
Abstract
Background
The indication for treatment of type 1 diabetes(T1D) with the sodium–glucose cotransporter 2 inhibitor (SGLT2i) dapagliflozin has been withdrawn in Europe likely because of concern for diabetic ketoacidosis (DKA). We calculated the incidence of DKA in people with T1D treated with SGLT2i in Denmark.
Methods
Clinical data from adults with T1D in Denmark were collected from nine outpatient clinics. Electronic health records made the search for DKA accurate.
Results
From a population of 10.500 we observed 134 people treated with SGLT2i over a total period of 222 patient-years. Of those 72% were female, mean age (SD) was 51.4 (13.6) years and median duration of treatment (median, IQR) with an SGLT2i were 12.0 (6.0–29.0) months. The incidence of DKA was zero%.
Conclusion
In 134 people with T1D treated with SGLT2i we found that none of the participants developed DKA during the treatment.
Estimating the incidence of DKA in type 1 diabetes during SGLT2i treatment. No events of DKA over an observation time of 222 patient years. SGLT2i may be safe in people with type 1 diabetes.Key messages
The sodium–glucose cotransporter 2 inhibitor (SGLT2i) dapagliflozin, was approved in Europe as adjunctive therapy for type 1 diabetes (T1D) in 2019. Recently AstraZeneca withdrew dapagliflozin for this indication due to concern for diabetic ketoacidosis (DKA). We have collected data from 134 people with T1D treated with SGLT2i and calculated the incidence of DKA.
This is a retrospective observational study, based on reports from nine participating centers in Denmark. Data were collected in the form of anonymized mean values of age, sex, treatment duration and incidence of DKA. We searched electronic health records for the diagnosis of DKA in an outpatient setting and during hospitalization. The system can discriminate between different types of diabetes allowing us to focus on T1D. As this is a quality assurance project with gathering of minimal data, consent from subjects or approval from institutional review boards were not required.
Characteristics of the study population.
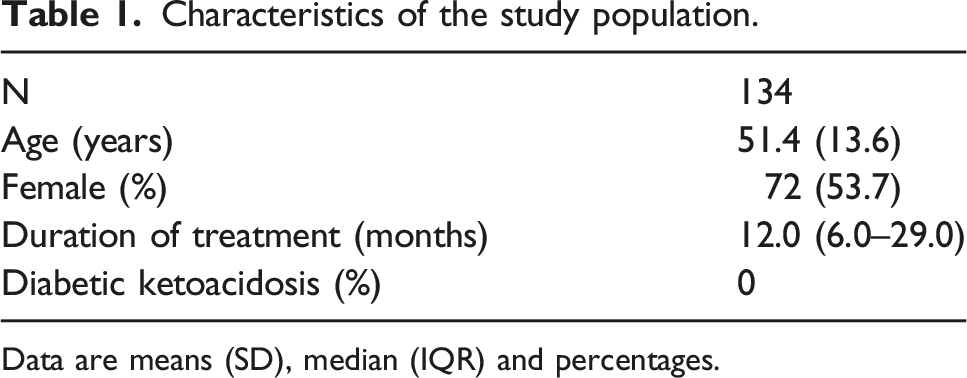
Data are means (SD), median (IQR) and percentages.
In the randomized controlled trials with dapagliflozin 5 mg once daily 4.0% of the participants with T1D developed DKA, compared to 1.1% in the placebo group over a period of 24–52 weeks. 1 This increased risk has been a limiting factor for more widespread use of SGLT2i in T1D.
Palanca et al. evaluated real-world safety of SGLT2i use in people with T1D in 199 adults and found DKA incidence to be 3.5%. 2 However, in the subgroup analysis of participants in whom the EU label was followed (dapagliflozin 5 mg once daily and BMI ≥ 27 kg/m2) there were no DKA events.
Several studies have shown that the SGLT2i have beneficial cardiovascular and kidney protective effects in people with and without type 2 diabetes (T2D). 3 There are no studies of heart and kidney outcomes in participants with T1D and there is currently no prospect that such studies will be made, although both sotagliflozin and empagliflozin have been demonstrated to reduce albuminuria in persons with T1D.4,5 If the cardiorenal effects seen in T2D and in populations without diabetes could be proven in T1D, these effects may outweigh the risk of DKA. As people with T1D have higher mortality compared with the general population, with cardiovascular disease (CVD) being the main cause of death, improved treatment of diabetic kidney disease and CVD is needed. It is therefore important to consider whether the risk of DKA with SGLT2i treatment observed in clinical trials of T1D can be offset by the large risk reductions seen in cardiovascular and kidney outcome studies in T2D populations.
This study is limited by its observational and retrospective character. We have no data about how individuals were selected, which was likely based on the judgement of the treating physician. Due to limited access to detailed clinical data, we cannot provide a thorough analysis of the characteristics of the population, such as BMI, insulin pump use, diabetes duration, glucose control and frequency of side effects. Being a real-world study with a population of 134 individuals interpretation needs to be done with care especially in respect to a relatively uncommon event such as DKA.
Persons with T1D in Denmark offered treatment with SGLT2i are carefully selected by the attending physician, receive training regarding the risks of this treatment and must demonstrate an understanding of how this is handled before treatment is initiated. This indicates that SGLT2i treatment may be safe in people with T1D if patients are carefully selected and instructed.
Footnotes
Acknowledgments
EBS, YH, ES, GHD, TMJA and MR have no relevant conflict of interest to disclose. V.S.S. has no conflicts of interest specific to this manuscript. V.S.S. is supported by the Department of Medicine Eliot Phillipson Clinician Scientist Training Program, a Banting and Best Diabetes Centre Postdoctoral fellowship at the University of Toronto, and a CIHR Frederick Banting and Charles Best Canada Graduate Scholarships Doctoral Research Award. V.S.S. has received travel support from Merck Canada. PLK has received lecture fee from Sanofi A/S, Novo Nordisk A/S and AstraZeneca A/S. UK har served as advisory board panels and/or received travel grants or speakers fee from Novo Nordisk, Abbott Medical Denmark, Eli Lilly, Boehringer Ingelheim, Mundipharma, Sanofi and Astra Zeneca. HUA owns stocks in Novo Nordisk. HUA has served on advisory boards for Novo Nordisk, Abbott and Astra Zeneca and has received lecture fees from Nordic Infucare. PHG has served on advisory boards for Astra Zeneca and Boehringer Ingelheim. He has received personal fees from Novo Nordisk. KKF owns stocks in Novo Nordisk and has received lecture fees from AstraZeneca and travel grants from Novo Nordisk. KWH has received honorarium as an advisory board member for Abbot Laboratories A/S Denmark. HHT has received fees from Boehringer Ingelheim Danmark A/S as an educator. D.Z.I.C. is supported by a Department of Medicine, University of Toronto Merit Award and receives support from the CIHR, the Heart and Stroke Richard Lewar Centre of Excellence, the Heart and Stroke Foundation and the Kidney Foundation of Canada, and trainee support from the Department of Medicine Eliot Phillipson Clinician Scientist Training Program, the Banting and Best Diabetes Centre Postdoctoral fellowship at the University of Toronto, and the CIHR Frederick Banting and Charles Best Canada Graduate Scholarships Doctoral Research Award. Dr. Cherney is also supported by a CIHR-Kidney Foundation of Canada Team Grant (2022-2026). PR reports personal fees from Bayer during the conduct of the study. He has received research support and personal fees from AstraZeneca and Novo Nordisk, and personal fees from Astellas Pharma, Boehringer Ingelheim, Eli Lilly, Gilead Sciences, Mundipharma, Sanofi, and Vifor Pharma. FP has served as a consultant, on advisory boards or as educator for AstraZeneca, Novo Nordisk, Boehringer Ingelheim, Sanofi, Mundipharma, MSD, Novartis, Amgen and has received research grants to institution from Novo Nordisk, Boehringer Ingelheim, Amgen and AstraZeneca.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author contributions
FP and ES initiated this study. EBS analyzed the data and drafted the first version of the manuscript, with subsequent discussion and input from all authors, who had access to all data. FP is the guarantor of this work and all authors approved the final version of the manuscript.