
Abstract
Objective
We aimed to explored the association between atherogenic index of plasma (AIP), body mass index (BMI) and stroke risk among people with abnormal glucose metabolism.
Methods
This study included participants with abnormal glucose metabolism from the China Health and Retirement Longitudinal Study (CHARLS). AIP was computed using the formula log (Triglyceride/High-density lipoprotein cholesterol). Participants were categorized into high and low levels based on median values for both AIP and BMI. Logistic regression models were employed to investigate the associations between AIP, BMI, and stroke.
Results
In the longitudinal analysis, 195 out of 3,682 individuals (5.3%) experienced stroke. Joint effects of AIP and BMI on stroke risk indicated that odds ratios for stroke were 1.41 (0.86-2.31) for high AIP & low BMI group, 1.81 (1.14-2.89) for low AIP & high BMI group, and 2.15 (1.42-3.27) for high AIP & high BMI group when compared to low AIP & low BMI group. A significant interaction was observed between AIP and BMI regarding stroke risk. However, this association appeared diminished within cross-sectional evaluations.
Conclusion
Elevated levels of both AIP and BMI are significantly correlated with an increased risk of stroke among individuals exhibiting abnormal glucose metabolism during longitudinal analysis.
Introduction
Abnormal glucose metabolism primarily encompasses both diabetes and prediabetes, with the transitional state between diabetes and normal blood glucose levels referred to as prediabetes. 1 The data from the International Diabetes Federation shows that 589 million adults worldwide have diabetes, while an additional 1120 million are classified as having prediabetes in 2024. 2 The progression of abnormal glucose metabolism often leads to various vascular complications, among which stroke is particularly concerning due to its high mortality rate and significant adverse effects on quality of life. 3 Individuals with diabetes face a risk of stroke that is approximately 1.5 to 2 times greater than that of those maintaining normal blood glucose level. 4 Moreover, the increased stroke risk associated with prediabetes warrants attention; research indicates that individuals in this category already experience heightened risks for all-cause mortality and cardiovascular disease. 5 Studies have shown that more than two-thirds of chronic stroke patients and more than one-third of acute stroke patients exhibited abnormalities in glucose metabolism.6,7 Epidemiological evidence robustly supports the link between abnormal glucose metabolism and stroke, establishing it as an independent risk factor for this condition. 8 Consequently, effectively identifying and intervening with individuals at high risk for stroke within the population exhibiting abnormal glucose metabolism is essential for mitigating their overall stroke risk.
In addition to hyperglycemia, people with abnormal glucose metabolism are often combined with obesity and abnormal lipid metabolism, both of which may contribute to an elevated risk of stroke.9,10 Obesity, commonly defined as a body mass index (BMI) ≥30 kg/m2, has long been recognized as a significant risk factor for stroke in the general population, with insulin resistance playing a crucial role in this association. 11 In recent years, Atherogenic index of plasma (AIP), calculated as the logarithm of the ratio of plasma triglycerides (TG) to high-density lipoprotein cholesterol (HDL-C), has also been found to be associated with an increased risk of stroke within the general population. 12 However, prior research has predominantly focused on single factor and relatively healthy individuals and has not adequately examined those with abnormal glucose metabolism, who is a demographic known to be at heightened risk for stroke. Furthermore, investigations into the combined effects of BMI and AIP on stroke risk remain limited, particularly among individuals exhibiting abnormal glucose metabolism.
Therefore, we used the data from the China Health and Retirement Longitudinal Study (CHARLS) to conduct a cross-sectional and longitudinal analysis for investigating the combined effects of BMI and AIP on stroke risk among people with abnormal glucose metabolism.
Methods
Study design and participants
The CHARLS study is a nationally representative longitudinal survey targeting individuals aged 45 years and older, recruited from 150 counties or districts and 450 villages across 28 provinces in China. Comprehensive details of the study design have been previously documented.13,14 In summary, the baseline survey for CHARLS was initiated in 2011 (wave 1), followed by four subsequent waves of data collection conducted in 2013 (wave 2), 2015 (wave 3), 2018 (wave 4), and most recently in 2020 (wave 5). During each wave, trained personnel performed face-to-face interviews to gather sociodemographic information, medical history, and health behaviors using standardized questionnaires for the participants. The CHARLS study adhered to the principles outlined in the Declaration of Helsinki and received approval from the Institutional Review Board at Peking University (IRB00001052-11015). All participants provided written informed consent.
The present study constitutes a secondary analysis of data derived from the CHARLS. Initially, we enrolled a total of 17,708 participants during wave 1. Abnormal glucose metabolism included diabetes and prediabetes. Among these participants, we identified a subset of 7,407 individuals with abnormal glucose metabolism based on specific criteria: prediabetes was defined as fasting plasma glucose (FPG) levels between 100–125 mg/dl or glycosylated hemoglobin A1c (HbA1c) levels ranging from 5.7% to <6.5%; diabetes was characterized by FPG ≥125 mg/dl or HbA1c ≥6.5%, self-reported medical history indicating diabetes diagnosis, or current use of antidiabetic medications.
15
Moreover, 1,577 participants with missing data for height, weight, HDL-C and TG were excluded in the cross-sectional study in 2011. We further excluded individuals with a history of stroke in 2011, or those with incomplete stroke-related data of stroke in the 2013, 2015, 2018, or 2020 waves. Ultimately, 3,682 participants were included in the longitudinal analysis, as illustrated in Figure 1. The flow chart of inclusion and exclusion.
Assessment of BMI and AIP
Trained nursing professionals measured height and weight for participants, and BMI calculated by dividing weight in kilograms by the square of height in meters. Fasting venous blood samples were collected by medical personnel from the Chinese Center for Disease Control and Prevention following standardized protocols, subsequently analyzed for TG and HDL-C using a Hitachi 7180 chemistry analyzer (Hitachi, Tokyo, Japan) at the Youan men Center for Clinical Laboratory of Capital Medical University. In accordance with previous studies, 16 AIP was computed as lg (TG/HDL-C). High and low levels were categorized based on the median values of AIP and BMI, resulting in four distinct groups: low AIP & low BMI, high AIP & low BMI, low AIP & high BMI, and high AIP & high BMI.
Outcome assessment
The primary outcome of interest in this study was the incidence of stroke, encompassing both cerebral infarction and hemorrhage. Self-reported stroke status was evaluated through questions such as: “Have you been diagnosed with stroke by a doctor”; “Since your last follow-up visit, have you received a diagnosis of stroke”; “In comparison to our last interview, is your stroke condition better, about the same, or worse”.
Covariates
In this study, sociodemographic characteristics and health-related data were considered as covariates. Sociodemographic variables encompassed age, sex (male, female), marital status (with spouse, without spouse), residence (rural, urban), and education level (elementary school or below, middle school, high school or above). Health-related factors included smoking status (never, former, current), drink status (yes, no), physical activity engagement (yes, no), depression history (yes, no), and a history of hypertension or coronary heart disease (CHD) (yes, no). Additionally, the use of antihypertensive medications, diabetes medications, or lipid-lowering therapies was recorded as binary variables (yes, no). To account for the influence of overall lipid levels on outcomes, total cholesterol (TC) was also included as a covariate.
Statistical analysis
Data are presented as means ± standard deviation (SD) or medians with interquartile ranges for continuous variables and percentages for categorical variables. Comparisons of baseline characteristics across four quadrants were conducted using one-way ANOVA or Kruskal Wallis rank-sum tests for continuous variables and χ2 tests for categorical variables. Logistic regression analysis was established to estimate the independent or joint effects of BMI and AIP on risk of stroke in the cross-sectional study, presented in odds ratios (ORs) and 95% confidence intervals (CIs). Moreover, a logistic regression model was employed to estimate the individual or joint effects of BMI and AIP on stroke incidence based on longitudinal data collected from 2011 to 2020. Various combinations of covariates were employed across three adjustment models. Model 1 was adjusted for age and sex; Model 2 included adjustments for age, sex, marital status, residence, educational level, smoking status, drinking status, and physical activity; while Model 3 further adjusted Model 2 by incorporating TC, depression history, a history of hypertension and CHD, as well as the use of antihypertensive medications, diabetes medications, and lipid-lowering therapies.
Furthermore, we investigated the multiplicative interaction to assess the combined effect of BMI and AIP on stroke risk. We also performed stratified analyses based on age (<60 years vs ≥60 years), sex (male vs female), residence (rural vs urban) and status of abnormal glucose metabolism (diabetes vs prediabetes). Additionally, several sensitivity analyses were conducted. Given that this study focused on a Chinese population context, we adopted the definition of overweight and above specific to this demographic, 17 classifying individuals with a BMI ≥24 kg/m2 as having a high level and those with a BMI <24 kg/m2 as having a low level for joint analysis purposes. Moreover, to account for potential confounding effects from pharmacological treatments, we excluded the participants utilizing blood pressure-lowering agents, glucose-lowering medications, and lipid-regulating therapies, respectively. All statistical analyses were conducted using STATA 17.0 software, and the significance level of statistical test is P < 0.05 in this study.
Results
Baseline characteristics of the study population
Baseline Characteristics of the Study Population divided by AIP and BMI in the Longitudinal Analysis.

Comparisons of the baseline characteristics across four quadrants are performed with one-way ANOVA or Kruskal-Wallis’s rank sum tests for continuous variables and χ2 tests for categorical variables. Abbreviations: TC, Total cholesterol; SBP, Systolic blood pressure; DBP, Diastolic blood pressure; CHD, Coronary heart disease; BMI, Body mass index; AIP, Atherogenic index of plasma.
Independent and joint effect of AIP and BMI on risk of stroke
Adjusted odds ratios (ORs) and 95 confidence intervals (95 CIs) of stroke according to AIP and BMI in the longitudinal analysis.
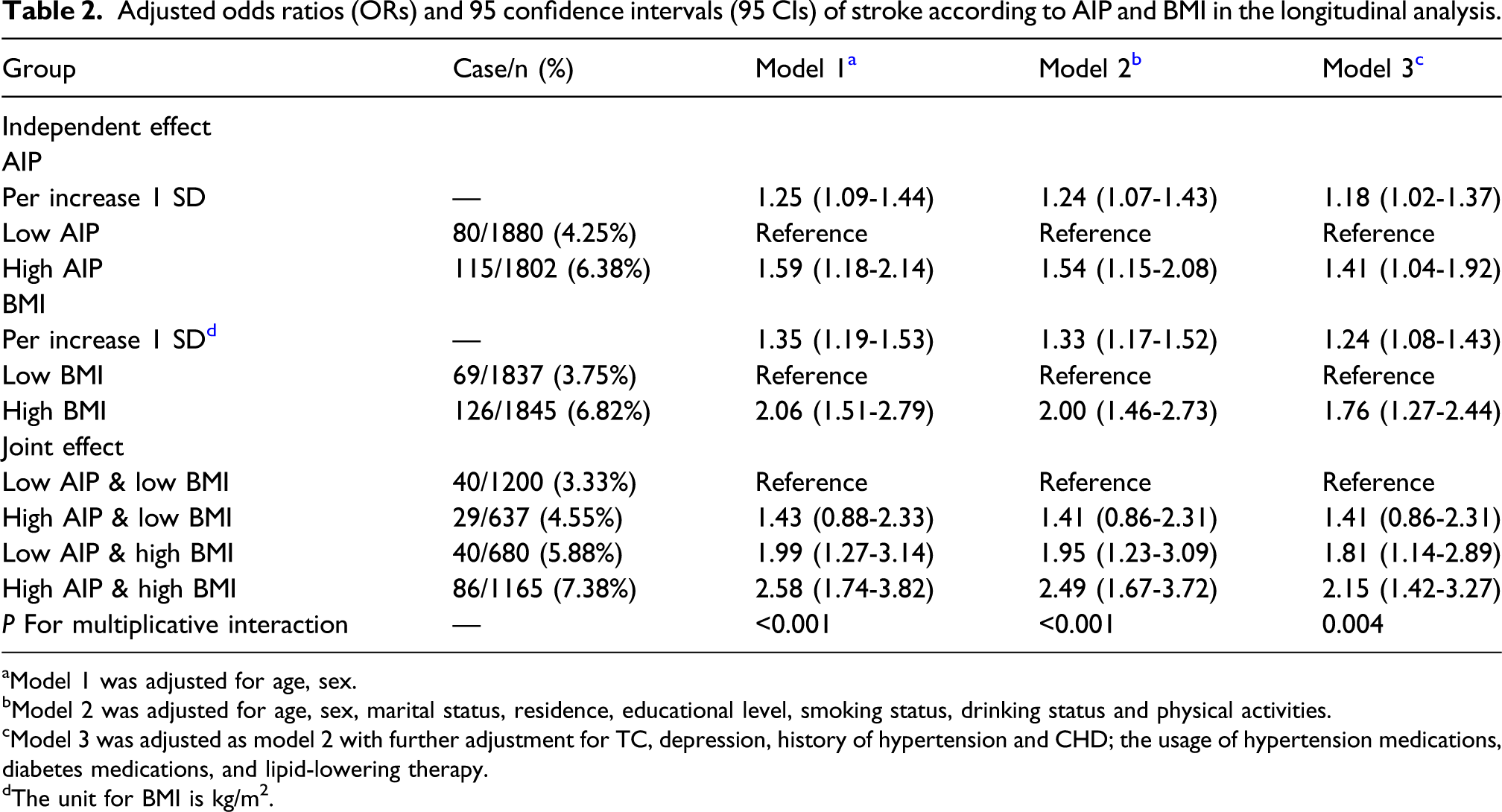
aModel 1 was adjusted for age, sex.
bModel 2 was adjusted for age, sex, marital status, residence, educational level, smoking status, drinking status and physical activities.
cModel 3 was adjusted as model 2 with further adjustment for TC, depression, history of hypertension and CHD; the usage of hypertension medications, diabetes medications, and lipid-lowering therapy.
dThe unit for BMI is kg/m2.
Subgroup and sensitivity analyses
The results of the subgroup analysis on the longitudinal data were presented in Figure 2. We observed that the combined effect of AIP and BMI on stroke risk was significant when interacting with age (P for interaction = 0.016), sex (P for interaction = 0.029), area of residence (P for interaction = 0.041) and status of abnormal glucose metabolism (P for interaction = 0.015). The joint effect of AIP and BMI on incident stroke seems to be pronounced in the older people, male, individuals who live in urban areas and diabetes. Additionally, after adopting the definition of overweight and above (BMI ≥24 kg/m2) in the Chinese population to divided the BMI group, the results did not change substantially (Table S3). Furthermore, the results of excluding the participants utilizing blood pressure-lowering agents, glucose-lowering medications, or lipid-regulating therapies were still consistent with those of the main analysis (Table S4-S5). Stratification analysis of associations between AIP and BMI and incident stroke. The multivariable model (Model 3) was adjusted for age, sex, marital status, residence, educational level, smoking status, drinking status, physical activities, TC, depression, history of hypertension and CHD; the usage of hypertension medications, diabetes medications, and lipid-lowering therapy. Stratification variables were mutually adjusted.
Discussion
This extensive nationwide longitudinal study aimed to investigate the independent and combined effects of BMI and AIP on stroke risk among individuals with abnormal glucose metabolism. Our findings indicate that both elevated levels of AIP and BMI are significantly associated with an increased risk of stroke in this population during longitudinal analysis, but this association weakened in cross-sectional assessments. Notably, the joint effect of AIP and BMI demonstrated a significant multiplicative interaction concerning incident stroke within the longitudinal framework. Furthermore, these results remained robust across subgroup and sensitivity analysis.
To our knowledge, prior evidence regarding the joint impact of AIP and BMI on incident strokes among individuals with abnormal glucose metabolism is limited. Several studies have established a correlation between elevated BMI and heightened stroke risk.11,18 A meta-analysis encompassing 44 prospective cohort studies reported a summary relative risk for stroke incidence at 1.10 (95% CIs: 1.06 to 1.13) per 5-unit increment in BMI. 19 Consistent with these findings, our analysis revealed that each SD increase in BMI corresponds to an ORs for stroke of 1.24 (95% CIs: 1.08 to 1.43) among those with abnormal glucose metabolism. Additionally, Zheng H et al. found that high cumulative AIP correlates with an increased ischemic stroke risk within the general population using data from the Kailuan study. 12 Another prospective cohort investigation indicated that rising AIP levels are significantly linked to stroke risk in middle-aged and elderly populations while exhibiting distinct characteristics based on individual glucose metabolism status. 20 In our assessment of the individual effect of AIP on stroke risk, we also identified a positive association between elevated AIP levels and increased stroke risk among individuals with abnormal glucose metabolism. However, previous research has predominantly focused on isolated factors influencing stroke risk within general populations rather than examining their interactive effects specifically in those experiencing altered glucose metabolism conditions. In contrast, our study elucidates how concurrent increases in both AIP and BMI substantially elevate the likelihood of strokes amongst individuals facing abnormalities in glucose processing mechanisms. We observed that elevated AIP and BMI levels were significantly associated with an increased risk of stroke in this population in the longitudinal analysis cohort, but this association was not significant in the cross-sectional assessment. The cross-sectional assessment only included stroke patients who were still alive at a certain point in time, which may have been affected by survivor bias or changes in disease exposure status, resulting in insignificant results.
Importantly, recognizing the multiplicative interaction between AIP and BMI underscores their potential synergistic contribution to heightened stroke risks in the longitudinal analysis. It is suggested to regular monitoring AIP and BMI level may serve as an effective strategy for identifying at higher risk of stroke in the population with abnormal glucose metabolism, thereby providing novel insights into clinical preventive measures against stroke.
The findings from the subgroup analysis of this study indicate that the combined effects of AIP and BMI on stroke risk among individuals with abnormal glucose metabolism vary by age, sex, residence area and status of abnormal glucose metabolism. We observed significant interactions between the joint influences of AIP and BMI on stroke risk in relation to these factors. Notably, our results revealed that older, and male who exhibit elevated levels of both AIP and BMI are at a heightened risk for stroke compared to their younger, and female counterparts, suggesting that this association is particularly pronounced in older, and male with abnormal glucose metabolism. Age and sex are critical determinants in the pathology of stroke, especially ischemic stroke. 21 Stroke is predominantly an age-related condition, exhibiting increased incidence rates among individuals over 65 years old. 22 Older patients experience higher mortality rates and diminished quality of life post-stroke when compared to younger patients.23,24 Furthermore, gender differences also influence both incidence and outcomes related to stroke. Previous studies have demonstrated that male generally face a greater lifetime incidence of strokes than female. 25 Consequently, our findings further underscore the necessity for enhanced monitoring and intervention strategies targeting both AIP and BMI levels in older, and male population with abnormal glucose metabolism to effectively mitigate their risk for stroke.
The mechanisms underlying the joint effect of BMI and AIP on stroke risk in individuals with abnormal glucose metabolism remain poorly understood; however, several contributing factors may be implicated. Firstly, obesity often correlates with insulin resistance which disrupts glucose and lipid metabolism—this can lead to vascular narrowing thereby increasing susceptibility to stroke. 26 Secondly, AIP serves as a novel biomarker reflecting atherosclerosis severity 27 ; prior research has established its close relationship with small dense low-density lipoprotein (sd-LDL). 28 Elevated levels of AIP tend to correlate with increased sd-LDL concentrations which are more prone to adhere to arterial walls—this exacerbates atherosclerosis further elevating stroke risks. 29 Lastly, concurrent elevations in both AIP and BMI suggest that insulin resistance along with associated hyperinsulinemia, hyperglycemia, and dyslipidemia promote adipocytokine release leading ultimately to vascular endothelial dysfunction as well as inflammation, and these processes collectively facilitate the onset and progression of strokes among those experiencing abnormal glucose metabolism.
The primary significance of this study lies in the identification of a positive correlation between elevated levels of both AIP and BMI with the risk of stroke in individuals exhibiting abnormal glucose metabolism, as well as the practical implications of their multiplicative interaction. Data from the global burden of disease study indicate a continuous rise in both abnormal glucose metabolism and stroke prevalence in recent years. 30 These two conditions frequently coexist and exert mutual influence. Stroke remains a leading cause of mortality and disability among patients with abnormal glucose metabolism, significantly exacerbating poor prognoses and increasing mortality rates for these individuals.31,32 Prior research has demonstrated that managing stroke risk factors, such as blood sugar, BMI, and lipid levels, could mitigate risk of stroke.33,34 However, current control measures for blood glucose, BMI, and lipid levels among those with abnormal glucose metabolism remain suboptimal, representing a substantial potential burden for stroke risk.35,36 Our findings suggest that individuals with both elevated BMI and AIP values may face an increased stroke risk compared to those exhibiting elevation in only one variable. This observation carries important implications for clinical practice and risk stratification within this population. By identifying people at high risk of stroke through comprehensive assessments of BMI and AIP levels, more targeted prevention strategies could be developed.
This study exhibits several notable strengths, including its status as the first large-scale longitudinal investigation to examine the joint effects of BMI and AIP levels on stroke risk among individuals with abnormal glucose metabolism. Additionally, it utilized data from CHARLS, a comprehensive and representative cohort of the Chinese population that undergoes regular long-term monitoring. Such extensive follow-up is crucial for accurately assessing longitudinal associations, particularly those pertaining to BMI, AIP levels, and their combined impact on stroke risk. However, this study also has several limitations that warrant consideration. First, being an observational study precludes it from fully eliminating residual confounding or establishing causality. Nonetheless, we have made efforts to adjust for potential confounders as thoroughly as possible. Furthermore, some unmeasured confounding factors, such as dietary factors, and the specific numerical levels of physical activity, might influence the association between both BMI/AIP and stroke risk. Second, stroke information was derived from self-reported sources without specific classification criteria, while this limitation may restrict the clinical applicability of our findings to some extent, self-reported disease data are generally acceptable in large cohort studies and previous research has demonstrated a reliable correlation between self-reported stroke history and medical records. 37 Third, our analysis focused solely on single measurements of AIP and BMI levels without investigating whether long-term fluctuations in these variables consistently influence outcomes, so further research is warranted in this area. Finally, since our results primarily pertain to the Chinese population, caution should be exercised when generalizing these findings to other countries or regions.
Conclusions
This study underscored that co-elevated BMI and AIP levels are significantly associated with an increased risk of stroke in individuals with abnormal glucose metabolism within longitudinal analyses and may exhibit a synergistic effect. Furthermore, this association appears more pronounced among older adults, male, urban residents and diabetes. These findings emphasize the clinical importance of enhanced monitoring and intervention regarding AIP and BMI levels in individuals with abnormal glucose metabolism to mitigate the incidence of stroke events.
Supplemental Material
Supplemental material - Combined effect of body mass index and Atherogenic index of plasma on risk of stroke among individuals with abnormal glucose metabolism: Evidence from the China health and retirement longitudinal study
Supplemental material for Combined effect of body mass index and Atherogenic index of plasma on risk of stroke among individuals with abnormal glucose metabolism: Evidence from the China health and retirement longitudinal study by Yushan Liao, Liheng Chen, Jinshen Huang, Haiqiong Liu, Zehua Li, Jing Yan, Yanbin Cai, Yu Sun, Wen Jin and Jingbin Guo in Diabetes and Vascular Disease Research.
Footnotes
Ethical considerations
The study was approved by the Biomedical Ethics Review Committee of Peking University (IRB00001052-11015), and informed consent was obtained from all participants.
Author contribution
Y.-S.L., and J.-B.G. were integral to the conception, design, and conduct of the study. Y.-S.L., L.-H.C, J.-S.H., Z.-H.L., J.Y., Y.-B.C, and Y.S., were involved in the acquisition, analysis, and interpretation of the data. Y.-S.L., L.-H.C, J.-S.H., H.-Q.L., and W.J., contributed to the drafting the manuscript. All authors participated in reviewing, editing, and providing approval for the final version of the manuscript. J.-B.G. assume the role of guarantors for this work, thereby possessing full access to all study data, shouldering responsibility for data integrity, and ensuring the precision of data analysis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.