
Abstract
Background
The purpose of this study is to assess metabolic indicators and trends in microvascular complications among Chinese adults with newly diagnosed type 2 diabetes during 2000–2020.
Methods
3,907 patients were included and divided into three groups according to a time period of 7 years. This study analyzed trends in proportions of patients reached therapeutic targets of blood glucose, pressure and lipids, and trends in albuminuria, retinopathy, and peripheral neuropathy.
Results
In the past 20 years, the age of adults with newly diagnosed type 2 diabetes tended to be younger, and the proportion of female patients increased. There seemed no improvements in blood glucose and pressure. The rate of awareness and treatment on target of hypertension was less than 50%. There was a significant decrease in the prevalence of retinopathy, but no changes in nephropathy or peripheral neuropathy. Complications were more common for patients who were smoker, male, or with hypertension and obesity.
Conclusions
Over the past two decades, there have been encouraging reductions in retinopathy in Chinese adults with newly diagnosed diabetes, but no significant change in albuminuria and peripheral neuropathy. It may be related to the low awareness of diabetes and insufficient controlled blood glucose, pressure and lipids on target.
Introduction
Type 2 diabetes mellitus (T2DM) is a growing public health issue in the world, affecting over 400 million people, and it is considered that diabetes could affect nearly 700 million people by 2045. 1 The prevalence of T2DM among people aged over 18 years in China is 11.2%. 2 The prevalence of diabetes among Chinese living in developed countries and regions is significantly higher than that of Caucasians. 3 Persistently hyperglycemia causes generalized vascular damage, which would affect heart, vascular, retina, kidneys and nerves, and finally resulting in various complications. 4 The prevalence of micro-albuminuria was 17.3–54.9%.5–7
Nowadays, at least in western countries, T2DM is probably diagnosed at an earlier stage and this might have reduced the prevalence of complications. 8 However, the information on the prevalence of chronic complications in newly diagnosed T2DM is still scant. Most studies, in fact, did not focused on microvascular complications, especially for the Chinese patients with newly diagnosed T2DM.
The aim of the present study was to assess the trend in risk factors and microvascular complications among Chinese adults with newly diagnosed diabetes in our hospital from 2000 to 2020.
Subjects, materials and methods
Study population
This is a retrospective, single-centre observational study. Ethical approval was obtained from the local ethics committee of our centre, and the study was conducted under the Declaration of Helsinki. All subjects were newly diagnosed T2DM patients who participated in screening for diabetes complications at our Diabetes Center between January 2000 and November 2020. A total of 3,907 cases were collected (Figure 1), including 2,233 males and 1,674 females, and divided into three groups according to a time period of 7 years. Flow diagram of cases screening.
Inclusion and exclusion criteria
Inclusion criteria: 1. Age ≥18; 2. Newly diagnosed T2DM with a duration of less than 6 months. Exclusion criteria: 1. Type 1 Diabetes; 2. Gestational diabetes mellitus (diabetes mellitus with pregnancy or gestational diabetes mellitus); 3. Other special types of diabetes; 4. Those who reported any microvascular disease before the diabetes diagnosis.
Treatment and risk factor controlling
The authors defined receiving diabetes treatment as the self-reported use of oral antidiabetic drugs or insulin currently. Blood pressure was measured up to four times with electronic sphygmomanometer, and the mean of all available readings was analyzed. Hypertension was defined as having elevated mean blood pressure (mean systolic/diastolic blood pressure≥140/90 mmHg) or the self-reported current use of antihypertensive medication. Receiving treatment was defined as the current use of antihypertensive medication, and blood pressure control as having a mean blood pressure<130/80 mmHg. Serum total cholesterol was measured by oxidase method, and measurements from fasting participants. Hyperlipidemia was defined as having elevated lipids (total cholesterol ≥ 5.17 mmol/L) or the self-reported current use of lipid-lowering medication. 9 Receiving treatment was defined as the self-reported current use of lipid-lowering medication and lipid control as total cholesterol <5.17 mmol/L.
Microvascular complications
The estimated glomerular filtration rate (eGFR) was calculated by using the Chronic Kidney Disease Epidemiology Collaboration formula. 10 Reduced eGFR was referred to as having an eGFR<60 mL/min/1.73 m2. Urine albumin and creatinine concentrations were measured in a random urine sample by fluorescent immunoassay. Albuminuria was defined as an albumin-to-creatinine ratio ≥30 mg/g. All participants had color fundus photographs or direct ophthalmoscope taken of both eyes retinopathy was assessed by graders using the Early Treatment Diabetic Retinopathy Study (ETDRS) protocol. 11 Retinopathy (DR) was defined as having microaneurysm, hemorrhage spot, neovascularization, vitreous hemorrhage, cotton-wool spot and macular lesions 12 combined with the diagnosis of an ophthalmologist. Clinical diagnostic criteria of peripheral neuropathy (DPN): those with clinical symptoms of neuropathy, 5 items check (ankle reflex, acupuncture pain, vibration, pressure, temperature) 1 out of 5 abnormalities; for those without clinical symptoms, 2 out of 5 examinations were abnormal.
Sociodemographic measures and body mass index calculation
Participants self-reported their age, gender, and smoking status (current, former or never). Body mass index (BMI) was calculated by measured weight in kilograms divided by height in meters squared. According to the WHO Asian population weight classification standard, participants were classified into three weight status groups (18≤ BMI <23 kg/m2 as normal; 23≤ BMI <27.5 kg/m2 as overweight; BMI ≥27.5 kg/m2 as obesity). Waist circumference (to the nearest 0.5 cm) was measured with a plastic tape meter at the level of the umbilicus. Central obesity: Waist circumference: male ≥90 cm, female ≥85 cm.
Statistical analyses
The authors calculated participant characteristics, the prevalence, treatment, control of risk factors, and the prevalence of microvascular and cardiovascular diseases. Survey years were pooled into three time-intervals (2000–2006, 2007–2013, and 2014–2020). Trends were assessed by using logistic (binary outcomes), linear (mean of continuous outcomes), or quantile (median of continuous outcomes) regression models. The midpoint of each survey period was modeled as a continuous, linear predictor in the regression models. The authors examined the distribution of risk factors and compared changes overtime using χ2 tests. For complications that changed significantly over time, adjusting for age and sex, we used multivariable logistic regression models to explore how changes in diabetes risk factors, and weight status might explain the observed trends. All analyses were conducted using SPSS version 23.0. A two-sided p value of 0.05 was considered statistically significant.
Results
Characteristics of Chinese adults aged ≥18 years’ with newly diagnosed diabetes.

Data are presented as percentages or means (with SD). Normal weight was defined as 18≤ BMI <23 kg/m2, overweight was defined as BMI ≥23 and<27.5 kg/m2, and obesity was defined as BMI ≥27.5 kg/m2.
Trends in the prevalence, treatment, and control of risk factors in Chinese adults with newly diagnosed diabetes during 2000–2020.

Abbreviations: IQR, interquartile range. Data are presented as percentages or median (with interquartile range). All three risk factors controlled was defined as A1C <7.0% plus blood pressure<130/80 mmHg, total cholesterol<174.0 mg/dL (4.5 mmol/L) %.

Trend in proportions of patients reached therapeutic targets of A1C <7.0%, BP <130/80 mmHg, and total cholesterol<5.17 mmol/L. (a) Proportions of patients reached therapeutic targets of A1C <7.0%, BP <130/80 mmHg and total cholesterol<5.17 mmol/L. (b) Proportions of patients reached three combined therapeutic targets.
There was no significant change in the prevalence of hypertension among adults with newly diagnosed T2DM (from 47.7 to 47.6%, p = 0.445, Table 2). An increasing trend in the proportion of adults with hypertension treated and controlled to less than 130/80 mmHg (41.9–49.7%, p = 0.258).
The use of lipid lowering medication was unchanged (Table 2), and the prevalence of hyperlipidemia was stable. However, the trend in the proportion with cholesterol control were increased from 32.2 to 41.1 (p = 0.179, Table 2, Figure 2).
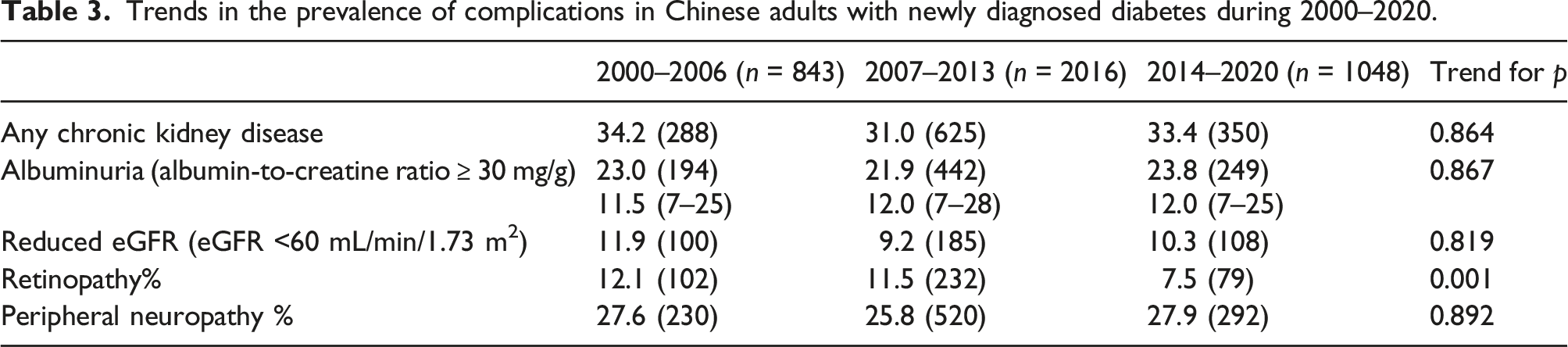
Trends in the prevalence of complications in Chinese adults with newly diagnosed diabetes during 2000–2020.

The prevalence of microvascular complications among Chinese adult patients with newly diagnosed diabetes during 2000–2020.
Adjusted odds ratios (95% CIs) for the associated risk factors with microvascular complications in Chinese adults with newly diagnosed diabetes.

Ref, Odds ratios were adjusted for age.
Discussion
This study found something interesting. Firstly, from 2000 to 2020, there was no improvement in the control of risk factors (such as A1C, blood pressure, or cholesterol), and substantial decline in the prevalence of retinopathy in those patients with newly diagnosed T2DM. Secondly, the burden of complications remained high. Approximately 23% patients had albuminuria, 11% had retinopathy, and 27% had peripheral neuropathy. Thirdly, the prevalence of obesity, peripheral neuropathy and albuminuria was unchanged, even if retinopathy declined.
Although aging is an independent risk factor for diabetes, studies indicated that the onset age of diabetes is getting younger globally,13,14 and the proportion of young and middle-aged patients is increasing. Large-scale epidemiological studies in China showed that the prevalence of diabetes among young and middle-aged people was increasing from 2007 to 2017.2,15 The percentage of young and middle-aged patients in this study is more than 80%, and the proportion of young patients shows an increasing trend, and the average age is also gradually younger. Similar to our study, the study by Zijing Wang et al. 16 found that from 2008 to 2017 in Beijing, diabetes was diagnosed at younger ages, as the average age at diabetes diagnosis dropped from 62 to 56 years. Considering the poor long-term prognosis of individuals with early-onset diabetes, it is of great importance for young patients to achieve optimal control of risk factors.
The results demonstrated that the proportion of patients with newly diagnosed diabetes or with obesity declined from 2014 to 2020, which was associated with enhanced awareness on related adverse event, but still less than one-third of patients with normal weight. It is well-known that hyperglycemia, hypertension, and dyslipidemia are risk factors for microvascular and macrovascular diseases in T2DM. In this study, there was no significant change in the control rate of blood glucose, blood pressure and blood lipid in the past 20 years, which was related to poor weight control, low awareness rate, lower control on target for blood glucose, blood pressure and lipid disorders, as well as lower education and management level for the patients with diabetes.
It was generally believed that microvascular complications were closely related to the level of blood glucose and the duration of diabetes. Our research showed that in newly diagnosed T2DM patients, the prevalence of microvascular complications remained high in the past 20 years, which suggested that the diagnosis of T2DM was delayed among a large proportion of T2DM patients. Due to the hidden onset of T2DM, it was difficult to determine the exact time of onset of disease, that may be the reason why there existed certain proportion of microvascular lesions in patients with newly diagnosed T2DM.
The prevalence of retinopathy varied in different studies, with 36% of newly diagnosed T2DM patients with DR in the UKPDS, compared with 13% in DD2.17,18 Several studies have shown that diagnosis at an older age was one of the risk factors for DR,19,20 which may explain why the prevalence of DR varies from study to study. This study showed that there was a remarkable association between retinopathy with male gender, which was consistent with the results of Liu et al. and other studies,20–22 but different from those of Talu S et al. 23 In this study, the prevalence of DR in patients with newly diagnosed T2DM decreased from 12.1% to 7.5% in the past 20 years, which may be related to the higher awareness of retinopathy and the earlier diagnosis of diabetes. The appearance and use of drugs with additional microvascular benefits might also contribute to the lower prevalence of retinopathy. Another possible explanation is the increasing percentage of patients achieving optimal blood glucose, blood pressure and lipids control in our study, as studies have demonstrated that hyperglycemia and hypertension were identified as critical risk factors of early retinopathy in T2DM 24
Lots of literature showed linear relation between the degree of microalbuminuria and BMI, blood pressure, while gender correlation of microalbuminuria was not been reported in T2DM.11,12 These findings differ from our data that there is no association of microalbuminuria with BMI. Our data demonstrated that there was no effect of BMI on the prevalence of microalbuminuria, probably because only 23%–30% of our patients were severe obesity. In this study, the prevalence of renal lesions did not decrease significantly in recent years, which should be attributed to the low awareness, treatment and control on target of blood pressure in these patients.
Among adults newly diagnosed T2DM, there was no change in the clinical manifestations of kidney disease over the last 20 years, unchanged in the prevalence of reduced eGFR. One study reported an increase in the prevalence of reduced eGFR but no significant change in the prevalence of albuminuria among US adults with diabetes from 1988 to 2008. 25 It may be related to unchanged blood pressure compliance status in these patients.
Nerve disorders already be present at the time of diabetes diagnosis. Based on some small study samples, neuropathy was already present in 2–10%.26,27 In recognition of the importance of early detection and treatment of neuropathy, several guidelines state that patients with T2DM should be screened for nerve disorders at the time of their diabetes diagnosis and yearly thereafter. 28 The present study showed that the prevalence of diagnosed neuropathy is much higher (25.8–27.9%), indicating that doctors need to pay more attention to the screening of peripheral neuropathy in newly diagnosed T2DM patients. Kostev et al. 29 have reported that DPN was associated with male gender and age. This study showed that male and smoker were significantly associated with DPN. This finding could be attributed to the damage exerted by smoking on vasa nervorum as well as its direct detrimental effects on nerve structure and function. The latter includes an increased oxidative stress, with reactive oxygen species and advanced glycosilation end-products as mediators, leading to mitochondrial dysfunction, inflammation, DNA damage and apoptosis. 30
Unhealthy lifestyle, including sedentary behavior and a high energy/high fat diet, is associated with the onset and progression of T2DM. Lifestyle change are generally considered to be the cornerstone of the treatment of T2DM. Encouragingly, our research showed that in recent years, more T2DM patients focused on lifestyle intervention without taking hypoglycemic agents, implying the higher awareness of the importance of a healthy lifestyle for T2DM control.
This study demonstrated that adults who were smokers, hypertension, male or obesity had the highest prevalence of complications at the time of diagnosis. Compared with men, the risk of complications in women was lower, which may be related to the protection of estrogen during menopause. The identification of high-risk groups can be made through household health records, basic public health services and random screening, such as during health check-ups or during the diagnosis and treatment of other diseases. Diabetes screening was helpful to the early detection of diabetes and improve the prevention and treatment of diabetes and its complications. Therefore, diabetes screening should be performed in all high-risk population.
Hypertension and dyslipidemia are two common comorbidities of diabetes. The integration treatment of diabetes, hypertension and dyslipidemia is critical for reducing the risk of complications. The 3B STUDY in China found that 72% T2DM patients reported comorbid hypertension, dyslipidemia, or both, and only 5.6% of T2DM patients reached all 3B targets. 31 Our study also showed that in newly diagnosed T2DM patients, the proportion of those who achieved all three risks controlled was less than 8%, though the proportion increased from 4.5% to 7.6% in the past 20 years. Furthermore, our data showed that the treatment of hypertension and hyperlipidemia failed in up to 80% and 75% of adults with newly diagnosed diabetes, respectively. It may be related to the low awareness rate of hyperlipidemia and hypertension in newly diagnosed T2DM patients, highlighting the need to increase of the awareness of risk factors and more aggressive and timely treatment of all risk factors immediately after diagnosis of T2DM.
Notably, there was an increasing tendency in the awareness of hypertension, which increased from 62.9% to 69.9% in the past 20 years. Despite the improvement in awareness, the percentage of treated hypertension remained low, approximately 20%, which was consisitent with 22.9% in China Patient-Centered Evaluative Assessment of Cardiac Events (PEACE) Million Persons Project. 32 And the percentage of treated hyperlipidemia remained to be approximately 20% in this study. Therefore, more effective and affordable treatment for hypertension and hyperlipidemia is needed.
Our study exists several limitations. Firstly, there may be misclassification of incident diabetes cases, because our definition relies on age of diagnosis and islet cell function. 33 However, prior research indicates that these measures were highly credible. Secondly, this is a single center sample and cannot reflect the overall epidemiological situation of the Chinese population.
Conclusions
Chinese adults with newly diagnosed T2DM have higher proportion of comorbid hypertension and hyperlipidemia. The control of risk factors for microvascular diseases in newly diagnosed T2DM should be improved. Control of glycemia, blood pressure, and total cholesterol is far from expectation despite the guidelines for the management of diabetes and cardiovascular diseases have been carried out. It is necessary to strengthen the screening of high-risk population, comprehensive management of various metabolic and cardiovascular risk factors for early diagnosis and treatment of diabetes and its complications.
Footnotes
Acknowledgements
We would like to thank the all colleagues in the Endocrinology Department, PLA Strategic Support Force Medical Center (The 306th Hospital of PLA).
Author contributions
Zhangrong Xu and Aihong Wang conceived and designed study. Lintao Shi, Jing Xue, Weibo Zhao, Yuxia Cheng, Xiang Li, Jianjun Wang, Zhangrong Xu and Aihong Wang acquired and analyzed the data. Lintao Shi, Jing Xue, Weibo Zhao, Yuxia Cheng and Aihong Wang interpreted data. Lintao Shi, Jing Xue, Weibo Zhao and Aihong Wang drafted manuscript. Lintao Shi, Jing Xue, Weibo Zhao, Yuxia Cheng, Xiang Li, Jianjun Wang, Zhangrong Xu and Aihong Wang revised manuscript critically and approved the submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by discipline construction promotion project of PLA Strategic Support Force Medical Center (21XK0106).