearing aids in older adults is hypothesized to improve hearing function, cognition, and depression among these individuals. 45 Castiglione et al. 46 demonstrated that hearing aids are effective for improving depressive and cognitive performance in older adults. The Personnes Agées QUID study of 3670 older adults aged 65 years found that ARHL was associated with accelerated cognitive decline in older adults, and hearing aids attenuated cognitive decline within a 25-year follow-up. 47 A recent review of five studies showed that although the exact result has not been established, there is a potential relationship between hearing aids and cognitive function. 48 Interactions between cognition and immediate or short-term usage of hearing aids have been observed, but limited evidence is available regarding the effect of long-term use of hearing aids on cognitive function. Thus, further research, including in older adults, with longer follow-up periods of hearing aid usage is needed. 49
This study has some limitations. First, this was a cross-sectional study, and the underlying mechanisms remain elusive. Second, the sample size of this study was limited, and there were no long-term follow-up results. Third, this study lacked a calculation (formula used or power analysis) and justification of the sample size. According to the list of centenarians and oldest-old adults provided by the Department of Civil Affairs of Hainan Province, this cross-sectional study conducted a household survey on all the centenarians and oldest-old adults aged 80–99 years residing in 16 cities and counties in Hainan Province, China.
Conclusion
ARHL is independently associated with ARCD and depression in Chinese centenarians and oldest-old adults.
Supplemental Material
sj-doc-2-taj-10.1177_20406223221084833 – Supplemental material for Associations between age-related hearing loss, cognitive decline, and depression in Chinese centenarians and oldest-old adults
Supplemental material, sj-doc-2-taj-10.1177_20406223221084833 for Associations between age-related hearing loss, cognitive decline, and depression in Chinese centenarians and oldest-old adults by Long Feng, Di Wu, Jieqiong Lin, Yulong Li, Yali Zhao, Pei Zhang, Yao Yao and Shihui Fu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-png-1-taj-10.1177_20406223221084833 – Supplemental material for Associations between age-related hearing loss, cognitive decline, and depression in Chinese centenarians and oldest-old adults
Supplemental material, sj-png-1-taj-10.1177_20406223221084833 for Associations between age-related hearing loss, cognitive decline, and depression in Chinese centenarians and oldest-old adults by Long Feng, Di Wu, Jieqiong Lin, Yulong Li, Yali Zhao, Pei Zhang, Yao Yao and Shihui Fu in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
We appreciate all those who participated in the present study for their continued cooperation.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the National Natural Science Foundation of China (81900357, 81903392, 81941021, 81901252, 82001476, 81802804, 81801251), the Military Medical Science and Technology Youth Incubation Program (20QNPY110, 19QNP060), the Excellent Youth Incubation Program of Chinese People’s Liberation Army General Hospital (2020-YQPY-007), the Military Medicine Youth Program of Chinese People’s Liberation Army General Hospital (QNF19069, QNF19068), the National Key R&D Program of China (2018YFC2000400), the National S&D Resource Sharing Service Platform Project of China (YCZYPT[2018]07), the Hainan Major Scientific and Technological Cooperation Project (2016KJHZ0039), the China Postdoctoral Science Foundation funded project (2019M650359, 2020M682816, 2021T140298), the Medical Big Data R&D Project of Chinese People’s Liberation Army General Hospital (MBD2018030), the National Geriatric Disease Clinical Medicine Research Center Project (NCRCG-PLAGH-2017-014), the Central Health Care Scientific Research Project (W2017BJ12), the Hainan Medical and Health Research Project (16A200057), the Sanya Medical and Health Science and Technology Innovation Project (2016YW21, 2017YW22, 2018YW11), and the Clinical Scientific Research Supporting Fund of Chinese People’s Liberation Army General Hospital (2017FC-CXYY-3009). The sponsors had no role in the design, conduct, interpretation, review, approval, or control of this study.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.