
Abstract
Objective
This observational study assesses trends in type 1 diabetes mellitus (T1DM) disease burden across the 19 countries of the European Union (EU) 15+ between 1990 and 2019.
Methods
The Global Burden of Disease Study database was used to gather T1DM age-standardised incidence (ASIR), prevalence (ASPR), mortality (ASMR), and disability-adjusted life-year (DALY) rates per 100,000 for each EU15+ country (1990 – 2019). Joinpoint regression analysis was used to describe the trends.
Results
From 1990 to 2019, T1DM ASIRs and ASPRs increased globally except for females in Finland (−2.9% and −9.4%), the largest increase in ASPR for males and females was observed in France (+144.4% and +137.5% respectively). All had reductions in ASMRs for males and females, with the largest observed in Spain (−56.7% and −79.0% respectively). Trends in DALYs were variable across countries, with increases in DALYs noted in 14/19 for males, and 9/19 for females. Denmark, Finland, Norway, Netherlands, and Sweden had a reduction in DALYs for both males and females.
Conclusions
Mortality from T1DM is reducing across EU15+ countries, despite concomitant increases in incidence and prevalence rates. Trends in DALYs are variable across countries, reflecting differential trends in the disease burden across countries with similarly high health expenditure.
Introduction
In 2017, the International Diabetes Federation’s (IDF) global estimate for the number of people under the age of 20 living with type 1 diabetes mellitus (T1DM) was 1,106,200, with a significant proportion residing in Europe (estimated at 286,000). 1 T1DM poses a significant financial burden upon health services, with the UK’s National Health Service (NHS) spending an estimated £1.9 billion on the disease in 2012. This figure is predicted to rise to £4.2 billion by 2035/36. 2
Over recent decades, increasing trends in the incidence and prevalence of T1DM have been reported by international collaborations such as the worldwide DIAMOND Project and the European EURODIAB study.3,4 Prevalence rates are projected to continue to increase globally posing further impact on T1DM burden of disease. 1 Specific comparisons of the disease burden from T1DM across high health expenditure countries using data obtained from the Global Burden of Disease (GBD) database are lacking.
The objective of this study was to extract and compare trends in T1DM age-standardised incidence rates (ASIRs), age-standardised prevalence rates (ASPRs), age-standardised mortality rates (ASMRs), mortality-to-incidence indices (MIIs), and disability-adjusted life-year (DALYs) rates across a group of countries with similarly high health expenditure, namely the European Union (EU) 15+ over the last three decades.
Research design and methods
Characteristics of the data source
The GBD Study database was used as the source of data. T1DM age standardised ASIR, ASPR, ASMR, and DALY rates data were extracted from the GBD online data repository (https://ghdx.healthdata.org/gbd-results-tool) for each of the 19 EU15+ countries for the years 1990–2019. Age-standardised rates were used to improve comparability between countries by accounting for each countries’ population age-profiles. Age-standardisation is calculated by adjusting to a standard world population from the United Nations Population Division’s World Population Prospects (2012 revision).
EU15+ countries were chosen as the cohort for comparison for two main reasons: firstly, this group of countries has been used previously in comparative observational analyses because of their similarly high health expenditure. Secondly, the data available for each of the EU15+ countries is of high quality. Indeed, the GBD study authors assess the quality of data available for all countries worldwide, based on the accessibility and completeness of vital registration (VR) and verbal autopsy (VA) data: all EU15+ countries have >/= 90% completeness of VR and VA data for every year from 1990 to 2019.
The data sources and modelling strategy used by the GBD study authors are outlined in detail in the most recently updated manuscript of the GBD Study. 5 Different models are used to calculate mortality, incidence, prevalence, and DALY rates, which are discussed in brief below.
The GBD study uses disease registries, survey data, systematic reviews, case notifications, and hospital administrative data (inpatient and outpatient claims) as data sources for estimations of incidence and prevalence rates. Specifically, for T1DM, the GBD collaborators incorporated all data pertaining to T1DM, juvenile-onset diabetes, and insulin-dependent diabetes from diabetic registries and estimates of T1DM in representative populations. It was assumed that all T1DM is diagnosed under 15 years of age, and that all diabetes patients under 15 years of age have T1DM. T1DM incidence and prevalence input data were processed with DisMod-MR 2.1 to account for systemic biases. T1DM prevalence rates incorporated study-level co-variates and case-specific mortality using CODEm in addition to DisMod-MR 2.1 processing.
In the GBD Study, mortality data are collated into a cause of death database from seven sources (VA, VR, cancer registries, police records, sibling history, surveillance, and survey/census data). Cause-specific mortality rates are then modelled using the cause of death ensemble modelling (CODEm) framework. For T1DM, type specific mortality data was only available from vital registration source coded by the International Classification of Diseases code, 10th revision (ICD10) (codes E10–E10.1, E10.3–E10.9, and P70.2). Verbal autopsy or ICD 9th revision data was not available. The CODEm model for T1DM set the age range 0–95+ years, whereas type 2 diabetes model set the age-range to 15–95+ years. Thus, the GBD methodology assumes all deaths under 15 years old are from T1DM (regardless of the ICD10 code assigned). Deaths from unspecified diabetes type (as coded by ICD10) were distributed to T1DM using meta-regression. Neonatal diabetes mortality was included with T1DM mortality.
DALYs are calculated by the GBD collaborators using an equation incorporating the sum of years of life lost (YLL) and the years of life lived with disability (YLD). GBD methodology computes YLL by multiplying the standard life-expectancy at the age of death by the estimated number of deaths (per cause). Deaths at younger ages are therefore highlighted as larger weight is applied (since standard life-expectancy is greater). YLD is calculated by the prevalence of T1DM (estimated by DisModMR 2.1) multiplied by that same disease’s disability weighting (from European disability weights measurement study). 6
Statistical analysis
Trends in incidence, prevalence, mortality, and DALYs were assessed using Joinpoint regression analysis (Joinpoint Command Line Version 4.5.0.1 provided by the United States National Cancer Institute Surveillance Research Program). 7 Joinpoint software observes data trends over time, connects line segments together on a logarithmic scale using the simplest possible model. Each line segment, or ‘Joinpoint,’ represents an observed trend. As Joinpoints are added to the model they are tested for significance using a Monte Carlo permutation method. Estimated annual percentage changes (EAPC) (and 95% confidence intervals) are given for each line segment and are tested for significance against the null hypothesis of no change.
Finally, to provide an estimation of population based case-fatality rates, mortality to incidence indices (MIIs) were computed, by dividing the annual ASMRs the respective ASIRs, for each sex, location, and year (1990–2019 inclusive). MIIs have been used previously as a crude indicator of relative survival and have demonstrated good correlation with cancer outcomes.8,9
Results
Changes were observed for T1DM ASIRs, ASPRs, ASMRs, MIIs, and DALYs over the 30-year period in all 19 EU15+ countries.
Trends in T1DM age-standardised rates
Incidence: Table 1 and Figure 1
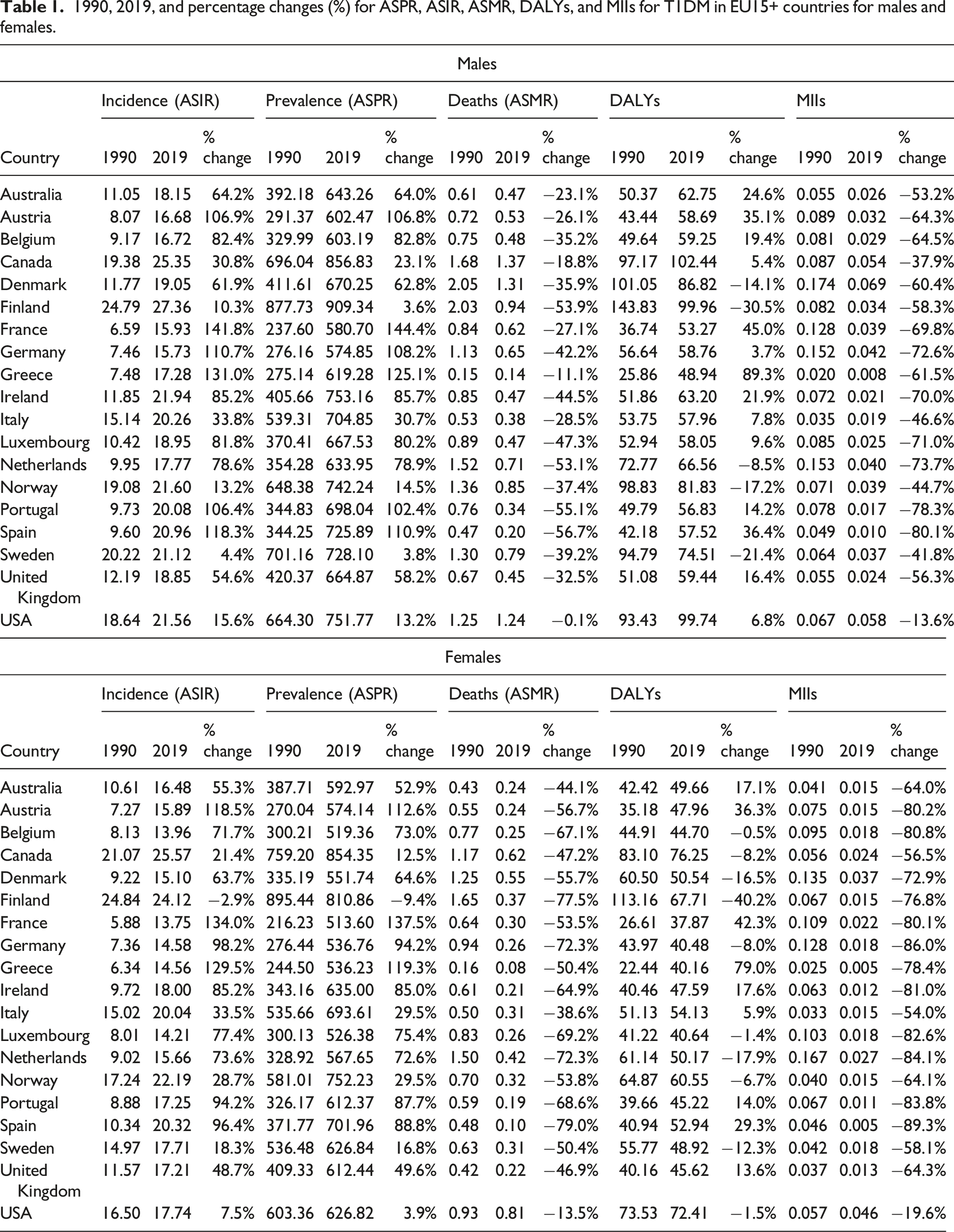
1990, 2019, and percentage changes (%) for ASPR, ASIR, ASMR, DALYs, and MIIs for T1DM in EU15+ countries for males and females.

Trends of T1DM age-standardised prevalence rates (ASPR) per 100 000 in EU15+ countries between 1990 and 2019, for males (unfilled squares) and females (filled squares).
Prevalence: Table 1 and Figure 2
The highest 2019 ASPRs for males were seen in Finland (909.34/100,00), and in Canada for females (854.35 in 100,000). The lowest ASPRs for males were observed in Germany (574.85/100,000), and France for females (513.6/100,000). For all countries excluding Norway, ASPRs were higher in males than females in 2019. Trends of T1DM age-standardised mortality rates (ASMR) per 100 000 in EU15+ countries between 1990 and 2019, for males (unfilled squares) and females (filled squares).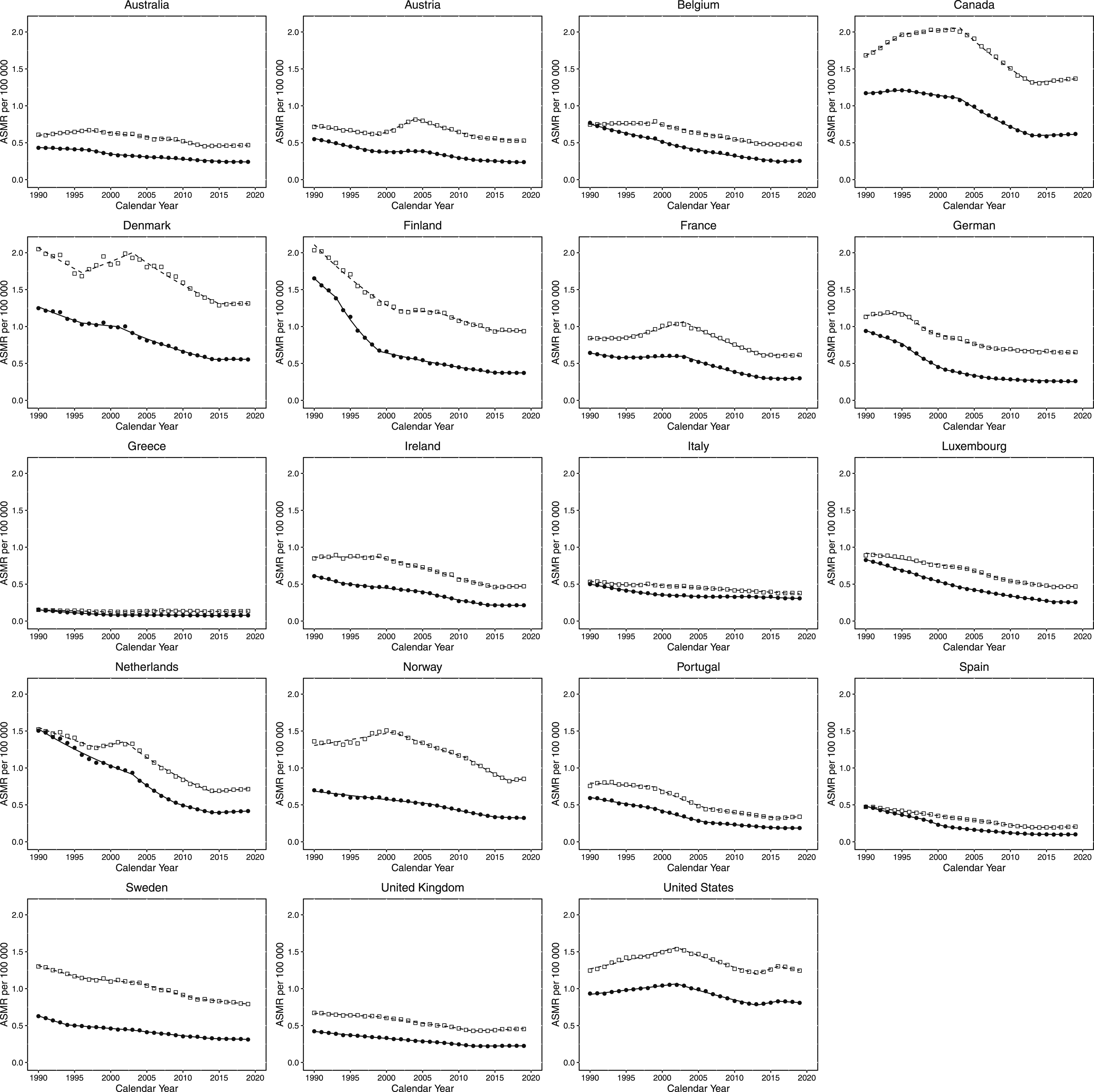
Mortality: Table 1 and Figure 3
The highest 2019 ASMRs for males were seen in Canada (1.37/100,000), and in the USA for females (0.81/100,000). The lowest 2019 ASMRs were observed in Greece for both males and females (0.14 and 0.08/100,000 respectively). For all countries, ASMRs were higher in males than females in 2019. Trends of T1DM disability adjusted life year rates (DALYs) per 100 000 in EU15+ countries between 1990 and 2019, for males (unfilled squares) and females (filled squares).
Mortality-to-incidence indices: Table 1
The highest 2019 MIIs for males were seen in Denmark (0.069), and in the USA for females (0.046). The lowest 2019 MIIs were observed in Greece for males (0.008), and in Greece and Portugal for females (0.005). For all countries, MIIs were higher in males than females in 2019.
Age-standardised disability-adjusted life-years: Table 1
The highest 2019 DALYs for males and females were seen in Canada (102.44 and 76.25/100,000 respectively). The lowest 2019 DALYs for males were observed in Greece (48.94/100,000), and in France for females (37.87/100,000). For all countries, DALYs were higher in males than females in 2019.
Age-standardised incidence rates: Table 1 and Figure 1
Relative increases in ASIRs were demonstrated for all countries over the 30-years observation period for both sexes (except for females in Finland who observed relative reductions in T1DM ASIR of −2.9%). The smallest relative increase in ASIR for males were observed in Sweden (+4.4%). The greatest relative increase in ASIR for males and females was observed in France (+141.8% and +134.0% respectively).
Age-standardised prevalence rates: Table 1 and Figure 2
Relative increase in ASPRs were demonstrated for all countries over the 30-years observation period for both sexes (except for females in Finland who saw a relative reduction of −9.4%). The greatest relative increases in ASPR for males and females were observed in France (+144.4% and +137.5% respectively). The smallest relative increase in ASPR for males was observed in Finland (+3.6%).
Age-standardised mortality rates: Table 1 and Figure 3
Relative reductions in ASMRs were demonstrated for all countries over the 30-years observation period for both sexes. The smallest relative reductions in ASMR for males and females were observed in the USA (−0.1% and −13.5% respectively). The greatest relative reductions in ASMR for males and females were observed in Spain (−56.7% and −79.0% respectively).
Mortality-to-incidence indices: Table 1
Relative reductions in MIIs were demonstrated for all countries over the 30-years observation period for both sexes. The smallest relative reductions in MIIs for males and females were observed in the USA (−13.6% and −19.6% respectively). The greatest relative reductions in MIIs for males and females were observed in Spain (−80.1% and −89.3% respectively).
Age-standardised disability-adjusted life-years: Table 1
Relative reductions were demonstrated in 5 and 10 of the 19 EU15+ countries investigated over the 30-years observation period (for males and females respectively). The greatest relative reductions in DALYs for males and females were observed in Finland (−30.5% and −40.2% respectively). The greatest relative increases in DALYs for males and females were observed in Greece (+89.3% and +79.0% respectively).
Joinpoint regression analysis of T1DM age-standardised rates
Incidence: Table 1
Observed trends were variable both within and across countries. For both males and females, the most rapid increases in EAPC for ASIRs occurred in Greece between 2001 and 2004 (+8.9%) and 2000-2004 (+7.2%) respectively. The most rapid reductions in EAPC for ASIR occurred in Italy for males and females between 2010 and 2015 (−8.4% and −8.7% respectively). No country observed persistently negative trends for either sex. Persistently positive trends were seen in all countries except for males in Ireland, for females in Australia, and for both males and females in Finland, Italy, Norway, Sweden, Canada, and the USA.
Prevalence: Table 1 and Figure 1
Observed trends were variable both within and across countries but generally increased in all observed countries. For both males and females, the greatest increase in EAPC for ASPRs occurred in Greece for males (+8.6% for 2001–2004) and Italy for females (+6.3% for 2005–2009). The greatest reduction in EAPC was observed in Italy for males (−8.3% for 2010–2015) and Norway for females (−8.9% for 2017–2019). Persistently positive trends were seen in all countries with identical exceptions seen in incidence.
Mortality rates: Table 1 and Figure 2
Observed trends were variable both within and across countries, but a general trend for reducing mortality was evident in all EU15+ countries. The greatest increase in EAPC for ASMR was observed in Austria for males (+6.2% for 1999–2004) and USA for females (+2.3% for 2013–2016). The greatest reduction in EAPC for ASMR was observed in Portugal for males (−6.7% for 1999–2006) and in Spain for females (−12.3% for 1998–2001). Persistently negative trends were only observed in Sweden for males, and Australia, Finland, Germany, Ireland, Luxembourg, Norway, Portugal, Spain, and Sweden for females. Persistently positive trends in ASMR EAPCs were not observed in any country for either sex.
Disability-adjusted life-years: Table 1 and Figure 3
Observed trends were variable both within and between countries. The greatest increase in EAPC for DALYs was observed in Spain for both males and females between 2017 and 2019 (+7.8% and +6.1% respectively). The greatest reduction in EAPC for DALYs was observed in Finland for males (−5% for 2012–2019) and Italy for females (−7.8% for 2010–2015). Persistently negative trends in DALYs were not observed in any country for either sex. Persistently positive trends in DALYs were observed in Australia and Greece for males, and Austria, France, and Greece for females.
Discussion
Principal findings
In this observational analysis of the trends in the disease burden from T1DM across the 19 countries of the EU15+ between 1990 and 2019, general overall increases in T1DM incidence and prevalence rates were observed in all countries and sexes (excluding for females in Finland). In a number of EU15+ countries, however, T1DM incidence and prevalence trends have shown changes in direction, with a transition to reducing ASIRs and ASPRs observed over the most recent years. Despite the overall increases in T1DM ASIRs and ASPRs, concomitant decreases in T1DM mortality rates across all countries and sexes were identified. Less uniform trends in DALYs from T1DM were observed, with some countries demonstrating improvements in DALY rates, and others demonstrating deteriorating rates. T1DM DALYs and ASMRs were greater in males than females for almost all countries and years observed.
Comparison with prior studies
Incidence & prevalence
Previous observational analyses have included data from the EURODIAB registries from 26 well defined geographic locations in 22 European countries to obtain age and sex-standardised incidence data. 4 These data reported similar increases in T1DM incidence (+3.9% in children <14 years across these centres between 1989 and 2013). They are also in keeping with additional evidence suggesting global increases in T1DM incidence over recent decades.3,10,11 Interestingly in analyses of individual centres contributing to the EURODIAB registries, a slowing rate of increases in incidence rates were observed in Finland and Norway. This is consistent with our analysis, which demonstrates reductions in ASIR and ASPR EAPCs over the most recent trends in number of EU15+ countries.
Females in Finland were the only cohort with overall reductions in ASIRs and ASPRs between 1990 and 2019 (Table 1). Previous evidence assessing T1DM incidence in Finland reported increasing incidence rates from 1980 which plateaued towards 2011.12,13 The trends in the present analysis mirror these findings and provide further evidence to show significant reductions in T1DM incidence in Finland from 2012 onwards respectively (Finland EAPC −6.3%, −3.3%, for males and females respectively (p < .05)).14,15
T1DM’s aetiology is typically autoimmune and may predispose females more than males. 16 Previous international T1DM incidence studies are not in agreement with a potential predominance of T1DM in a particular gender, and the data in the present analysis show that females had lower ASIRs than males in 17/19 countries investigated in 2019.3,10,14,15,17–21 Differences may be explained by contrasting study designs and demographics of the patient groups investigated; for example one study identified that males over the age of 9 and females below the age of 10 may have higher incidence rates than their counterparts. 10
The overall increases in both T1DM incidence and prevalence rates pose significant impacts on health services. Of note, the long term sequelae of poorly controlled T1DM coupled with the increasing demand for anti-diabetic medication and technology have notable financial implications. 22
Mortality
Despite the increases in prevalence and incidence, mortality from T1DM is improving, reflecting improvements in the management of the disease. 23 The excess mortality from T1DM is well evidenced, with possible contributing factors including associated cardiovascular, renal, and neuropathic disease.24,25 Limited data directly comparing mortality rates from T1DM across the EU exist, however single nations studies have been conducted in Finland and Sweden, with regional studies in the UK.21,26–29 These data largely mirror the trends observed in this analysis, suggesting overall decreases in T1DM mortality trends. It has been suggested that the mainstay of this reduction in mortality stems from improved quality of care, and better primary prevention of late diabetic complications such as cardiovascular disease. 30 The acute complications from untreated diabetes remain amongst the leading causes of T1DM mortality. 21 Access to diabetes services, insulin, and compliance with insulin therapy amongst children are contributors to acute complications. In the UK, the National Institute for Health and Care Excellence (NICE) recommends a number of yearly checks for children with diabetes to prevent complications, of which The National Paediatrics Diabetes Audit (NPDA) considers seven of these checks to be yearly essentials. In 2018/19, 55.2% of those aged under 24 with diabetes underwent all seven health-checks, improving from 49.8% the previous year. 31 The importance of psychosocial and socio-economic factors in relation to early mortality from T1DM has been well described. 32
Disability-adjusted life-years
A DALY represents the equivalence of losing a single year of full health, and is defined as a measure of health burden, or morbidity, of a disease with regards to mortality and disability. Over time this can be recorded to assess the changing health implications of disease diagnosis for patients within a population. Limited data exist which compare trends in DALYs over time across EU countries. Despite positive changes within diabetes healthcare policy and uniform reductions in mortality rates, our data show that T1DM DALYs have increased in the majority of EU15+ countries over the most recent trends (12/19 and 16/19 countries for males and females respectively). We also find that T1DM DALYs between countries was highly heterogenous (most recent EAPC T1DM DALYs range −7% to +7.8%). These findings may represent disparity between the effectiveness of different public health strategies.
Strengths and weaknesses
We believe this to be the first study to compare T1DM incidence, prevalence, mortality, and DALYs in EU15+ countries using data obtained from the GBD study. There are a number of important limitations to consider when using these data. Firstly, this observational study design of this project renders discussion regarding causative contributors to the trends cautious. Secondly, the GBD attributes all deaths from diabetes in individuals less than 15 years of age to type 1 diabetes, even if not specified. To adjust for other ill-defined non specified diagnoses in individuals >15 years old, the GBD uses ‘garbage’ code redistribution algorithms, which assess and redistribute deaths assigned to ill-defined diagnoses or conditions which cannot be a single cause of death. For attributing mortality to T1DM, only vital registration data were available, of a potential seven data sources for estimations of disease mortality in the GBD methodology. Third, we acknowledge the change in coding practice from ICD-9 to ICD-10 during the study period, and the GBD attempts to account for this by mapping deaths to lists of causes of deaths. The authors acknowledge that due to the method of data extraction we are unable to account for the number of individuals who have been mislabelled as T1DM patients, though this is likely to be negligible and without bearing significant impact the data. Finally, there are inevitably confounders that are not accounted for; we extracted sex-specific, age-standardised data to limit additional confounders which would affect the reliability of the data for comparison.
Conclusions
Whilst incidence and prevalence of T1DM have generally increased in EU15+ countries over the last three decades, mortality has decreased. Some EU15+ countries have, however, noted improving incidence and prevalence from T1DM over the most recent trends. Trends in DALYs were more variable across included countries and should be a focus of future investigation. This study highlights the significant positive impact that health services in EU15+ countries have had on the morbidity and mortality of patients with T1DM over the last 30-years. This study underscores the importance of these initiatives as the prevalence and incidence of T1DM continues to rise.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.