
Abstract
Background:
Using normal home blood pressure (home BP) as a reference, isolated high home systolic blood pressure (IH-home SBP) increases the risk of diabetic nephropathy. However, whether diabetic nephropathy would improve among diabetic patients without IH-home SBP has not been previously assessed.
Methods:
This prospective 5-year cohort study of 264 patients with moderate or severe albuminuria investigated the effect of IH-home SBP or normal home BP on the risk of diabetic nephropathy in patients with type 2 diabetes mellitus. Improvement of diabetic nephropathy was defined as remission or regression from moderate or severe albuminuria to normal or mildly increased albuminuria.
Results:
Improvement of diabetic nephropathy was shown in 59 out of 264 patients during 5 years. The adjusted odds ratio (95% confidence interval) of normal home BP for improving diabetic nephropathy was 2.52 (1.01–5.99, p = 0.05).
Conclusion:
Normal home BP had relation to an improvement in diabetic nephropathy among type 2 diabetic patients with moderate and severe increased albuminuria in the observation period of 5 years. Good home BP control might be valuable to ameliorate diabetic nephropathy.
Introduction
Controlling home blood pressure (home BP) is of paramount importance in preventing diabetic nephropathy 1 because high home BP is associated with the progression of diabetic nephropathy.2, 3
When systolic blood pressure (SBP) is hypertensive while diastolic blood pressure (DBP) is normotensive, isolated systolic hypertension (ISH) is diagnosed. 4 ISH is a frequent form of hypertension, which increases the risk of premature cardiovascular deaths5–7 ISH, assessed by home BP (home ISH), has also been shown to associate with the risk for the development of diabetic nephropathy. Isolated high home systolic blood pressure (IH-home SBP) is a valuable predictor of diabetic nephropathy progression, based on results from our previous cohort study.8,9
In contrast, rigorous control of SBP is associated with remission or regression of diabetic nephropathy.10– 13 The optimal home SBP for remission induction or regression of microalbuminuria might be below 130 mmHg. 14 Using an angiotensin II receptor blocker (ARB) reduced microalbuminuria in Japanese with patients type 2 diabetes mellitus (DM) regardless of with or without hypertension. 15
Nevertheless, whether diabetic nephropathy would improve in diabetic patients without IH-home SBP has not been previously assessed. Then, we changed the viewpoints and performed a further assessment aiming to provide the impact of preventing ISH on the improvement of diabetic nephropathy in the patient group with type 2 DM through the observation period of 5 years.
Methods
The resources investigated in this study was the same as in our previous research based on data from KAMOGAWA-HBP study, which was the home BP cohort of patients type 2 diabetic patients who regularly went to the clinic at the Kyoto Prefectural University of Medicine Hospital or some other general hospitals existed in Japan as an outpatient. 1 The patients regular care physicians are the principal investigator of the study.
The current research involved patients with type 2 DM and assessed a prognostic significance of home BP for progression of diabetic nephropathy. Nephropathy was classified as follows: normal or mild albuminuria, described as urinary albumin/creatinine ratio (UACR) less than 30 mg per gram of creatinine (mg/g Cr); moderately increased albuminuria (microalbuminuria), described as UACR 30–300 mg/g Cr, or severely increased albuminuria (macroalbuminuria), described as UACR more than 300 mg/g Cr.16–21 Improvement of diabetic nephropathy was described as remission or regression from moderate or severe albuminuria to normal or mildly increased albuminuria within the confines of the observation period. The local research ethics committee had recognition of the research methods (RBMR-E-349). Adherence to the general rules of the Declaration of Helsinki was kept by the research, and all patients who participated in the research prior to enrollment provided informed consent.
Data collection
Morning fasting blood samples were collected for biochemical measurements. Serum lipid profile (including levels of low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, and triglycerides), hemoglobin A1C (HbA1c), creatinine and some other biochemical markers were evaluated by common laboratory process. The data collection of urinary samples was performed simultaneously with the beginning of the home BP measurements. Urinary albumin and creatinine concentrations were measured in second morning urine samples. An immunoturbidimetric assay was used to measure UACR, and the mean value of three consecutive urinary measurements was evaluated, which corresponded to the UACR. As recommended by the Japan Diabetes Society, levels of HbA1c were categorized and reported according to the National Glycohemoglobin Standardization Program guidelines. 22 We collected analysis of the data about patient demographics and clinical characteristics, including sex, age, duration of DM, smoking status, alcohol consumption, and use of antihypertensive medication at the same time as home BP measurements began. We used the volume plethysmographic method in order to measure the brachial-ankle pulse wave velocity (baPWV), which was made use of our previous cohort study also. 23 We made a diagnosis for diabetic nephropathy on the basis of the Nephropathy Study Group criteria. 24 Alcohol drinking behavior (everyday, social, or never) and smoking behavior (current, past, or never) were evaluated through interviews for patients. We made a diagnosis for Type 2 DM when the fasting plasma glucose level was more than 126 mg/dl (7.0 mmol/L) or random plasma glucose level more than or equal to 200 mg/dl (11.1 mmol/L) on the basis of the American Diabetes Association criteria. 25
Home BP measurements
In this study, a single baseline BP measurement was performed at entry for this study. Participants were provided instructions on how to measure their SBP/DBP at home three times each morning and evening for 14 consecutive days. And then, the 14-day average of the three morning and three evening mean values were calculated. Participants were provided instructions on measuring method of their morning SBP/DBP within 1h of waking up, before breakfast or, taking drugs, and sat and rested for at least 5 minutes. 26 We applied to similarly instructions for evening SBP/DBP measurements before sleeping. In addition, eating was prohibited for over 1 hour before the evening measurement. Furthermore, we instructed patients that the cuff of the measuring device should be put around the contralateral side of the dominant arm, with its position maintained at heart level. home BP measurements were performed using an automated device, HEM-70801C (Omron Healthcare Co. Ltd, Kyoto, Japan), which utilizes a digital display to present values of SBP/DBP and heart rate, measured using the cuff-oscillometric method. HEM-70801C utilizes the same components and BP-determining algorithm as those of another device, HEM-705IT, which was previously approved the criteria of the British Hypertension Society protocol. 27
In accordance with the Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019), 28 the target level of home BP control is under 125/75 mmHg in hypertensive patients with type2 DM. Participants were categorized into four groups based on home BP levels: normal home BP (morning SBP less than 125 mmHg and morning DBP less than 75 mmHg), IH-home SBP (morning SBP more than or equal to 125 mmHg and morning DBP less than 75 mmHg, isolated high home DBP (IH-home DBP) (morning SBP less than 125 mmHg and morning DBP more than or equal to 75 mmHg), and high home BP (morning SBP more than or equal to 125 mmHg and morning DBP more than or equal to 75 mmHg). 29
Statistical analysis
The characteristics of patients who participated in our study were reported as medians with interquartile ranges or numbers. Logistic regression analysis was used to assess the relationship between IH-home SBP, IH-home DBP, and high home BP, and the risk of diabetic nephropathy, with “normal home BP” set as a reference. The following factors were considered as covariates among the adjusted models: sex, body mass index (BMI), duration of diabetes, HbA1c levels, total cholesterol, creatinine, smoking status, Clinical SBP and use of antihypertensive drugs (Model 2). In addition, adjustments were carried out the use of renin-angiotensin-aldosterone system inhibitors instead of other antihypertensive drugs (Model 3).
Moreover, we performed subgroup analyses according to age (more than or equal to 65 years vs. less than 65 years) and the use of antihypertensive medications (with vs. without antihypertensive drugs). Statistical significance was set at p < 0.05. Statistical analyses had been performed using JMP version 13.2 software (SAS Institute Inc., Cary, NC, USA). Two-tailed t test were used to determine statistical significance.
Results
Patients with type 2 DM were recruited 1,372 in the study. They were aged 20–90 years. Excluded patients were 115 and 422 because of insufficient home BP and data of UACR, respectively. Additionally, 148 patients were excluded as they freshly prescribed angiotensin-converting-enzyme inhibitor (ACE-I) or ARB or stopped them during follow-up. And then, 423 patients were excluded, who were with normal and mildly increased albuminuria.
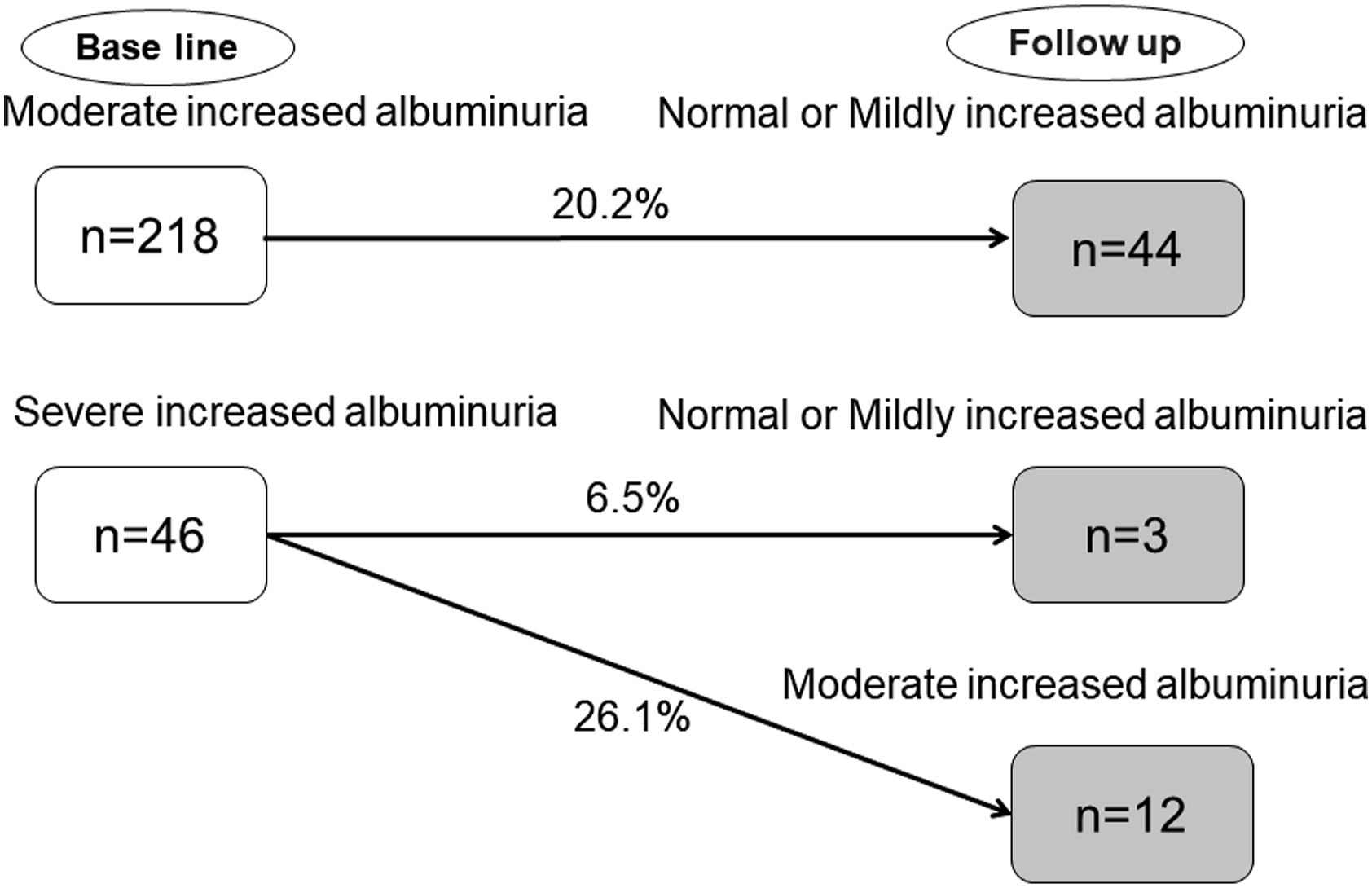
Finally, 264 patients with moderate or severe albuminuria included (Figure 1). During the observation period of 5 years, among 218 participants with moderately increased albuminuria, 44 patients showed improvement to normal or mildly increased albuminuria. Among 46 patients with severely increased albuminuria, 12 patients improved to moderately increased albuminuria, and 3 patients improved to normal or mildly increased albuminuria (Figure 2). Flow diagram for the KAMOGAWA-HBP cohort. Transition of diabetic nephropathy remission or regression.
The mean of SBP among 218 participants with moderate increased albuminuria was 138.4mmHg, and the mean of SBP among 44 participants with severe increased albuminuria was 148.3mmHg.
Improvement of diabetic nephropathy was observed in 15 patients (34.1%) among normal home BP group, in 16 patients (17.6%) among IH-home SBP group, and 28 patients (22.4%) among high home BP group, respectively. In IH-home DBP group, there were no improvement of diabetic nephropathy.
Characteristics of patients.
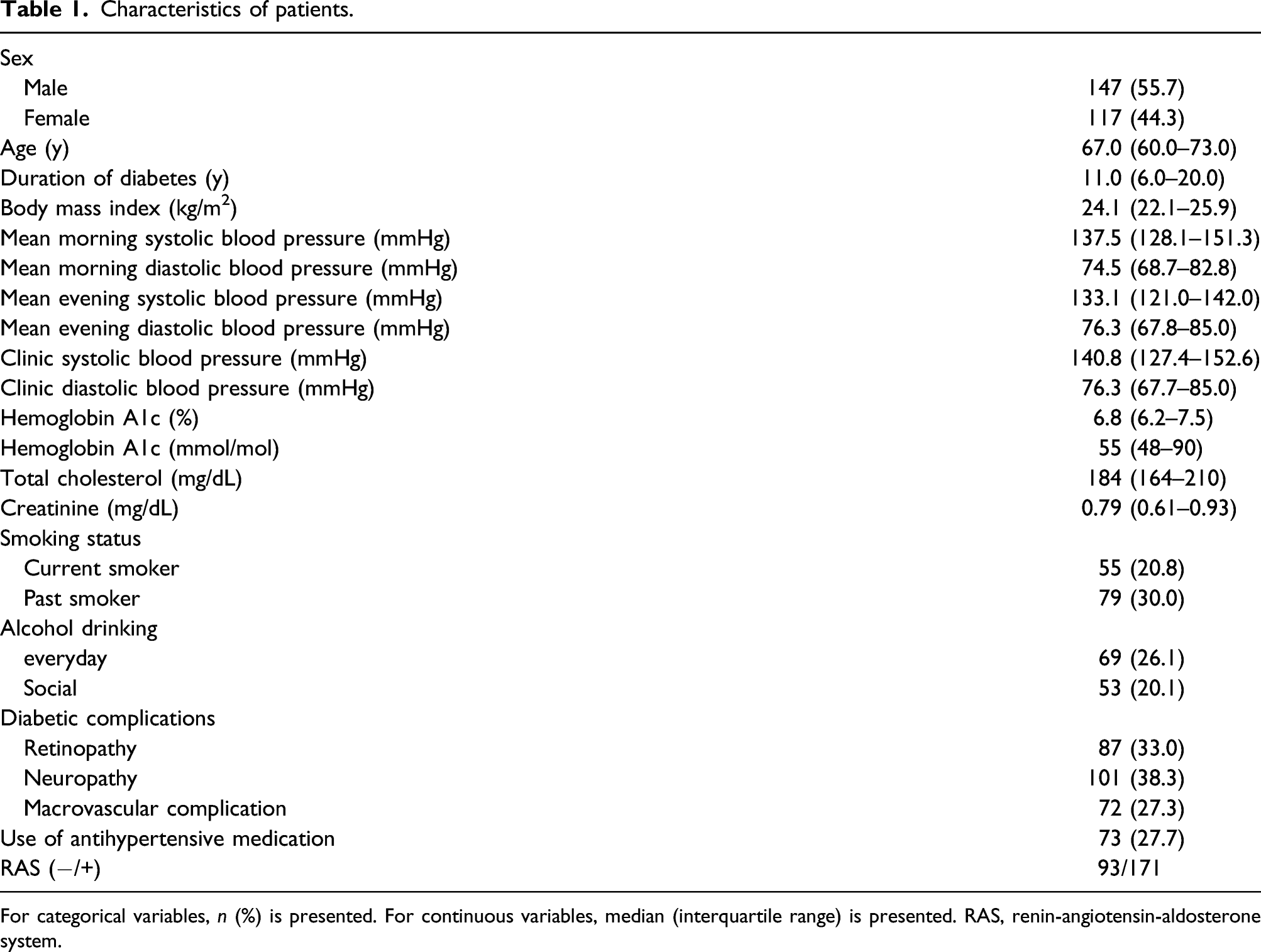
For categorical variables, n (%) is presented. For continuous variables, median (interquartile range) is presented. RAS, renin-angiotensin-aldosterone system.
Unadjusted and adjusted odds ratios for the remission or regression of diabetic nephropathy.
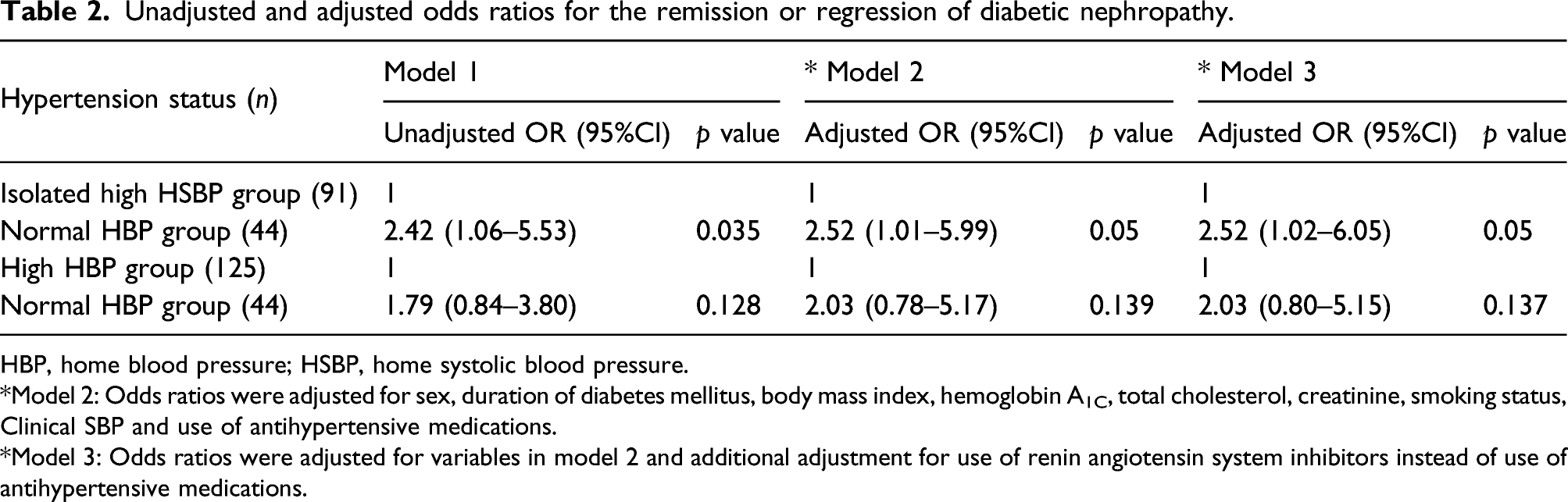
HBP, home blood pressure; HSBP, home systolic blood pressure.
*Model 2: Odds ratios were adjusted for sex, duration of diabetes mellitus, body mass index, hemoglobin A1C, total cholesterol, creatinine, smoking status, Clinical SBP and use of antihypertensive medications.
*Model 3: Odds ratios were adjusted for variables in model 2 and additional adjustment for use of renin angiotensin system inhibitors instead of use of antihypertensive medications.
Unadjusted and adjusted odds ratios for the remission or regression of diabetic nephropathy in patients equal to or more than 65 years old and less than 65 years old.
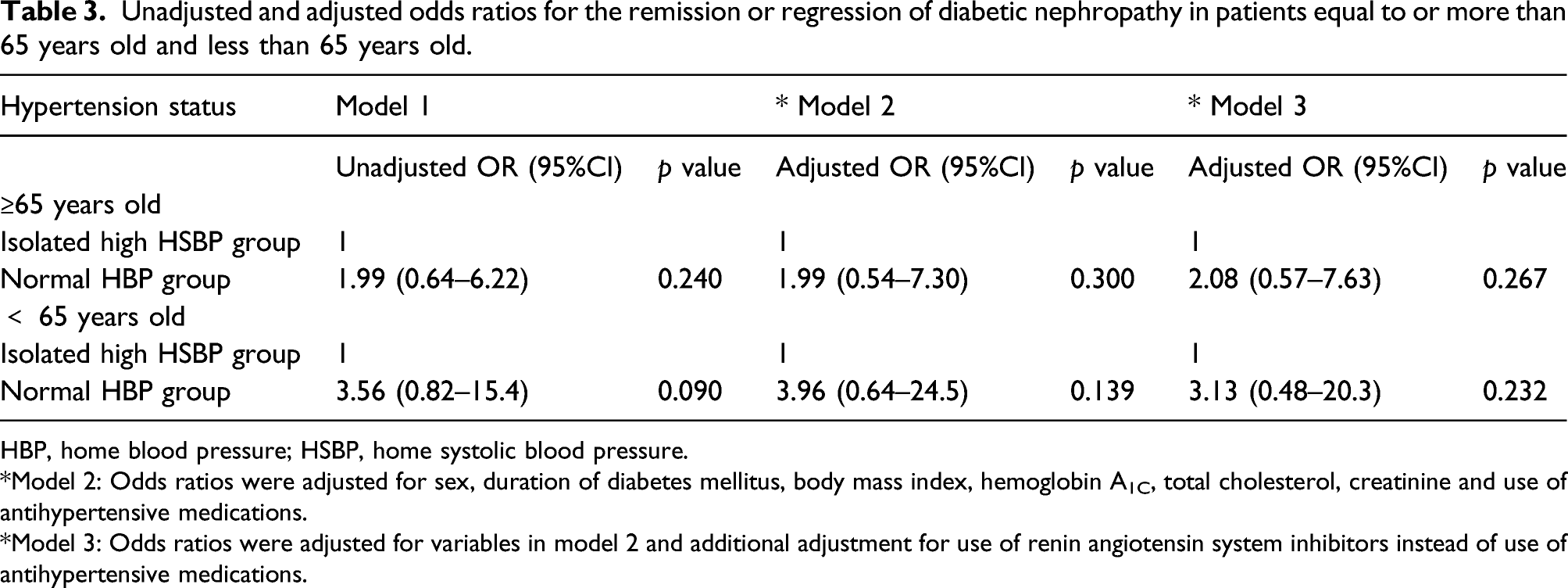
HBP, home blood pressure; HSBP, home systolic blood pressure.
*Model 2: Odds ratios were adjusted for sex, duration of diabetes mellitus, body mass index, hemoglobin A1C, total cholesterol, creatinine and use of antihypertensive medications.
*Model 3: Odds ratios were adjusted for variables in model 2 and additional adjustment for use of renin angiotensin system inhibitors instead of use of antihypertensive medications.
Unadjusted and adjusted odds ratios for the remission or regression of diabetic nephropathy in patients with moderate increased albuminuria and in patients with severe increased albuminuria.
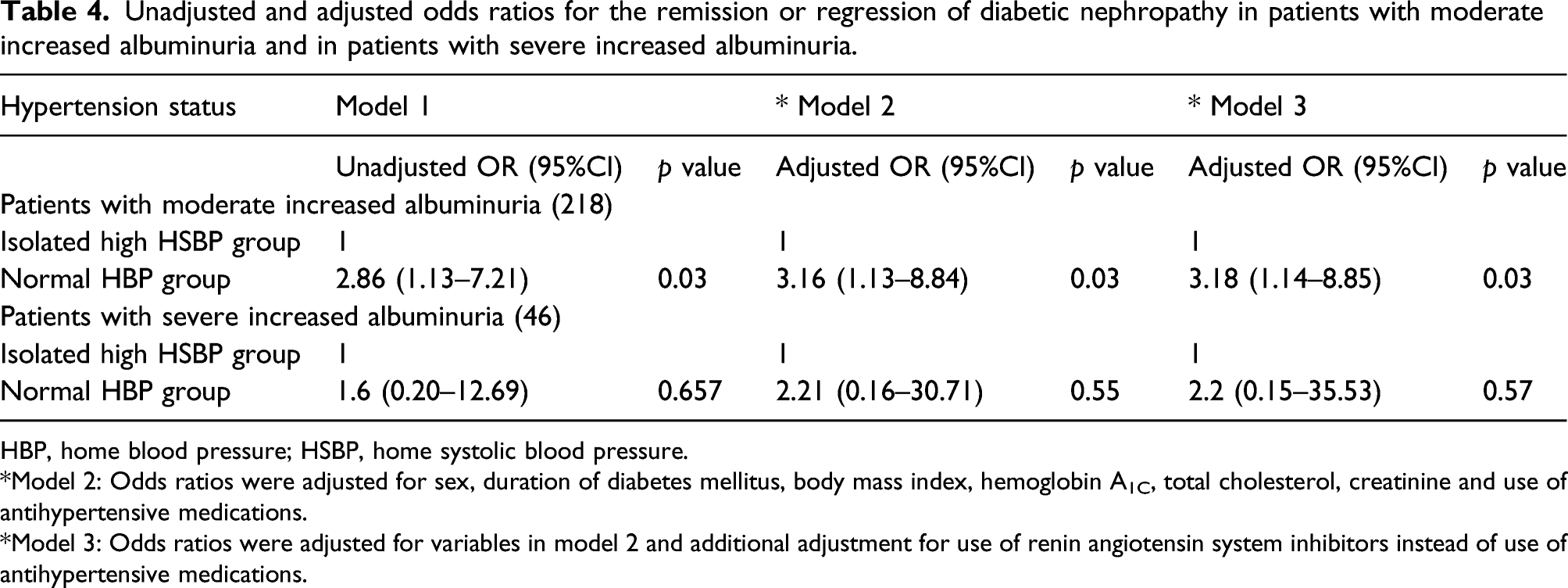
HBP, home blood pressure; HSBP, home systolic blood pressure.
*Model 2: Odds ratios were adjusted for sex, duration of diabetes mellitus, body mass index, hemoglobin A1C, total cholesterol, creatinine and use of antihypertensive medications.
*Model 3: Odds ratios were adjusted for variables in model 2 and additional adjustment for use of renin angiotensin system inhibitors instead of use of antihypertensive medications.
Discussion
Normal home BP was associated with improvement of albuminuria in type 2 diabetic patients during an observation period of 5 years.
A mechanism likely to account for the association between good SBP control and remission or regression of diabetic nephropathy has been described elsewhere.10–15 Inadequately controlled SBP at baseline may induce hemodynamic changes in patients with type 2. 14 The pathogenesis of ISH is enrolled increased arterial stiffness. 30 Furthermore, arterial aging might result in an additional progression in IH-home SBP, which is a risk factor for target-organ damage 31 and diabetic nephropathy. 32 In type 2 diabetes, an association between proteinuria and high BP is strictly related to a higher risk of cardiovascular disease.33,34 Appropriate management is of great importance for advanced type 2 diabetic nephropathy. 35 Therefore, home SBP should be adequately managed (less than 125 mmHg). In home BP management, it is important to clarify that maintaining normal home BP is important for improving nephropathy.
Normal home BP was associated with remission or regression of diabetic nephropathy in this study. The patients in the normal home BP group were younger than those in the IH- home SBP group (64 vs 70 years old, p= 0.001). Arterial stiffness was higher among patients in the IH- home SBP group than in the normal home BP group (1958 vs 1738. m/s, p= 0.006) if comparing arterial stiffness using baPWV measurements between the normal home BP and IH- home SBP groups.22,33 Thus, arterial aging in normal home BP was not advanced, which might be associated with the improvement in diabetic nephropathy.
ISH among young to middle-aged Japanese people is associated with the risk of premature cardiovascular deaths. 34 In the current study, age-stratified subgroup analysis revealed that the adjusted OR was higher among patients aged less than 65 years than in those aged more than or equal to 65 years. Meanwhile, subgroup analyses stratified by use of antihypertensive medications revealed that the adjusted ORs were the same in spite of the presence or absence of ARB/ACE-I. Participants using ARB/ACE-I are at a lower risk of diabetic nephropathy and more frequently experience remission or regression of diabetic nephropathy.10–15 However, remission or regression of diabetic nephropathy was shown less frequently in patients using ARB/ACE-I than in patients not using ARB/ACE-I (17.5% vs. 31.2%) in our study. It should be attention to patients in this group had higher SBP (142.6 vs 135.3 mmHg, p < 0.01) than patients without ARB/ACE-I. Furthermore, they had a longer duration of diabetes (15.0 vs 13.0 years, p < 0.01) and poorer estimated glomerular filtration rate (69.1 vs 74.7 mil/min/1.73m2, p < 0.01). To summarize these results, patients with ARB/ACE-I had remarkable hypertension and developed atherosclerosis and diabetic nephropathy, which consequently counteracted the effectiveness of ARB/ACE-I.
This is the first study to evaluate the impact of normal home BP in improving diabetic nephropathy among type 2 diabetic patients over the medium to long term compared with IH-home SBP to the best of our belief. These results support and strengthen previous reports. In addition, the importance of intensive home BP management among younger patients with diabetes was elucidated through an observation period of 5 years.
Despite, there are some considerable limitations in interpreting the findings. First, data on daily salt intake, protein intake, or exercise intensity, which would be associated with diabetic nephropathy progression, were lack.35,36,37,38 We could not clearly identify the prognostic marker of home BP in the diabetic nephropathy progression even in a longer study in this regard. Second, the study included only Japanese people. Therefore, generalizability of these findings to other ethnic groups may not expect much. Third, we performed only a single baseline BP measurement. This would have resulted in a latent bias. Nevertheless, the association between BP at baseline or during follow-up and target organ damage was confirmed. 28 If the addition of subsequent values did not notably change the results, single BP assessments might be reliable. Fourth, another important issue is the lack of ultrasound findings on kidneys at baseline, particularly the size of kidneys, which should be hypertrophic or enlarged before the development of moderately increased albuminuria. Finally, a non-albuminuric phenotype has been reported in diabetic kidney disease (DKD) of type 2 DM. 39 Therefore, many patients with type 2 DM, despite being normoalbuminuric if they have a glomerular filtration rate (GFR) of less than 60 mil/min/1.73m2, still have DKD. In the present study, we did not include patients with a GFR less than 60 mil/min/1.73m2. Thus, we were not able to evaluate the decline in renal function according to in the definition of DKD in this study. Further studies will be conducted in the future.
In conclusion, normal home BP in type 2 diabetic patients was a prognostic marker for the improvement of diabetic nephropathy in a prospective cohort study of 5 years.
Footnotes
Acknowledgements
We thank Naoko Higo R.N., Terumi Kaneko R.N., and Machiko Hasegawa R.N. of the Kyoto Prefectural University of Medicine, for teaching patients how to measure their blood pressure and Sayoko Tanaka also of the Kyoto Prefectural University of Medicine, for their secretarial assistance. We thank
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article Emi Ushigome received grant support from the Japanese Study Group for Physiology and Management of Blood Pressure, the Astellas Foundation for Research on Metabolic Disorders (Grant number: 4024), the Japan Society for the Promotion of Science, Mishima Kaiun Memorial Foundation, and received personal fees from Nippon Boehringer Ingelheim Co., Ltd., Mitsubishi Tanabe Pharma Corporation, LIMITED, Ltd., Takeda Pharmaceutical Company Ltd., Novo Nordisk Pharma Ltd., MSD K.K., DAIICHI SANKYO COMPANY, Kyowa Hakko Kirin Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Kowa Pharmaceutical Co., Ltd., Ono Pharmaceutical Co., Ltd., Taisho Pharmaceutical Co., AstraZeneca K.K., and Sanofi K.K., outside the submitted work. Donated Fund Laboratory of Diabetes therapeutics is an endowment department, supported with an unrestricted grant from Taiyo Kagaku Co. Ltd., Ono Pharmaceutical Co., Ltd., and Taisho Pharmaceutical Co., Ltd. Mai Asano received personal fees from Kowa Pharmaceutical Co., Ltd., Abbott Japan Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Takeda Pharmaceutical Co., Ltd., Ono Pharmaceutical Co., Ltd., Novo Nordisk Pharma Ltd., AstraZeneca K.K., and Chugai Pharmaceutical Co., Ltd., outside the submitted work. Masahide Hamaguchi received grants from AstraZeneca K.K., Nippon Boehringer Ingelheim Co. Ltd., Ono Pharma Co. Ltd., Oishi Kenko inc., Yamada Bee Farm, and received personal fees from Ono Pharma Co. Ltd., AstraZeneca K.K., Eli Lilly, Japan, Mitsubishi Tanabe Pharma Corp., Sumitomo Dainippon Pharma Co., Ltd., Daiichi Sankyo Co. Ltd., Sanofi K.K., Kowa Pharma Co. Ltd., outside the submitted work. Masahiro Yamazaki reports personal fees from MSD K.K., personal fees from Sumitomo Dainippon Pharma Co., Ltd., personal fees from Kowa Company, Limited, personal fees from Takeda Pharmaceutical Company Limited, personal fees from AstraZeneca PLC, personal fees from KOWA PHARMACEUTICAL COMPANY LTD., personal fees from Kyowa Hakko Kirin Co., Ltd., personal fees from DAIICHI SANKYO COMPANY, LIMITED, personal fees from ONO PHARMACEUTICAL CO., LTD., outside the submitted work. Isao Yokota reports grants from KAKENHI, AMED, and Health, Labour and Welfare Policy Research Grants, research fund by Nihon Medi-Physics, and speaker fees from Chugai Pharmaceutical Co, AstraZeneca plt, Japan Tabacco Pharamaceutical Division, and Nippon Shinyaku Co, outside the submitted work. Michiaki Fukui received grant support from Ono Pharma Co. Ltd., Oishi Kenko inc., Yamada Bee Farm, Nippon Boehringer Ingelheim Co. Ltd., Kissei Pharma Co. Ltd., Mitsubishi Tanabe Pharma Corp., Daiichi Sankyo Co. Ltd., Sanofi K.K., Takeda Pharma Co. Ltd., Astellas Pharma Inc., MSD K.K., Kyowa Kirin Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Kowa Pharma Co. Ltd., Novo Nordisk Pharma Ltd., Sanwa Kagagu Kenkyusho CO., Ltd., Eli Lilly, Japan, K.K., Taisho Pharma Co., Ltd., Terumo Corp., Tejin Pharma Ltd., Nippon Chemiphar Co., Ltd., Abbott Japan Co. Ltd., and Johnson & Johnson K.K. Medical Co., TERUMO CORPORATION, and received personal fees from Nippon Boehringer Ingelheim Co., Ltd., Kissei Pharma Co., Ltd., Mitsubishi Tanabe Pharma Corp., Daiichi Sankyo Co. Ltd., Sanofi K.K., Takeda Pharma Co. Ltd., Astellas Pharma Inc., MSD K.K., Kyowa Kirin Co. Ltd., Sumitomo Dainippon Pharma Co. Ltd., Kowa Pharma Co. Ltd., Novo Nordisk Pharma Ltd., Ono Pharma Co. Ltd., Sanwa Kagaku Kenkyusho Co. Ltd., Eli Lilly Japan K.K., Taisho Pharma Co., Ltd., Bayer Yakuhin, Ltd., AstraZeneca K.K., Mochida Pharma Co. Ltd., Abbott Japan Co. Ltd., Teijin Pharma Ltd., Arkray Inc., Medtronic Japan Co. Ltd., and Nipro Corp., TERUMO CORPORATION, outside the submitted work. The sponsors were not concerned with the study design, collection, analysis, interpretation of data, nor in the writing of this manuscript, nor in the decision to submit the article for publication. The authors, their immediate families, and any research foundations with which they are affiliated have not received any financial benefits from any commercial entity related to the subject of this article. The authors declare that although they are affiliated with a department that is supported financially by pharmaceutical company, the authors received no financial benefits for this study and department affiliation does not alter their adherence to all journal policies on sharing data and materials.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by EU received grant support from the Japanese Study Group for Physiology and Management of Blood Pressure and the Astellas Foundation for Research on Metabolic Disorders [grant number: 4024].