
Abstract
Background
Early-onset type 2 diabetes (T2DM), diagnosed before age 40, progresses rapidly and has a higher risk of complications compared to late-onset T2DM. Its global prevalence is rising, but the underlying risk factors are insufficiently understood.
Objective
This systematic review and meta-analysis aimed to evaluate risk factors associated with early-onset T2DM to support clinical decision-making and inform preventive strategies.
Methods
37 studies (cohort, case-control, cross-sectional) were identified from PubMed, Web of Science, and Embase up to October 31, 2024. Data were analyzed using STATA 17.0, and pooled odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Subgroup analyses were performed by region, study type, and sample size.
Results
Compared with normoglycemic individuals, early-onset T2DM was strongly associated with family history of diabetes (OR = 4.54, 95%CI: 2.31–8.90), high BMI (OR = 2.87, 95%CI: 2.22–3.80), maternal gestational diabetes (OR = 3.01, 95%CI: 2.44–3.72), and elevated fasting glucose (OR = 8.73, 95%CI: 4.91–16.92). Subgroup and sensitivity analyses confirmed the robustness of these findings despite persistent heterogeneity. In comparisons with late-onset T2DM, family history (OR = 2.90), male sex (OR = 1.57), and BMI (OR = 1.12 per unit) remained significant risk factors.
Conclusion
Early-onset T2DM is shaped by familial, metabolic, and lifestyle determinants. Incorporating these factors into early screening and intervention programs, particularly lifestyle modification in young high-risk populations, is essential to reduce disease burden and delay progression.
Introduction
Diabetes mellitus (DM) has become a global pandemic, affecting approximately 1 in 10 individuals aged 20-79 years and it is one of the leading causes of premature mortality. The global burden of DM continues to rise, with the number of affected individuals projected to reach 784 million by 2045. 1 Early-onset type 2 diabetes (T2DM), defined as a diagnosis before the age of 40, has traditionally been considered a condition of middle-aged and older adults. However, its rising incidence among children, adolescents, and young adults—particularly since the 2000s—has become a major public health concern. This is exemplified by a nearly threefold increase in the standardized incidence ratio among individuals below 40 years old.2–4
Early onset of diabetes prolongs exposure to hyperglycemia, thereby heightening the risk of long-term complications. Furthermore, the progression of type 2 diabetes in younger individuals can be faster and more disruptive compared to those diagnosed later in life, leading to early morbidity and reduced quality of life.5,6 Evidence suggests that early-onset T2DM presents a more severe phenotype, with faster β-cell decline, earlier need for insulin therapy, and a higher lifetime risk of adverse outcomes. 7 It is also marked by greater insulin resistance,8–11and greater deterioration of β-cell function, resulting in a more rapid rise in glycemic levels 12 and elevated risks of complicationsg13–17 and premature mortality.18–20
The rising prevalence of early-onset T2DM has been linked to multiple risk factors, underscoring its multifactorial nature. In the last two decades, a number of studies have explored the risk factors of early-onset type 2 diabetes.21–29 However, small sample sizes, heterogeneous study settings, and uncontrolled confounders have limited the validity and reliability of their findings. A systematic review is therefore needed to address inconsistencies, methodological variations, and potential biases in existing studies, and to provide a more reliable synthesis for clinical practice and future research. Accordingly, this meta-analysis sought to systematically evaluate risk factors for early-onset T2DM and to examine the influence of study region, sample size, and design on the reported associations. The findings are expected to provide robust evidence to inform clinical decision-making and policy development, thereby contributing to strategies that may reduce the burden of early-onset T2DM.
This meta-analysis aimed to systematically evaluate risk factors for early-onset type 2 diabetes (T2DM). It further examined the influence of study region, sample size, and design on reported associations. The novelty of this study lies in its comprehensive synthesis across diverse populations and settings, providing evidence to inform prevention, clinical decision-making, and policy development.
Materials and methods
Given the nature of this meta-analysis, ethical approval was not required, and the study was prospectively registered in PROSPERO (CRD42024560614).
Study selection
Inclusion criteria
The inclusion criteria for the literature were established based on the PECOs principle (P: Participants; E: Exposures; C: Comparisons; O: Outcomes; S: Study design) as follows: ① Participants: Individuals who met the diagnostic criteria for T2DM as defined by the WHO, ADA, or IEC after 1985, and were diagnosed before the age of 40 or 45, as these age thresholds are most commonly adopted in both international and Chinese studies, reflecting the current lack of a universally accepted definition of early-onset T2DM; ② Exposures: Factors influencing the progression of T2DMM, including but not limited to sociodemographic characteristics, lifestyle factors, and anthropometric measures. ③ Comparisons: Comparison with individuals diagnosed with late-onset type 2 diabetes or those without type 2 diabetes; ④ Outcomes: Identification and quantification of risk factors for early-onset type 2 diabetes, as well as the evaluation of the effectiveness of interventions aimed at reducing these risks. Study design: Cohort studies, case-control studies, and cross-sectional observational studies. This study was registered in PROSPERO (CRD42024560614).
Exclusion criteria
The exclusion criteria were as follows: ① Letters to the editor; ② Low-quality literature; ③ Conference abstracts, case reports, and literature with incomplete data; ④ Non-Chinese or non-English literature; ⑤ Studies focused on genetic or chromosomal risk factors.
Literature search strategy
To include studies in this systematic review, we searched multiple databases, including Wan Fang Data, CNKI, China Biomedical Literature Database, VIP, Embase, PubMed, Web of Science, Cochrane Library, and CINAHL, from their inception until October 31th, 2024. Additionally, we reviewed the reference lists of all eligible articles and reviews to identify further studies. The specific search strategy for PubMed was as follows:
Selection process
Two trained researchers independently conducted literature searches based on the established search strategy. The identified articles were imported into EndNote 20, and duplicate records were removed using the “Find duplicates” function. Initial screening was performed by reviewing the titles and abstracts, followed by a comprehensive full-text review. Cross-verification was subsequently conducted, and the corresponding author resolved any disagreements. The literature selection adhered strictly to predefined inclusion and exclusion criteria.
Quality appraisal
The quality assessment of all literature was conducted independently by 2 trained researchers who cross-checked the results at each step. In case of disagreement, a decision was made through discussion or by consulting a third-party expert for Cross-sectional study using the Agency for Healthcare Research and Quality (AHRQ) criterion. 30 This evaluation criterion includes 11 items, with scores of 8 -11 indicating high quality, 4 -7 indicating moderate quality, and 0 -3 indicating low quality. This study included articles scoring ≥6. For cohort and case-control studies, these studies were determined by combining the Newcastle–Ottawa Scale1(NOS) and appraising the number of events per variable. With a score of 9 out of 9, which included study population selection (4 points), comparability of cohort design or analyses (2 points), and outcome evaluation and follow-up (3 points). Scores of 0-3, 4-6, and 7-9 were assigned to low, moderate, and high-quality studies respectively according to this scale.
Data extraction
Data extraction was independently conducted by two researchers using Microsoft Excel software. The extracted data included the first author, publication year, region, study type, sample size, and risk factors. After extraction, a summary was compiled and verified. Any disagreement was resolved by a third researcher, who would make the final decision.
Statistical methods
Data synthesis
All statistical analyses were performed using Stata 17.0. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated as pooled effect sizes. Analyses were conducted separately for early-onset T2DM versus normoglycemic controls and early-onset versus late-onset T2DM. When original studies reported results stratified by prediabetes phenotype, these subgroups were first combined. For risk factors not suitable for quantitative pooling, qualitative summaries were provided.
Heterogeneity
Heterogeneity was assessed using the I2 statistic and Q-test. A fixed-effects model was applied when I2 <50% and P > 0.10; otherwise, a random-effects model was adopted.
Subgroup and sensitivity analyses
In the early-onset versus normoglycemic group, risk factors with substantial heterogeneity (I2 ≥ 50%) and at least five studies were further examined using subgroup analyses and leave-one-out sensitivity analyses to identify potential sources of heterogeneity and to assess the robustness of pooled estimates.
Publication bias
Potential publication bias was evaluated using Egger’s regression test and visual inspection of funnel plots. In this study, Egger’s tests did not indicate significant bias (P > 0.05), and the funnel plots were largely symmetrical, suggesting no evidence of small-study effects.
Result
Literature search results
A total of 1,594 articles were obtained through both database and manual searches of Chinese and English sources. After removing 534 duplicates, 1,001 articles were excluded based on title and abstract review. A further 36 articles were excluded after full-text review, leaving 23 articles for final analysis. Figure 1 presents the flow diagram showing the selection of the identified articles in the literature search. Flow chart of literature screening. The diagram illustrates the process of identifying, screening, and including studies in the meta-analysis according to the PRISMA guidelines. It shows the number of records retrieved, excluded, and finally included at each stage of the selection process.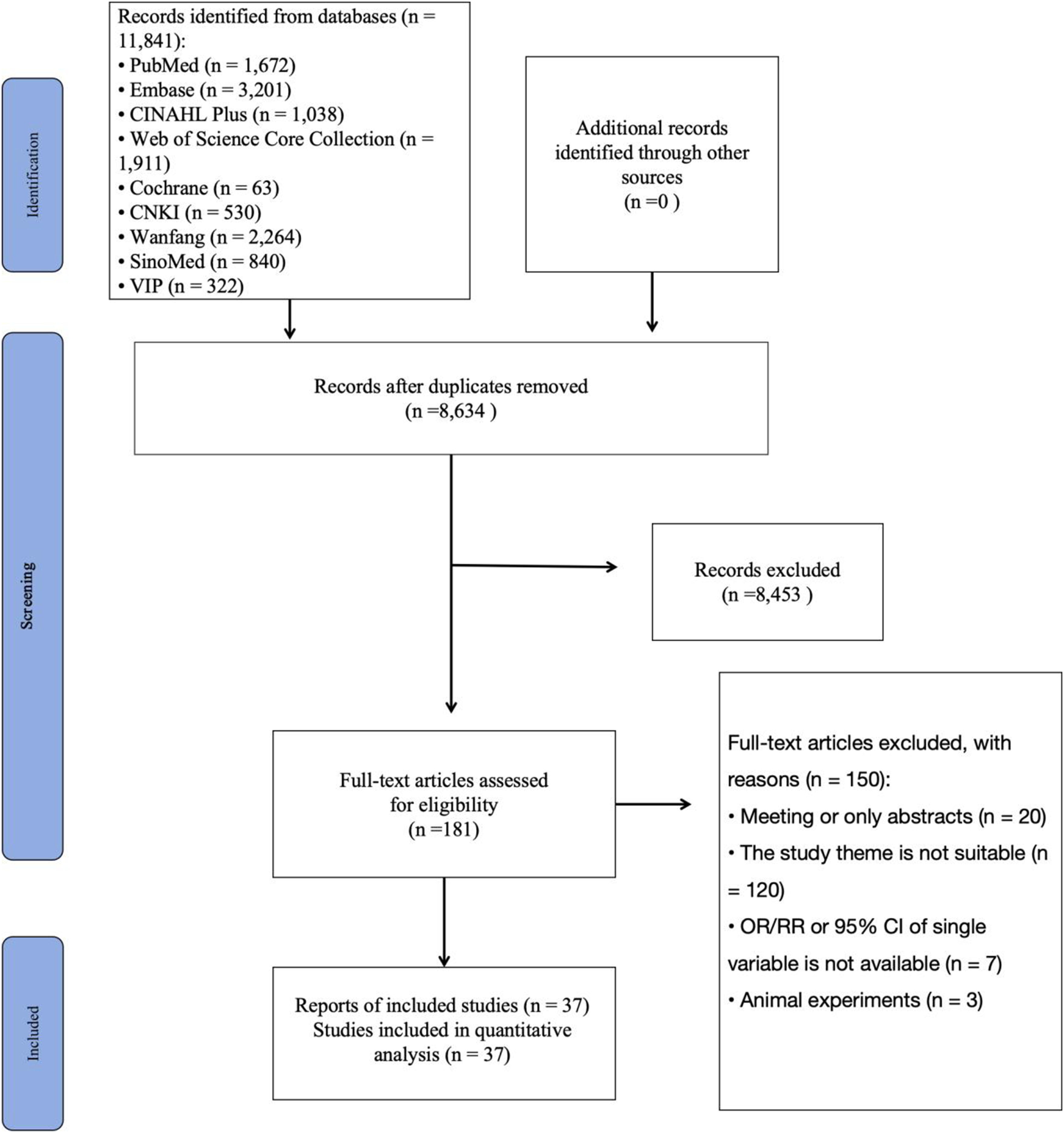
Characteristics of the included studies and methodological quality
Characteristics of included studies.

The characteristics of the 37 included studies are presented in Table 1, comprising 17 studies published in Chinese and 20 in English. Study designs included 24 cross-sectional studies, 9 cohort studies, and 4 case-control studies.
For the cross-sectional studies, methodological quality was assessed using the Agency for Healthcare Research and Quality (AHRQ) checklist. Scores ranged from 2 to 7 out of 11, indicating moderate overall quality. Most studies clearly reported data sources and eligibility criteria, but common shortcomings included insufficient adjustment for confounders, inadequate reporting of missing data, lack of evaluator blinding for subjective outcomes, and limited quality control procedures.
The cohort studies were evaluated using the Newcastle–Ottawa Scale (NOS), with scores ranging from 6 to 9, reflecting generally high quality. Strengths included adequate cohort selection, exposure ascertainment, and follow-up, but many studies provided only limited adjustment for confounders in the Comparability domain.
The case-control studies also used the NOS, with scores ranging from 5 to 8, indicating moderate-to-high quality. While case definitions, control selection, and exposure ascertainment were usually appropriate, several studies did not specify control criteria or failed to adjust for multiple confounders.
Overall, the included studies met most methodological standards; however, insufficient control of confounding, particularly in observational designs, remains a notable concern when interpreting the pooled results. Quality assessment of cross-sectional, cohort, and case-control studies is presented in Supplemental 2, 3, and 4, respectively.
Meta-analysis results of factors influencing the early-onset type 2 diabetes
Meta-analysis of risk factors for Early-onset type 2 diabetes (Early-onset vs normal).

Meta-analysis of risk factors for Early-onset type 2 diabetes (Early-onset vs late-onset).

Early-onset versus normoglycemic controls
Sociodemographic factors: Male sex [OR = 1.62, 95% CI (1.33–1.96)] Family history of diabetes [OR = 2.90, 95% CI (2.29–3.67)] High BMI [OR = 1.44, 95% CI (1.32–1.56)] Maternal gestational diabetes [OR = 3.01, 95% CI (2.44–3.72)] High waist-to-hip ratio [OR = 2.44, 95% CI (2.17–2.74)]
Lifestyle factors: Lack of physical exercise [OR = 2.01, 95% CI (1.25–2.23)] Moderate physical activity [OR = 0.67, 95% CI (0.49–0.92)] → protective factor
Clinical and metabolic indicators: Acanthosis nigricans [OR = 2.49, 95% CI (1.40–4.45)] Elevated triglycerides (TG) [OR = 1.45, 95% CI (1.25–1.68)] Elevated fasting blood glucose [OR = 10.81, 95% CI (6.73–17.39)]
Early-onset versus late-onset T2DM
Sociodemographic and lifestyle factors Family history of diabetes [OR = 1.85, 95% CI (1.32–2.59)] High BMI [OR = 1.52, 95% CI (1.28–1.80)]
Clinical indicators: Elevated triglycerides (TG) [OR = 1.39, 95% CI (1.12–1.72)]
Subgroup analysis
Results of the subgroup analyses on the risk factors for early-onset type 2 diabetes.

Sensitivity analysis
Sensitivity analyses were subsequently performed using a leave-one-out approach. Sequential exclusion of individual studies did not materially alter the pooled estimates, indicating that the results were robust and not driven by any single study.
Publication bias
To evaluate the potential for publication bias, we conducted funnel plot analyses, Egger’s regression tests, and the trim-and-fill method for those risk factors that were examined in 10 or more studies. Triglycerides (TG), body mass index (BMI), and family history met this inclusion threshold, and the corresponding funnel plots are presented in Figures 2–4, respectively. Funnel plot assessing publication bias for triglycerides (TG). The plot shows asymmetry suggesting potential small-study effects. Three studies were imputed using the trim-and-fill method. Funnel plot for body mass index (BMI). The plot appears symmetric with no studies imputed, indicating low risk of publication bias. Funnel plot for family history. The plot shows mild asymmetry. Egger’s test was significant, and two studies were imputed using the trim-and-fill method.


For TG, the funnel plot was asymmetric, and Egger’s test indicated small-study effects (P = 0.001). The trim-and-fill method suggested three missing studies, reducing the pooled OR from 1.45 (95% CI: 1.25–1.68) to 1.39 (95% CI: 1.21–1.61), though the association remained significant.
For BMI, the funnel plot was largely symmetric, and no bias was detected by Egger’s test (p = 0.379). No studies were imputed, and the pooled OR was unchanged at 1.44 (95% CI: 1.32–1.56).
For family history, Egger’s test suggested small-study effects (P = 0.008). Two studies were imputed, with the pooled OR decreasing slightly from 2.90 (95% CI: 2.29–3.67) to 2.76 (95% CI: 2.17–3.52).
Overall, although TG and family history showed signs of publication bias, the adjusted estimates were consistent with the original results, supporting the robustness of the findings.
Discussion
Maternal gestational diabetes increases the risk of early-onset type 2 diabetes in offspring: The importance of improved glycemic control during pregnancy
Our meta-analysis demonstrated a significant association between maternal gestational diabetes (GDM) and the risk of early-onset T2DM in offspring (OR = 3.01, 95% CI: 2.44–3.72). This finding emphasizes the long-term impact of the intrauterine glycemic environment on metabolic health. Evidence from the HAPO follow-up study and other cohorts consistently shows that maternal hyperglycemia increases the likelihood of obesity, impaired glucose tolerance, and metabolic syndrome in children.68–70
Biological mechanisms may involve epigenetic alterations induced by maternal hyperglycemia, which can impair insulin sensitivity, accelerate β-cell dysfunction, and disrupt normal adipose development. These intergenerational effects highlight the importance of achieving optimal glucose control during pregnancy. Early screening for GDM, timely lifestyle counseling, and pharmacological intervention when indicated remain essential to reducing adverse perinatal outcomes and lowering the risk of diabetes in the next generation.
Nonetheless, the current evidence base is limited. Only two eligible studies were available for pooled analysis, restricting the robustness and generalizability of the findings. Differences in diagnostic thresholds, study populations, and confounder adjustment further contribute to uncertainty. Larger, prospective, and ethnically diverse studies are needed to confirm the magnitude of risk and clarify underlying pathways. Despite these limitations, our results, in line with existing literature, support maternal glucose management during pregnancy as a key strategy to mitigate the intergenerational transmission of diabetes risk.
Early screening and management of impaired fasting glucose: A precision approach to preventing early-onset type 2 diabetes
Elevated fasting blood glucose (FBG) was one of the strongest predictors of early-onset T2DM, with a pooled odds ratio of 8.73 (95% CI: 4.91–16.92; I2 = 69.7%). This nearly ninefold increase underscores the pivotal role of impaired fasting glucose (IFG) in accelerating disease onset among younger individuals. Cohort studies yielded more consistent results than cross-sectional designs, supporting the robustness of this association.
The contribution of IFG to early-onset diabetes appears distinct from that in late-onset cases. While dysglycemia is a common risk factor across age groups, younger patients demonstrate more rapid β-cell decline and earlier development of insulin resistance.71–73 Mechanistic studies have shown that individuals with IFG often exhibit subclinical β-cell dysfunction long before overt diabetes is diagnosed. 74 Genetic predisposition, epigenetic alterations, and adverse early-life metabolic exposures may further accelerate this progression.
Clinically, elevated FBG should be regarded as a critical early warning signal. Screening for IFG provides an opportunity for timely intervention before the onset of diabetes. Lifestyle modification—including dietary change, increased physical activity, and weight control—remains the foundation of prevention, while pharmacological approaches such as metformin may be considered in high-risk individuals. Compared with late-onset disease, early-onset T2DM may warrant more intensive monitoring and earlier therapeutic intervention to mitigate its long-term complications.
Family history as a stronger risk factor for early-onset type 2 diabetes compared to general diabetes
Our analysis revealed that a family history of diabetes significantly elevates the risk of early-onset T2DM (OR = 4.54, 95% CI: 2.31–8.90), albeit with substantial heterogeneity (I2 = 93.2%). This finding is consistent with previous studies that consistently identify family history as a significant predictor of diabetes risk, with a more pronounced effect when the disease manifests at younger ages.75,76
The observed effect likely stems from both inherited susceptibility and shared environmental factors. Genetic variants associated with insulin resistance and β-cell dysfunction have been demonstrated to have a greater impact in early-onset disease, while family-level dietary habits, physical activity levels, and socioeconomic conditions may exacerbate this risk 76 . Collectively, these elements hasten the onset of T2DM in individuals with a familial predisposition.
It is important to note a limitation: most studies did not specify whether diabetes in family members was early- or late-onset, introducing uncertainty regarding whether parental early-onset diabetes confers an even greater risk. Further research with more detailed family medical histories is required to elucidate this relationship.
From a clinical standpoint, individuals with a family history of diabetes should be considered a priority group for preventive measures. Recommended interventions encompass lifestyle changes, routine metabolic screenings, and, when appropriate, early pharmacological interventions to delay or prevent the progression of the disease.77,78
Ethnic differences in risk factors for early-onset type 2 diabetes
Ethnic variation may also shape the determinants of early-onset T2DM. In our analyses, the associations of family history and BMI with early-onset T2DM appeared stronger in Asian populations compared with non-Asian cohorts, suggesting that genetic susceptibility and reduced β-cell function may play a more prominent role in Asian groups. This pattern is consistent with previous evidence indicating that Asians develop diabetes at comparatively lower BMI thresholds, reflecting impaired insulin secretory capacity despite modest adiposity. By contrast, in non-Asian populations, obesity-related insulin resistance has been more widely recognized as the dominant driver.
These observations underscore the need for ethnicity-specific prevention strategies. For Asian populations, where the disease burden is rapidly increasing, early screening among individuals with a family history of diabetes and maintaining healthy weight even at relatively low BMI levels may be particularly important. In Western populations, interventions focusing on obesity reduction and lifestyle modification are likely to remain the most effective. Taken together, both our findings and prior evidence highlight that ethnic background should be considered when designing strategies for the prevention and management of early-onset T2DM.
Early-onset versus late-onset T2DM: Risk factors and mechanisms
This meta-analysis identified key differences in risk factors between early-onset and late-onset T2DM. We found that family history was a significantly stronger risk factor for early-onset T2DM (OR = 4.54, 95% CI: 2.31–8.90), indicating that individuals with a family history of diabetes are at a much higher risk of developing the disease at a younger age. In contrast, the association between family history and late-onset T2DM was weaker, suggesting that age-related factors and insulin resistance become more influential in older populations.
Similarly, BMI was a more prominent risk factor for early-onset T2DM (OR = 2.87, 95% CI: 2.22–3.80). This shows that younger individuals, even with lower BMI, are at a higher risk compared to older populations. For late-onset T2DM, the risk is more associated with obesity-related insulin resistance, which is typically more severe in older adults. Additionally, elevated fasting blood glucose (FBG) was significantly linked to early-onset T2DM(OR = 8.73,95% CI: 4.91–16.92). This finding supports the idea that high FBG in younger individuals acts as an early warning sign of T2DM onset. These findings highlight that early-onset T2DM is not simply diabetes at a younger age but rather a more aggressive form of the disease with faster progression and earlier complications. Genetic predisposition, insulin resistance, and β-cell dysfunction appear to drive early-onset T2DM, whereas in late-onset cases, aging-related factors tend to play a more prominent role. 79
In clinical practice, early-onset T2DM requires early screening and more intensive management. Regular screening, along with early intervention through lifestyle changes and pharmacological treatments (e.g., metformin), is critical to slowing disease progression and preventing complications. Early-onset T2DM should be closely monitored and treated more aggressively than late-onset cases, given the faster disease progression in younger individuals. 80
Study limitations
This meta-analysis has several limitations that should be considered when interpreting the findings. First, the inclusion of studies was limited to those published in Chinese and English. This language restriction may have excluded relevant studies published in other languages, potentially leading to selection bias and incomplete representation of the global evidence base. As a result, the findings may not fully represent the diversity of populations and settings worldwide.
Second, the included studies consist of a mix of cross-sectional studies, case-control studies, and cohort studies. While these study designs provide valuable insights, cross-sectional and case-control studies inherently have weaker ability to establish causality compared to cohort studies. Cross-sectional studies capture associations at a single point in time and cannot determine temporal relationships, while case-control studies are prone to recall and selection biases. These design limitations weaken the strength of the evidence for causal relationships between risk factors and early-onset type 2 diabetes (T2DM).
Additionally, the evidence summarized in this meta-analysis exhibits substantial heterogeneity, as indicated by the variability in study populations, methodologies, and reported outcomes. High heterogeneity complicates the interpretation of pooled results and reduces their generalizability to clinical practice. Consequently, healthcare professionals should exercise caution when applying these findings in clinical decision-making, and individual patient contexts should always be considered.
To address these limitations and strengthen the evidence base, future research should prioritize large-scale, high-quality cohort studies. Cohort studies are essential for establishing temporal relationships and causality, as they allow for the prospective tracking of risk factors and outcomes over time. Moreover, expanding the geographic and linguistic scope of future studies would provide a more comprehensive understanding of early-onset T2DM across diverse populations. Such research efforts would help clarify the underlying relationships between risk factors and disease onset, ultimately improving the accuracy and applicability of clinical guidelines for early detection and prevention of early-onset T2DM.
Future directions
Given the heightened risk and familial predisposition of early-onset T2DM, future research should focus on early intervention strategies targeting high-risk groups. Prenatal and early-life factors, such as maternal gestational diabetes and childhood obesity, warrant particular attention. Early lifestyle interventions, including dietary modifications and physical activity, can significantly reduce the risk of T2DM in susceptible individuals. Genetic screening and counseling may also play a pivotal role in identifying and managing at-risk populations. Collaborative efforts between healthcare providers, researchers, and health policymakers are essential to develop and implement effective prevention and management programs tailored to the needs of individuals with or at risk for early-onset T2DM.
In conclusion, our findings emphasize the critical need for early identification and intervention in individuals at risk for early-onset T2DM. Addressing modifiable risk factors, understanding genetic predispositions, and implementing targeted prevention strategies can mitigate the burden of T2DM and improve long-term health outcomes for younger populations.
Conclusion
In summary, sociodemographic factors such as male sex, family history of diabetes, maternal gestational diabetes, high body mass index (BMI); lifestyle factors such as smoking and lack of physical activity; and disease factors such as hypertension, acanthosis nigricans, high cholesterol, and elevated fasting blood glucose are risk factors for the early-onset type 2 diabetes. In the face of manifold risk factors, multi-level prevention strategies with tailored lifestyle interventions, where needed, are likely to have greater success.
Supplemental Material
Supplemental Material - Risk factors of early-onset type 2 diabetes: A systematic review and meta-analysis
Supplemental Material for Risk factors of early-onset type 2 diabetes: A systematic review and meta-analysis by Shengying Hu, Yizhu Zhang, Angela C. Y. Poon, Yan Ji, Botian Hou, Chenye Zhang, Hongyu Sun, Yumei Sun in Diabetes & Vascular Disease Research
Supplemental Material
Supplemental Material - Risk factors of early-onset type 2 diabetes: A systematic review and meta-analysis
Supplemental Material for Risk factors of early-onset type 2 diabetes: A systematic review and meta-analysis by Shengying Hu, Yizhu Zhang, Angela C. Y. Poon, Yan Ji, Botian Hou, Chenye Zhang, Hongyu Sun, Yumei Sun in Diabetes & Vascular Disease Research
Supplemental Material
Supplemental Material - Risk factors of early-onset type 2 diabetes: A systematic review and meta-analysis
Supplemental Material for Risk factors of early-onset type 2 diabetes: A systematic review and meta-analysis by Shengying Hu, Yizhu Zhang, Angela C. Y. Poon, Yan Ji, Botian Hou, Chenye Zhang, Hongyu Sun, Yumei Sun in Diabetes & Vascular Disease Research
Supplemental Material
Supplemental Material - Risk factors of early-onset type 2 diabetes: A systematic review and meta-analysis
Supplemental Material for Risk factors of early-onset type 2 diabetes: A systematic review and meta-analysis by Shengying Hu, Yizhu Zhang, Angela C. Y. Poon, Yan Ji, Botian Hou, Chenye Zhang, Hongyu Sun, Yumei Sun in Diabetes & Vascular Disease Research
Footnotes
CRediT contributions statement
Author contributions Study design: Shengying Hu. Search strategy, study selection, data extraction, assessment of methodological quality, data analysis: Shengying Hu, Yizhu Zhang, Botian Hou, Chenye Zhang. Grading the quality of evidence: Shengying Hu, Yizhu Zhang. Supervision: Hongyu Sun, Yumei Sun. Writing—original draft preparation: Shengying Hu. Writing—review and editing: Angela CY Poon, Yan Ji.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Program of China (Grant No. 2023YFC3604605).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.