
Abstract
Objective:
To compare clinical outcomes in diabetic patients with heart failure managed by insulin with those managed by non-insulin (oral hypoglycemic agents and/or lifestyle modification) based therapy.
Methods:
PubMed and Scopus databases were searched for studies conducted on diabetic patients with heart failure. Studies were to compare outcomes of patients managed by insulin versus non-insulin therapies.
Results:
15 studies were included. Compared to those who were managed using non-insulin therapy, insulin-treated patients had increased risk of all-cause mortality (RR 1.46, 95% CI: 1.14, 1.88) and cardiovascular specific mortality (RR 1.62, 95% CI: 1.33, 1.96). Those managed using insulin also had increased risk of hospitalization (RR 1.45, 95% CI: 1.09, 1.93) and readmission (RR 1.49, 95% CI: 1.32, 1.67). There was no additional risk for stroke (RR 1.07, 95% CI: 0.91, 1.27) or myocardial infarction (MI) (RR 1.10, 95% CI: 0.96, 1.27) between the two groups of patients.
Conclusions:
Receipt of insulin among diabetic patients with heart failure was associated with an increased risk of mortality, hospitalization and readmission compared to management using oral hypoglycemic agents and/or lifestyle modification. Such patients should be closely monitored for any adverse events.
Keywords
Introduction
There has been a global upsurge in the incidence of diabetes mellitus as well as heart failure in the recent years. According to the Global burden of disease (2017) estimates, the incidence of diabetes was ∼23 million and the disability-adjusted life-years (DALYs) associated with diabetes was ∼68 million. 1 Prevalence of type 2 diabetes mellitus has increased by ∼30% in the last decade. In 2005, the prevalence was 333 million which rose to 435 million by 2015. 2 The incidence of heart failure is also alarming with ∼26 million people affected worldwide.3,4 Both diseases share a strong inter-association. Studies indicate over 2 times higher risk of heart failure in subjects with type 2 diabetes mellitus.5,6 Additionally, presence of type 2 diabetes increases the risk of adverse cardiovascular outcomes, mortality, hospitalization, and leads to overall unfavorable prognosis among those with pre-existing cardiac disease, in comparison to those without diabetes.5,7–9
The underlying mechanisms leading to poor outcomes in diabetics have been postulated to be around disruption and dysregulation of cellular mechanisms. The increased oxidative stress, underlying inflammation, inflammation of coronary endothelium, non-regulated insulin signaling, increased levels of advanced glycated end-products, and alterations in myocardial substrate metabolism as well as signal transduction have been proposed to be some of the key factors.5,10–13 Presence of diabetes also brings some key structural and functional changes such as left ventricular systolic dysfunction, increase in left ventricular mass and wall thickness, diastolic dysfunction along with a notable increase in extracellular volume fraction .14–17 These changes also contribute to an increased risk of poor outcomes.
Many of these underlying factors and pathophysiological mechanisms might be counteracted through use of pharmacological therapy for management of diabetes mellitus. 5 This, in turn, may reduce the risk of heart failure and its associated complications and possibly, improve prognosis. 5 Insulin is a commonly used second-line pharmacological agent for managing type 2 diabetes. 18 However, a concern with use of insulin is the associated risk of sodium and fluid retention and hypoglycemia which could further accentuate heart failure and worsen outcomes .19–21 There is a lack of systematic evidence on the safety and efficacy of use of insulin in patients with heart failure and concomitant type 2 diabetes, compared to other modes of management such as oral hypoglycemic agents and/or lifestyle modifications. Studies have attempted to analyze the impact of management using insulin on outcomes of heart failure, but the findings of these studies have not been systematically synthesized. There is a need to conduct a careful systematic review and meta-analysis to document and synthesize the findings of these studies and present conclusive and updated evidence that could guide clinical practices. The current meta-analysis was therefore undertaken with the aim to understand the effect of use of insulin therapy, compared to other non-insulin-based management strategies, on clinical outcomes in patients with concomitant diabetes and heart failure.
Methods
Search strategy
A literature search of manuscripts published, only in English, ending November 1, 2021, was executed using both PubMed and Scopus. The implemented search focused on medical subject heading (MeSH) terminology and free text words. Details of our search strategy are summarized in Supplementary Table 1. Our literature search targeted studies conducted among diabetic patients with heart failure and had presented outcomes of interest based on the mode of management of diabetes, that is, managed by insulin or non-insulin management comprising of oral hypoglycemic drugs and/or diet and lifestyle modification. The primary outcomes of interest were all-cause mortality and cardiovascular specific mortality. Secondary outcomes included hospitalization for heart failure, readmission for heart failure, risk of myocardial infarction and stroke. Study processes followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines. 22 The protocol for this meta-analysis was registered in the International Prospective Registry of Systematic Reviews (PROSPERO; registration number CRD42021290253).
Selection criteria and methods
Studies, retrieved through literature searches, were both identified and reviewed by two subject experts. Initial screening focused on title and abstracts from the retrieved results. Subsequently, duplicate results were discarded. Finally, the subject experts reviewed content from the full texts of each of the remaining studies to determine inclusion or exclusion. In rare cases, disagreements between subject experts occurred. These were resolved through internal discussion and evaluation until a consensus was reached. Only studies consistent with our inclusion criteria were selected for the meta-analysis.
Inclusion criteria
Studies that were either observational in design (retrospective cohort, prospective cohort, case-control) or randomized trials were included in the meta-analysis. For inclusion studies were required to have been conducted among patients with heart failure and associated diabetes. Further, the study should have examined the outcomes of interest between the two groups of patients, that is, those managed with insulin and those managed using oral hypoglycemic agents and/or lifestyle modification.
Exclusion criteria
Studies which were reported as review articles or case-reports were excluded from the current meta-analysis. Also, studies that omitted results on outcomes of interest or excluded present comparative findings between those managed with insulin and those with non-insulin-based management were excluded.
Data extraction and quality assessment
Using a data extraction sheet, relevant data was extracted from the included studies by two separate authors. Specifically, authors focused on extracting key information such as year of publications, study author name, study settings, pertinent subject characteristics, study design including sample size and finally, results. The Newcastle-Ottawa Quality Assessment Scale was use for observational studies and consequently used for quality assessment. 23
Statistical analysis
The current study was conducted using STATA version 16.0. The effect sizes were reported as pooled relative risk (RR) with 95% CI (confidence intervals). Subgroup analysis was done based on study design and etiology of heart failure (i.e., ischemic or non-ischemic). I2 test measured heterogeneity and identify situations where I2 > 40%, random effects model was used. 24 A p-value < 0.05 was statistically significant. To assess the presence or the absence of any publication bias of the data, an Egger’s test was implemented. 25
Results
Article selection, study characteristics, and quality evaluation
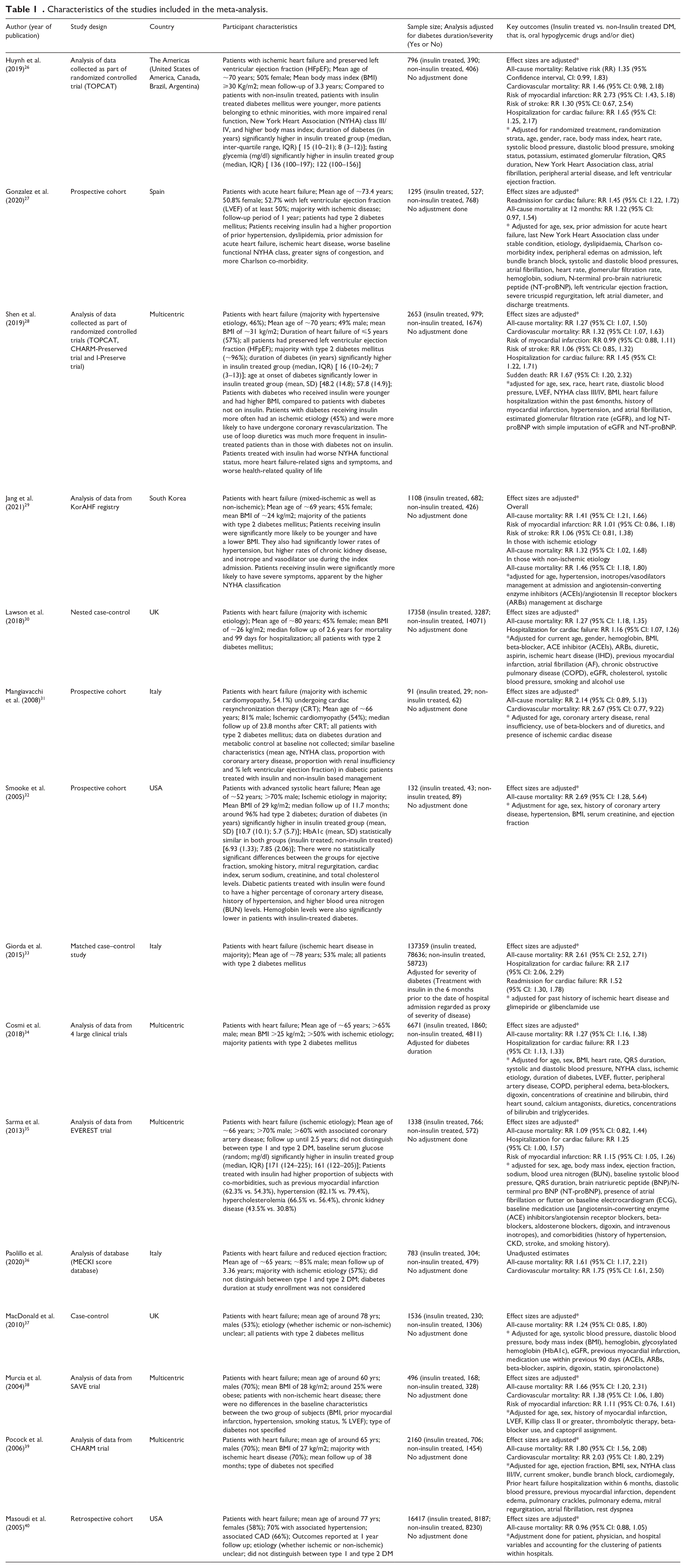
Utilizing the aforementioned literature search method, and subsequently removing duplicated results, a total of 1284 citations were obtained (Figure 1). Filtering of titles and abstracts led to removal of 1239 citations. From the remaining 45 studies, 30 were excluded after reading the full text. Finally, a total of 15 studies were selected for inclusion.26–40 Table 1 presents the details of the included studies. Six studies were based on analysis of data collected as part of randomized controlled trials (RCTs). Three each were prospective cohort and case-control studies respectively. Two studies were based on analysis of data collected as part of registry and one was a retrospective cohort in design. Five studies were multicentric and one was done in the Americas (i.e., USA, Canada, Brazil, and Argentina). Three studies were conducted in Italy, 2 in USA, 2 in United Kingdom, and one study each in Spain and South Korea. In most of the studies, majority of the patients had ischemic heart disease (n =10). In almost all the included studies, the comparison group consisted of subjects managed with oral hypoglycemic drugs. A total of 9 studies had subjects with type 2 diabetes mellitus and in remaining, data on type of diabetes was not provided. Quality evaluation of studies included in our analysis are summarized in Supplementary Tables 2 and 3. Included studies were of modest to good quality. There was a possibility that some TOPCAT data may be double counted by including both of the Huynh and Shen analyses.26,28 Similarly, some of the CHARM trial data may be duplicated by inclusion of Shen and Pocock analyses.28,39 In order to overcome, we conducted a sensitivity analysis by excluding studies by Huynh et al. and Pocock et al.26,39
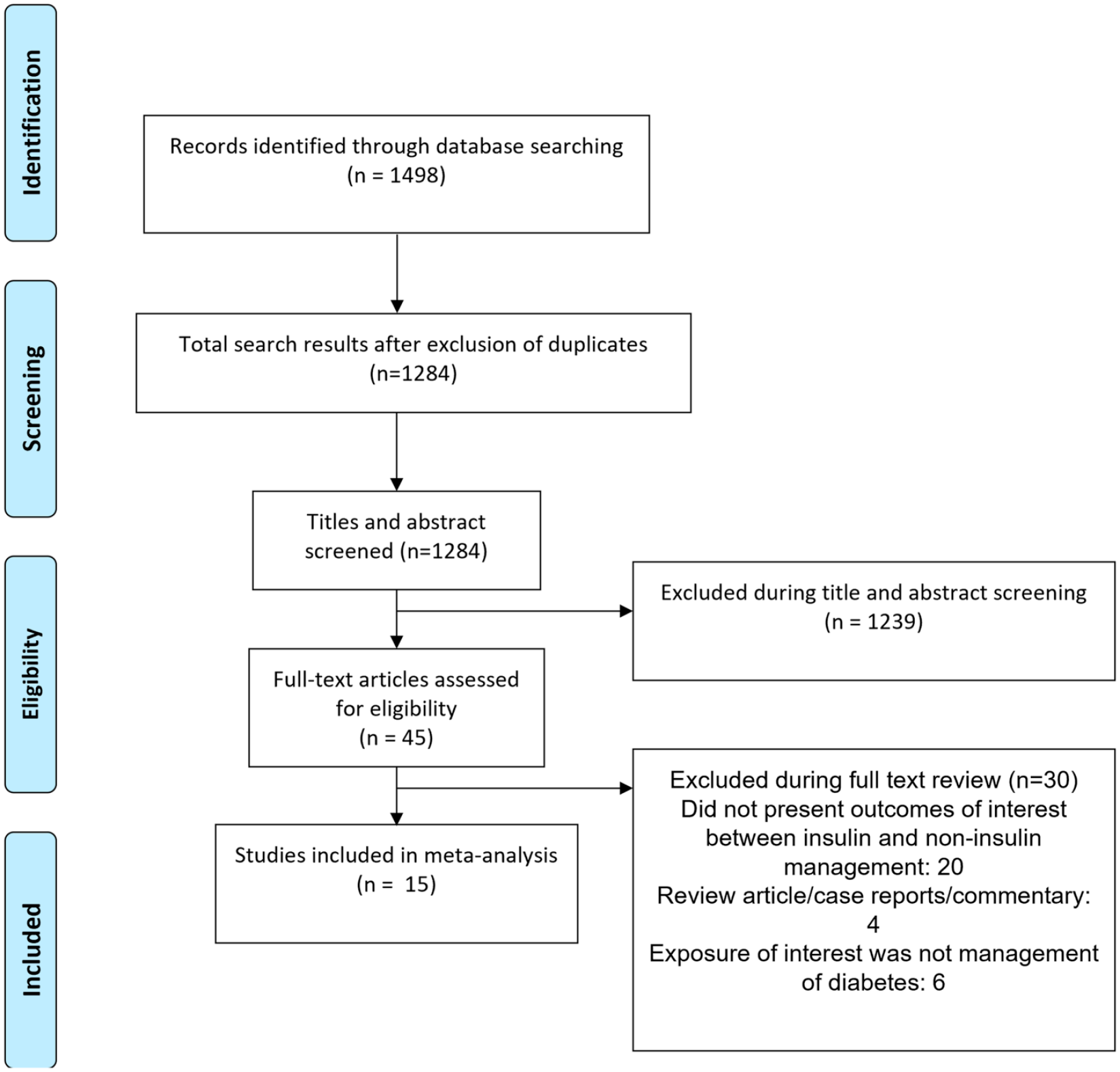
Selection process of the studies included in the review.
Characteristics of the studies included in the meta-analysis.
Effect on mortality outcomes
Compared to those who were managed using non-insulin therapy (i.e., oral hypoglycemic agents and/or diet), those managed using insulin had increased risk of all-cause mortality (RR 1.46, 95% CI: 1.14, 1.88; N = 15; I2 = 98.3%) and cardiovascular specific mortality (RR 1.62, 95% CI: 1.33, 1.96; N=6; I2 = 70.7%) (Figure 2). Results from the Egger’s test indicate no publication bias (p = 0.27 for all-cause mortality; p = 0.18 for cardiovascular specific mortality). The findings on sensitivity analysis after exclusion of studies by Huynh et al. and Pocock et al. were statistically similar to the overall pooled findings (supplementary figure 1).
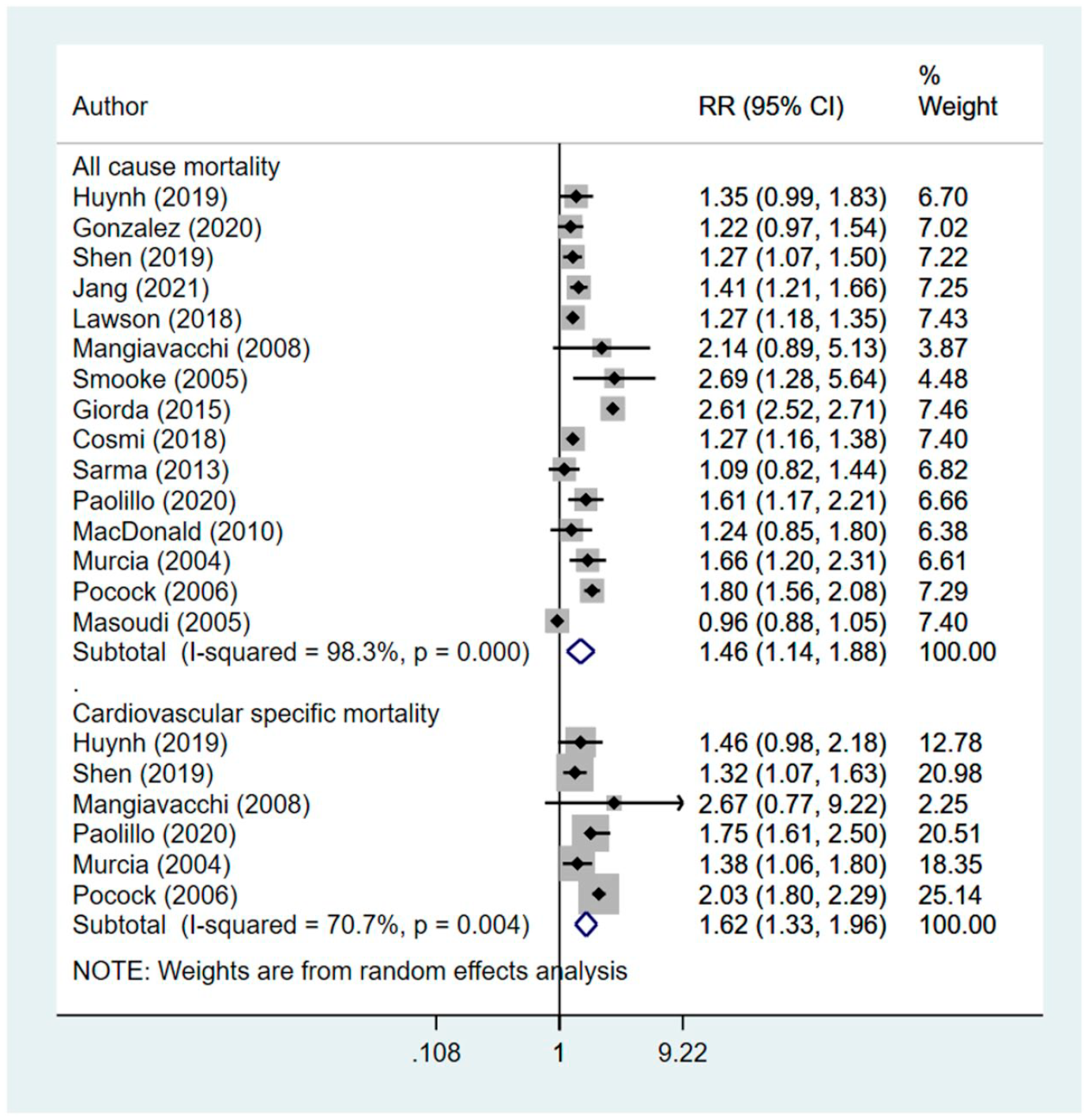
Effect of management of diabetes using insulin, compared to non-insulin management in patients with heart disease on mortality related outcomes.
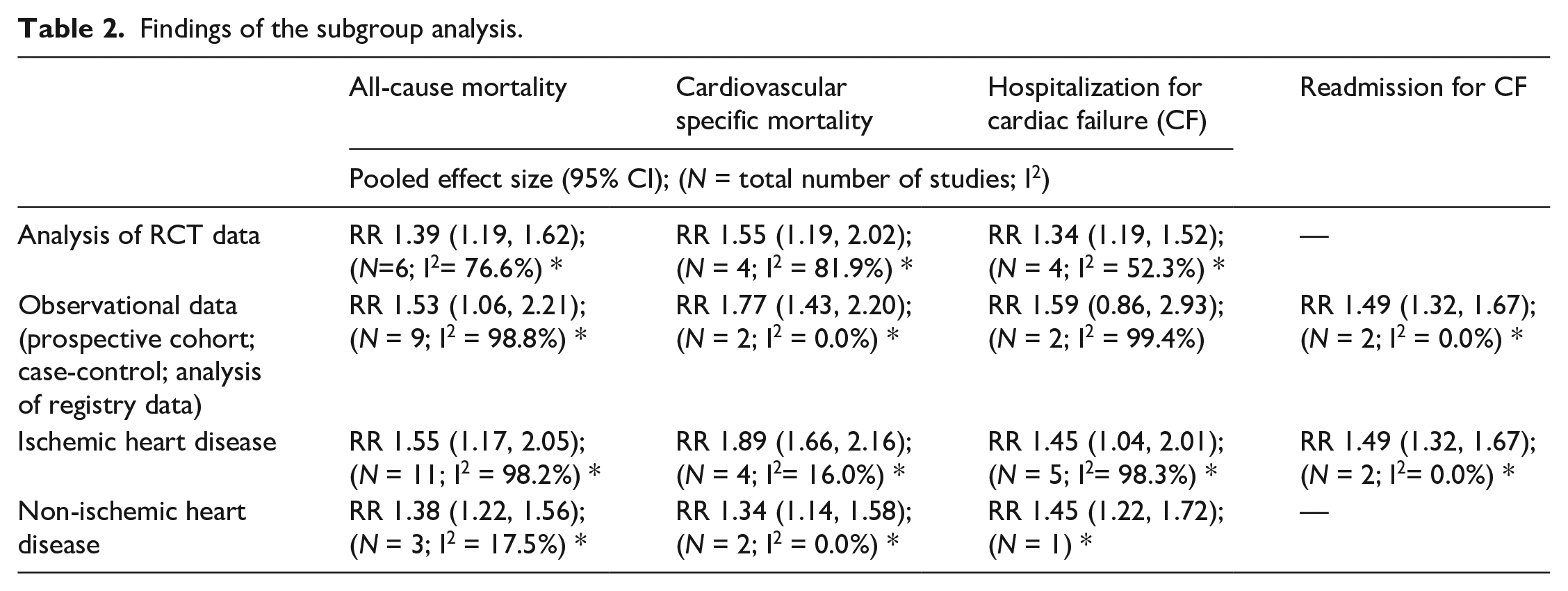
Subgroup analysis indicated that in both ischemic and non-ischemic heart disease, the pooled effect size for all-cause mortality as well as cardiovascular specific mortality was higher in diabetics managed with insulin, compared to those undergoing non-insulin management Table 2). However, the number of studies with non-ischemic heart failure were few. Further, the risk of mortality was higher when only studies with observational design were pooled, compared to when only RCTs were pooled (Table 2).
Findings of the subgroup analysis.
Effect on secondary outcomes
Compared to those who were managed using non-insulin therapy, those managed using insulin had increased risk of hospitalization (RR 1.45, 95% CI: 1.09, 1.93; N = 6; I2 = 97.8%) and readmission (RR 1.49, 95% CI: 1.32, 1.67; N = 2; I2 = 0.0%) (Figure 3). There was no additional risk for stroke (RR 1.07, 95% CI: 0.91, 1.27; N = 3; I2 = 0.0%) or myocardial infarction (MI) (RR 1.10, 95% CI: 0.96, 1.27; N = 5; I2 = 68.4%) between the two groups. Egger’s test did not indicate the presence of publication bias (p = 0.42 for hospitalization; p = 0.13 for readmission; p = 0.65 for stroke and p = 0.43 for MI). The findings on sensitivity analysis after exclusion of studies by Huynh et al. and Pocock et al. were statistically similar to the overall pooled findings (supplementary figure 2).
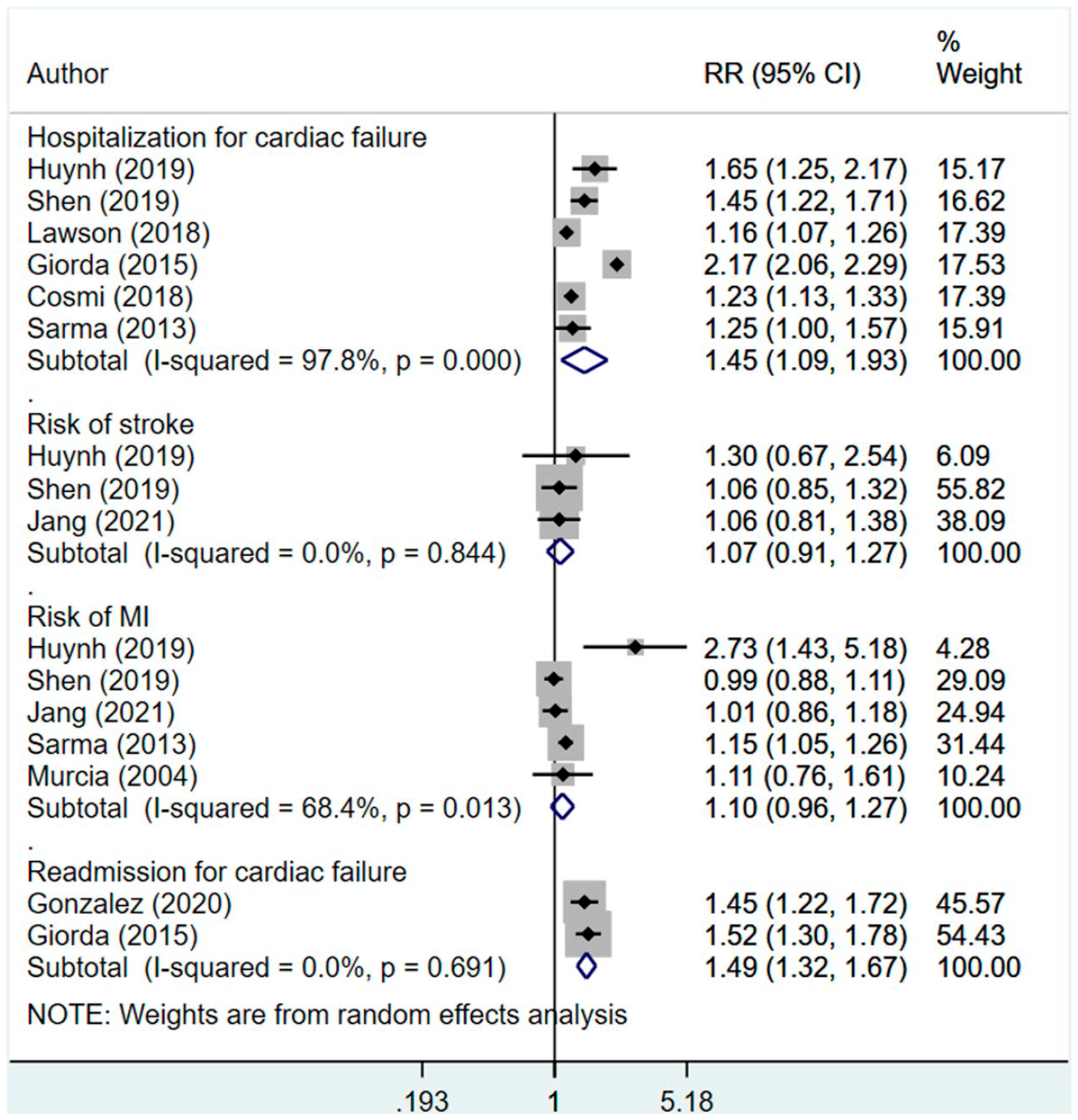
Effect of management of diabetes using insulin, compared to non-insulin management in patients with heart disease on hospitalization, readmission, stroke, and myocardial infarction.
In subgroup analysis, the risk of hospitalization was higher when only studies with observational design were pooled (RR 1.59, 95% CI: 0.86, 2.93; N = 2; I2 = 99.4%), compared to when only RCTs were pooled (RR 1.34, 95% CI: 1.19, 1.52; N = 4; I2 = 52.3%) (Table 2). In both ischemic and non-ischemic heart disease, the pooled effect size for hospitalization was higher in diabetics managed with insulin, compared to those undergoing non-insulin management; however, the number of studies with patients having non-ischemic heart failure were few (Table 2).
Discussion
It is well established that presence of diabetes adversely affects the outcomes and prognosis of heart failure.5,8,9,41 In addition, available literature does provide support that pharmacological management of diabetes offers some improvement in the clinical outcomes of heart failure. 5 However, the nature of pharmacological management also has an impact on outcomes. Our review showed that use of insulin was associated with an increased the risk of adverse outcomes, compared to non-insulin-based management. One of the potential explanations for an increased risk of adverse outcome in patients managed with insulin is related to its sodium and water retention properties.20,42 The anti-natriuretic effect of insulin is due to reduction in glycosuria and a consequent decrease in sodium excretion. 42 Further, insulin increases sodium and water absorption in the nephrons. This results in increase in vascular volume and leads to increased cardiac work overload. 42 Another plausible explanation is related to the increased risk of hypoglycemia which is common in patients managed with insulin. 43 Hypoglycemia has adverse cardiovascular effects through sympathetic activation culminating into increased heart rate (i.e., tachycardia), myocardial infarction, and a substantial lowering of blood potassium level (i.e., hypokalemia).44,45 All these predispose to a pro-thrombotic state and increase the risk of arrhythmias. There has been recent emerging evidence that insulin might lead to reduced contractility of heart through induction of Gi-biased beta 2-adrenergic signaling in hearts. 46
One of the known adverse effects of exogenous insulin is the increase in insulin levels above normal physiological threshold in systemic circulation leading to hyperinsulinemia. 47 A state of hyperinsulinemia has a wide variety of negative effects such as increased insulin resistance, excessive weight gain, derangement in lipid profile, inflammation, and exhaustion of beta-cells.48–51 Cardiac muscles derive their energy from oxidation of free fatty acids and not from glucose. This is the reason why cardiac myocardium is relatively resistant to insulin action. 50 Exogenous insulin administration led hyperinsulinemia counteracts the natural insulin resistance that myocardium has, and this leads to increased glucose entry and consequent glucolipotoxicity. 50 Studies have shown that hyperinsulinemia can lead to cardiomyopathy, induce endothelial dysfunction and increase the risk of atherosclerosis.52–54 Such adverse effects could be attributed to underlying pathophysiological derangements such as suppression of important pathways like those involved in production of nitric oxide and phosphatidylinositol-3-kinase signaling.53,54 Exogenous insulin predisposes to weight gain and increased adiposity that can accentuate underlying inflammatory environment and increase the levels of circulating inflammatory cytokines. 55 This could also increase the risk of poor cardiovascular outcomes.
There are certain limitations of the current study. Insulin therapy is never the first line for the treatment of type 2 diabetes and reflects more severe or longer disease duration compared to patients managed with oral hypoglycemics or lifestyle advice. In the included studies, not all provided a comparison of the duration and severity of diabetes among the two groups. Further, a total of 9 studies only had subjects with type 2 diabetes and in the remaining 6 studies, no clear distinction was made based on type of diabetes. In studies that provided data on diabetes duration, the age at onset was earlier and the duration of diabetes was more in those that were managed with insulin, compared to non-insulin treated group. Also, the data provided by the included studies clearly demonstrates that those receiving insulin therapy had comparatively worse baseline clinical parameters and a higher prevalence of comorbidities, compared to those receiving non-insulin based management. It is not surprising therefore, that patients treated with insulin could have comparatively worse outcomes. Further, in most of the studies, the statistical model was not adjusted for diabetes duration and/or severity and therefore, it may not be able to conclude conclusively that receipt of insulin worsens outcomes. This argument is further supported by the observations from some of the trials, such as ORIGIN, UKPDS and BARI-2D,56–58 that investigated the effect of insulin monotherapy on cardiovascular safety in apparently healthy individuals, including incident heart failure. These trials found no difference in any cardiovascular outcomes, including hospitalization for heart failure, when compared to standard care. On the contrary, observational studies among apparently healthy subjects with diabetes suggested an increase in risk of incident heart failure with insulin therapy. However, the possibility that the effect is modified by residual confounding cannot be ruled out. These are important considerations while interpreting the findings of this meta-analysis. This analysis includes a diverse range of participants (stable outpatients, hospitalized patients, reduced and preserved ejection fraction) and study designs. This could be a potential methodological weakness and limits the generalizability of the findings.
Another important point is that there could be a switch in treatment provided to the study subjects, that is, there would be subjects that were initially started on oral hypoglycemic drugs and then shifted to insulin treatment or vice-versa. While this shift in treatment may impact the outcome, most of the included studies did not account for this in the analysis. It would have been interesting to know whether there were differences, if any, between the ambulatory/hospitalized patients or those with reduced and preserved ejection fraction. These subgroup analyses could not be done as the included studies did not present findings stratified by these subgroups. Majority of the studies included in this meta-analysis were observational in design and some of them analyzed data from a randomized controlled trial that was not designed to test the hypothesis under consideration. Therefore, the possibility that some important confounders are not adjusted for, cannot be ruled out. The present meta-analysis could not conclusively ascertain the differential risk of insulin therapy, if any, in individuals suffering from either ischemic or non-ischemic heart failure mainly because only few studies included patients with non-ischemic heart failure. An additional limitation was the use of only PubMed and Scopus databases, with the possibility that other studies might have been identified using wider search criteria.
Conclusion
Based on pooling of findings from 15 studies, the meta-analysis noted a significant association between insulin-based management and all-cause mortality, cardiovascular specific mortality, hospitalization due to cardiac failure and readmission among subjects with heart failure and concomitant type 2 diabetes. However, there are certain methodological limitations and therefore careful interpretation of the findings of this meta-analysis is warranted. Nonetheless, necessary caution should be exercised in patients with type 2 diabetes mellitus that are started on insulin therapy. For those who are undergoing insulin-based management, regular follow up and careful supervision is necessitated.
Key messages
We compared clinical outcomes in diabetic patients with heart failure managed by insulin. Management of diabetes among patients with heart failure using insulin might be associated with an increased risk of mortality, hospitalization, and readmission. This increased risk of adverse outcomes should be carefully interpreted as the findings may be influenced by methodological limitations of the studies
Supplemental Material
sj-docx-1-dvr-10.1177_14791641221093175 – Supplemental material for Impact of insulin therapy on outcomes of diabetic patients with heart failure: A systematic review and meta-analysis
Supplemental material, sj-docx-1-dvr-10.1177_14791641221093175 for Impact of insulin therapy on outcomes of diabetic patients with heart failure: A systematic review and meta-analysis by Jingxing Liu and Xinhua Hu in Diabetes & Vascular Disease Research
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.