
Abstract
Aim:
The aim of this study was to investigate the association between the transcription factor 7-like 2 gene (TCF7L2) rs7903146 polymorphism and peripheral arterial disease in type 2 diabetes.
Methods:
In total, 1818 Korean type 2 diabetes patients were enrolled from January 2013 to December 2017. Subjects were categorized into two groups according to their duration of type 2 diabetes: long (⩾10 years, n = 771) and short (<10 years, n = 1047) durations. A multivariate logistic regression model was used for assuming an additive effect on peripheral arterial disease for the presence of a variant allele in TCF7L2 rs7903146.
Results:
The frequency of the minor T-allele was 7.6% (n = 139), and this allele was significantly associated with a 2.6-fold higher risk of peripheral arterial disease (odds ratio = 2.595, 95% confidence interval = 1.177–5.722, p = 0.018) in patients exhibiting a long duration of type 2 diabetes (⩾10 years). This result was significant after adjusting for age, sex, body mass index, familial history of diabetes, smoking, duration of diabetes and laboratory measurements, which included glycated haemoglobin, fasting plasma glucose and lipid profiles. In patients with diabetes < 10 years, there was no significant association between TCF7L2 rs7903146 and peripheral arterial disease (odds ratio = 1.233, 95% confidence interval = 0.492–3.093, p = 0.655).
Conclusion:
Our results provide evidence that genetic variation in TCF7L2 rs7903146 could increase risk for peripheral arterial disease in patients exhibiting long-standing type 2 diabetes.
Introduction
Peripheral arterial disease (PAD) contributes to reduced quality of life derived from intermittent claudication, morbidity from non-healing ulcers and a potential major amputation leading to significant disability. 1 Beyond local lower-extremity complications, PAD is strongly associated with higher risk of incident cardiovascular and cerebrovascular diseases, or even higher all-cause mortality. 2 The burden of PAD is significantly higher among patients with type 2 diabetes (T2D) as shown in the UK Prospective Diabetes Study [28% increased risk of PAD per 1% increase in glycated A1c (HbA1c) level]. 3 Still, there is a relatively lack of active interventions to treat PAD compared to other cardiac or cerebral complications in T2D.
In a recently published genome-wide association study, 126 variants at four loci associated with risk of T2D were reported. 4 Among many T2D-related genes, the genetic variant of the transcription factor 7-like 2 (TCF7L2) gene has been shown to be reproducibly associated with T2D in various ethnicities. 5
To date, there is limited information regarding the association between TCF7L2 rs7903146 polymorphism and PAD in patients with T2D. Therefore, the objective of this study was to evaluate the association between gene variant TCF7L2 rs7903146 and prevalent PAD in the patients with long-standing T2D.
Methods
Subjects
In total, 1818 subjects with T2D who visited the Diabetes Centre at Chungbuk National University Hospital from January 2013 to December 2017 were recruited. T2D were diagnosed according to the criteria from the American Diabetes Association. 6 Exclusion criteria were a diagnosed type 1 diabetes, gestational diabetes, diabetes due to other causes and malignancies. For a better prediction of the risk for diabetic complications in subjects with T2D, we further classified all subjects into two groups: long duration of diabetes group (⩾10 years, n = 771) and short duration of diabetes group (<10 years, n = 1047) according to their age at diabetes diagnosis. PAD was defined as ankle–brachial index (ABI) ⩽ 0.9 or previous history of lower extremity bypass and/or endovascular therapy. Details of the obtained clinical, laboratory data and measurement of ABI are presented in the Supplementary Methods. The study was conducted according to the principles of the revised Declaration of Helsinki, a statement of ethical principles to provide guidance to physicians and other participants in medical research involving human subjects. All participants provided their written informed consent. All samples derived from the National Biobank of Korea were obtained with informed consent under institutional review board of Chungbuk National University Hospital–approved protocols (IRB No. 2019-04-026).
TCF7L2 genotyping
Genomic DNA was isolated and stored at −20°C. Genotyping master mix and fluorescent probes were used for variant detection by real-time polymerase chain reaction (PCR) system (Supplementary Methods). Frequency of the genotype was calculated to be in Hardy–Weinberg equilibrium (p = 0.644).
Statistical analysis
We analysed the association between TCF7L2 rs7903146 variant and PAD using following multivariate logistic regression models: model 1 unadjusted; model 2 adjusted for age, sex and body mass index (BMI); model 3 further adjusted for familial history of diabetes, smoking, laboratory measurements including HbA1c, and lipid profiles. Statistical analyses were performed with SPSS Statistics for Windows, version 24.0 (IBM Corp., Armonk, NY, USA) (Supplementary Methods).
Results
Baseline characteristics
The baseline characteristics of the subjects (994 males and 824 females) according to the TCF7L2 rs7903146 polymorphism are summarized in Supplementary Table S1. The majority of the patients (1679; 92.4% of the total patients analysed) were identified with C/C genotype with the remaining 139 patients having either heterozygous C/T (n = 137 or 7.5% of the total patients) or homozygous T/T (n = 2 or 0.1% of the total patients) at the TCF7L2 rs7903146 site. No significant difference was found in anthropometric and biochemical variables between groups.
Clinical risk factors for PAD
The prevalence of PAD was 10.7% (n = 195) in patients with T2D, and significantly higher (p < 0.008) in patients with long (⩾10 years; n = 100 out of 771 patients or 13%) versus short (<10 years; n = 95 out of 1047 patients or 9.1%) durations. Supplementary Table S2 shows odds ratios (ORs) of PAD. Age [OR = 1.047, 95% confidence interval (CI) = 1.032–1.062], male (OR = 1.670, 95% CI = 1.223–2.280), presence of familial history of diabetes (OR = 1.616, 95% CI = 1.180–2.213), current smoking (OR = 2.138, 95% CI = 1.344–3.401) and comorbid hypertension (OR = 2.536, 95% CI = 1.801–3.572) were associated with PAD (all p < 0.05). Serum total cholesterol (⩾200 mg/dL), triglyceride (⩾250 mg/dL) and low-density lipoprotein (LDL) cholesterol (⩾100 mg/dL) were also associated with PAD, with ORs of 1.866 (95% CI = 1.166–2.986), 1.975 (95% CI = 1.101–3.541) and 2.272 (95% CI = 1.294–3.990), respectively (all p < 0.05). However, overweight (BMI ⩾ 25 kg/m2) and hyperglycaemia (HbA1c ⩾ 7.0% or fasting plasma glucose ⩾ 126 mg/dL) and lower high-density lipoprotein (HDL) cholesterol levels (male < 40 mg/dL, female < 50 mg/dL) showed no significant association with PAD.
Association between the TCF7L2 polymorphism rs7903146 and PAD
Overall, the distribution of the genotypes in the patients with PAD was as follows: C/T or T/T (n = 20 patients or 14.4%) and C/C (n = 175 patients or 10.4%) (OR = 1.444, 95% CI = 0.877–2.379, p = 0.149) (Supplementary Table S3). In patients with a long duration of diabetes (⩾10 years, n = 771), the PAD in patients with T/T or C/T genotypes was more prevalent at 23.3% (n = 14/60 patients) compared to 12.1% patients with C/C genotype (n = 86/711 patients) (p = 0.015). However, patients with a shorter duration of diabetes and exhibiting PAD were found to have a non-significant difference (p = 0.410) comparing the possessing either T/T or C/T genotypes (7.6% of the population or n = 6/79) versus the C/C genotype (9.2% or n = 89/968) (Supplementary Table S3).
Figure 1 shows univariate and multivariate analyses for the association between TCF7L2 rs7903146 polymorphism and PAD, and the strongest association was observed with PAD in the subgroup with long duration of diabetes (Figure 1). The risk allele (T) TCF7L2 rs7903146 showed a highly significant association with PAD (model 1, unadjusted OR = 2.212, 95% CI = 1.167–4.192, p = 0.015), even after adjustment of age, sex, BMI (model 2, adjusted OR = 2.368, 95% CI = 1.155–4.854, p = 0.019). After further adjustment for presence of familial history of diabetes, smoking habit, laboratory measurements including HbA1c, and lipid profiles (model 3), the results remained unchanged, showing that TCF7L2 T-allele of rs7903146 was strongly associated with PAD (adjusted OR = 2.595, 95% CI = 1.177–5.722, p = 0.018).
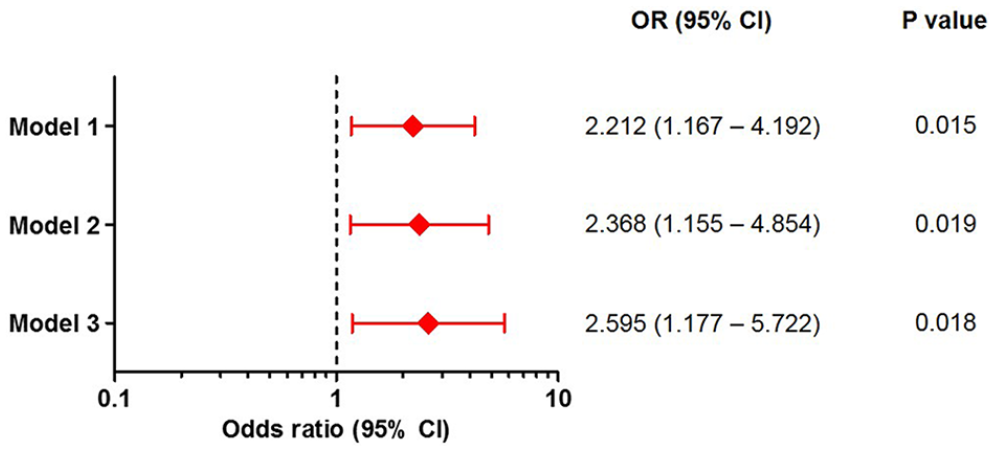
Odds ratio of peripheral arterial disease for TCF7L2 polymorphism rs7903146 for patients with long duration of diabetes (⩾10 years) (n = 771). Data are expressed as ORs and 95% confidence intervals. Multivariate logistic regression models were adjusted for the following covariates: model 1, unadjusted; model 2: age, sex and body mass index; and model 3: adjusted for the same covariates of model 2 plus presence of familial history of diabetes, smoking, glycated haemoglobin, total cholesterol and triglycerides.
Discussion
In this study, we identified that the specific allele variant, rs7903146, from the TCF7L2 gene was significantly associated with PAD in only patients with long-standing diabetes more than 10 years in duration after adjusting well-known cardiometabolic risk factors.
Since a primary clinical feature of PAD shows atherosclerotic change in the mid-to-small arteries, we hypothesized that genetic variation of TCF7L2 gene rs7903146 could be associated with increased risk of PAD in patients with T2D. The TCF7L2 gene is located on chromosome 10 and encodes the transcription factor TCF7L2 protein. 7 This protein can influence the Wnt signalling pathway as a β-catenin transcriptional partner. 5 Several SNPs in the TCF7L2 gene have shown association with increased risk of T2D and gestational diabetes mellitus. 5 Of particular interest in the specific role of TCF7L2 appeared to be involved in the remodelling process of blood vessels. This could be explained by the recent possible mechanism of Wnt signalling pathway regulating vascular smooth muscle cell differentiation. 8 Transcriptional activation of TCF7L2 also activates the nuclear factor-kB signalling pathway, which regulates inflammatory response. 9
According to numerous large-scale genome-wide association studies (GWAS), TCF7L2 was associated with reduced beta-cell function and diabetes has been reported. 10 More importantly, TCF7L2 SNP rs7903146 has been identified as the most significant variant associated with diabetes (40% increased risk of diabetes per allele). 11 In terms of the association between rs7903146 and PAD, the Atherosclerosis Risk in Communities (ARIC) study did not significantly identify an association with the prevalence of PAD. 12 The difference in our findings may likely be due to the heterogeneous population of Black (27.1%) and White (72.9%) patients in the ARIC study compared to a more uniform racial group in this study. In addition to racial differences from our study, TCF7L2 SNP might be difficult to have a clear impact in groups with a population with normal glucose tolerance.
Several limitations of this study could be considered. Study subjects were primarily Korean T2D patients. Because of the genetic differences among ethnicity, future studies will need to examine the importance of racial/ethnic differences with this specific SNP. Second, PAD does not occur at the early stage of diabetes, so it can be challenging to obtain sufficient number of PAD group in patients with a shorter duration of diabetes.
Conclusion
This study indicates that the TCF7L2 SNP, rs7903146, is associated with a higher prevalent PAD in patients with a long duration of T2D. We believe that this additional new information about the genetic association with this specific variant and PAD in patients with long duration of T2D will contribute to a better understanding and development of strategic therapeutic protocols in the treatment of this special population.
Supplemental Material
Supplementary_data – Supplemental material for Genetic variation in TCF7L2 rs7903146 correlating with peripheral arterial disease in long-standing type 2 diabetes
Supplemental material, Supplementary_data for Genetic variation in TCF7L2 rs7903146 correlating with peripheral arterial disease in long-standing type 2 diabetes by Eu Jeong Ku, Gun Woo Won, Yong Hee Lee, Dong-Hwa Lee, Hyun Jeong Jeon and Tae Keun Oh in Diabetes & Vascular Disease Research
Footnotes
Authors’ Note
The part of our data was presented as a poster exhibition at the 55th EASD Annual Meeting of the European Association for the Study of Diabetes. The authors thank the staff and participants of National Biobank of Korea in Chungbuk National University Hospital for their important contributions. The biospecimens for this study were provided by the Chungbuk National University Hospital, a member of the National Biobank of Korea, which is supported by the Ministry of Health, Welfare and Family Affairs. T.K.O. and E.J.K. conceived and designed the study. Y.H.L. and G.W.W. conducted the experiment. T.K.O. conducted all data quality control measures. E.J.K. conducted statistical analyses and drafted the manuscript. T.K.O., E.J.K., H.J.J. and D.-H.L. have contributed discussion of our study findings. All authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: E.J.K. was supported by research grant from the Chungbuk National University Hospital in 2019.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.