
Abstract
Objective:
Glucose dysregulation is an independent risk factor for cardiovascular and neurodegenerative disease development through synaptic dysfunction resulting in cognitive decline. The aim of this study was to study the interplay between impaired glycaemic metabolism (hyperglycaemia and insulin resistance), cardiac stress (cardiac troponin T and N-terminal brain natriuretic peptide) and executive cognitive function prospectively, in a bi-ethnic sex cohort.
Methods:
Black and White teachers (N = 338, aged 20–63 years) from the Sympathetic activity and Ambulatory Blood Pressure in Africans study were monitored over a 3-year period. Fasting blood samples were obtained for cardiac troponin T, N-terminal brain natriuretic peptide, glycated haemoglobin and the homeostatic model assessment-insulin resistance for insulin resistance. The Stroop colour-word conflict test was applied to assess executive cognitive function at baseline.
Results:
Over the 3-year period, Black men revealed constant high levels of cardiac troponin T (⩾4.2 ng/L), pre-diabetes (glycated haemoglobin > 5.7%) and insulin resistance (homeostatic model assessment-insulin resistance >3). %Δ Glycated haemoglobin was associated with %Δ insulin resistance (p < 0.001) and increases in %ΔN-terminal brain natriuretic peptide (p = 0.02) in Black men only. In the latter, baseline Stroop colour-word conflict test was inversely associated with %Δ cardiac troponin T (p = 0.001) and %Δ insulin resistance levels (p = 0.01).
Conclusion:
Progressive myocyte stretch and chronic myocyte injury, coupled with glucose dysregulation, may interfere with processes related to interference control in Black men.
Keywords
Introduction
The importance of blood glucose regulation in cardiovascular disease (CVD) prevention has been emphasized. 1 Hyperglycaemia persists during conditions of chronic stress and vascular injury.2,3 One of the causes of hyperglycaemia, insulin resistance (IR), plays a detrimental role in CVD, as it independently predicts prevalent and incident CVD development. 4 Furthermore, studies also showed that chronic hyperglycaemia [glycosylated haemoglobin (HbA1c) ⩾5.6)] is associated with subclinical myocyte injury. 5
Injury to cardiac myocytes has been identified as a major contributing factor to cardiac dysfunction and failure. 6 Myocyte injury is the main stimulus for the release of cardiac troponin T (cTnT) from the myofibrils in cardiac muscle. 7 An association between cTnT and N-terminal pro-B-type natriuretic peptide (NT-proBNP) was reported in individuals with the metabolic syndrome. 8 In Black men from the Sympathetic activity and Ambulatory Blood Pressure in Africans (SABPA) cohort, cTnT was also associated with NT-proBNP, which may indicate increased cardiac wall strain in our population group. 9
There is increasing evidence to suggest a role of cardiac stress in the development of neurodegenerative diseases as cTnT and NT-proBNP are independently associated with cognitive decline.10,11 Mirza et al. 10 reported that higher NT-proBNP is related to poorer performance in multiple cognitive tests [Stroop colour-word conflict test (STROOP-CWT)], while Gluck et al. 12 showed that the STROOP-CWT was associated with impaired glucose regulation. Furthermore, executive cognitive function, assessed with the STROOP-CWT, differed significantly between individuals with type 2 diabetes and individuals with normal glucose metabolism. 13
The aim of this study was therefore to study the interplay between impaired glycaemic metabolism, cardiac and cognitive function. We assessed the relationship between changes (%Δ) in cardiac stress risk markers (cTnT and NT-proBNP), glycaemic metabolism (HbA1c, IR) and a cognitive test score in a bi-ethnic sex cohort over a 3-year period.
Methods
The SABPA prospective cohort study included urban Black and White teachers from the Dr Kenneth Kaunda Education District of the North West Province of South Africa. 14 This selection was chosen to ensure a similar socio-economic class. 15 From February to May (2008 and 2009), 2170 teachers were invited to participate (Figure 1). Participants aged 20–65 years were assessed for eligibility, with 407 being included in phase I of the study. Phase II of the study was conducted after a period of 3 years from February to May (2011 and 2012). The successful follow-up rate was 87.8% (359 participants; aged 20–63 years). Reasons for non-participation in phase II of the study were pregnancy (N = 2), death (N = 6) and dropouts (N = 42). To avoid bias pertaining to cardio-metabolic risk, participants with an HIV positive status (N = 21) were excluded for the purpose of this study. 15 Ultimately 338 (152 Black and 186 White) participants remained.
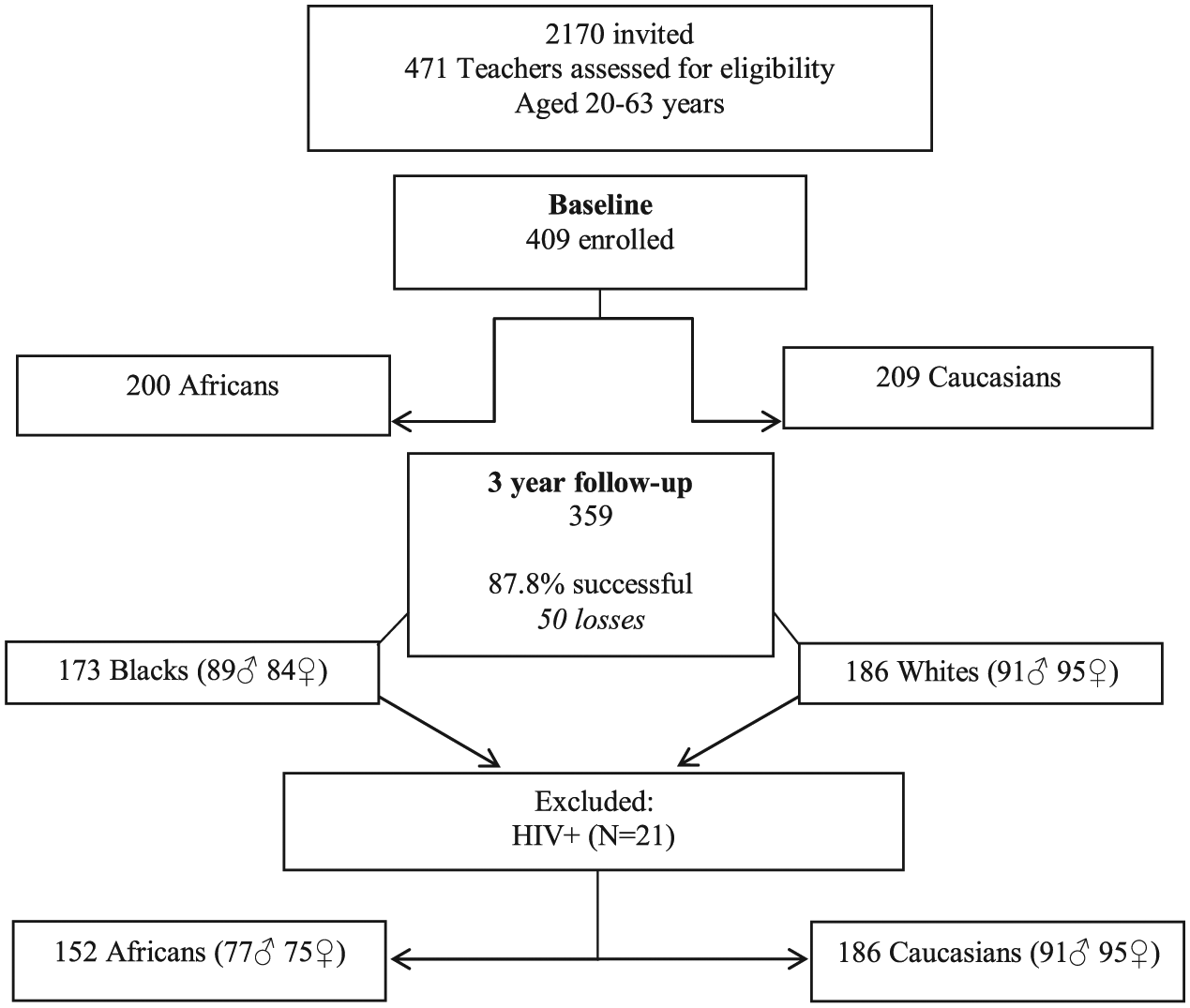
A South African bi-ethnic sex cohort.
Informed consent was obtained from all the participants prior to commencement of the study. The Ethics Review Board of the North-West University, Potchefstroom Campus (NWU-00036-07-S6) gave ethical approval and the study also complied with the Declaration of Helsinki’s ethical guidelines, revised in 2008. 16
Experimental methods and data collection
All clinical assessments were obtained over 48-h. Each participant was connected to the Cardiotens CE120® (Meditech, Budapest, Hungary) apparatus and accelerometers in order to measure 24-h ambulatory blood pressure, electrocardiogram (ECG), as well as 24-h physical activity at approximately 08:00. The correct cuff sizes were applied to the non-dominant arm of each participant. The participants were transported to the Metabolic Unit Research Facility at the North-West University at approximately 16:30 where they were introduced to the experimental set-up. Each participant received his or her own private bedroom and a standardized dinner. Demographic and General Health questionnaires were also completed. The participants were advised to fast and rest from 22:00 for the next day’s clinical measurements.
At approximately 07:30, the following morning, the 24-h ambulatory devices were disconnected where after anthropometric and clinical measurements followed. All resting ECGs, blood sampling and STROOP-CWT measures were obtained after the participants had been in a semi-recumbent position for approximately 30–45 min. Once the assessments were completed, the participants received breakfast and were transported back to their respective schools. Immediate feedback was also provided.
Lifestyle determinants
Registered level II anthropometrists obtained the anthropometric measurements according to standardized procedures. The mean of three measurements was used to ensure accuracy. Inter- and intra-observer variability was found to be less than 10%. The Mosteller formula [weight (kg) × height (cm)/3600]½ was used to calculate the body surface area. Each participant’s daily physical activity was also monitored (Actical® activity monitor; Mini Mitter Co., Inc., Bend, OR, USA; Montreal, QC, Canada).
Biochemical measurements
Fasting blood samples were obtained by registered nurses from the ante-brachial vein utilizing a sterile winged infusion set and handled according to standardized procedures for storage at −80°C until analysis. Gamma-glutamyl transferase (γGT), an indicator of alcohol abuse, was analysed with the enzyme rate method (UniCel DxC 800; Beckman and Coulter, Krefeld, Germany). Serum cotinine, an indicator of nicotine levels, was analysed with the homogeneous immunoassay on Modular ROCHE Automized (Roche, Basel, Switzerland). Serum cTnT and NT-proBNP were analysed with the high-sensitive electrochemiluminescence immunoassay (ECLIA), Elecsys (Roche). In our sample, there were 91 (26.84%) undetectable cTnT values (<3 pg/mL) that were substituted for lower than detectable values. The inter- and intra-batch variability was 15% and 5.6%, respectively, for cTnT and 4.6% and 4.2% for NT-proBNP. An ultrahigh-sensitivity turbidimetric method (UniCel DxC 800; Beckman and Coulter) was used to analyse C-reactive protein. Serum tumour necrosis factor-alpha (TNF-α) was analysed with the Quantikine high-sensitivity human TNF-α enzyme-linked immunosorbent assay [HS ELISA; R&D Systems, Minneapolis, MN, USA]. Despite serum handling within 30 min, the inter- and intra-assay variability for TNF-α was 15% and 17.8%, respectively.
Fasting blood glucose samples were collected in sodium fluoride tubes and analysed with the timed-end-point method (UniCel DxC 800; Beckman Coulter). The turbidimetric inhibition immunoassay was used to determine HbA1c (Integra 400; Roche). Serum insulin was analysed with the ECLIA (Elecsys 2010; Roche) with an intra- and inter-assay precision of 2% and 2.8%, respectively. The homeostatic model assessment (HOMA) was used to indicate IR and was measured using the following formula: fasting glucose × fasting insulin/405. 17
Cardiovascular assessment procedures
As part of the SABPA study design, 24-h BP was measured at 30-min intervals from 08:00 to 22:00 and at 60-min intervals from 22:00 to 06:00. 18 The European Society of Cardiology criteria for hypertension were employed [average 24 h systolic blood pressure (SBP) of ⩾130 mm Hg and/or diastolic blood pressure (DBP) of ⩾80 mm Hg]. 15 The data were analysed with the CardioVisions 1.19 Personal Edition software (Meditech). Participants had to record any abnormalities they experienced throughout the day, on a 24-h diary card. The abnormalities included visual disturbances, headaches, nausea, fainting, palpitations and stress. The Norav NHH-1200® ECG (Norav Medical Ltd, PC 1200, Israel, Software version 5.030) was used to record the resting 10-lead ECG.
Executive cognitive function
Executive cognitive function was assessed by means of the STROOP-CWT. The participants were shown a cardboard containing series of five words in random orders describing a specific colour, but written in different colours. The ink colour of a given word had to be identified verbally. When participants are faced with the task to name the ink colour of a word instead of reading the word, an interference is caused by the more automated task (reading the colour represented by the word).19,20 In order to perform the less automated task, it is therefore required by the participants to inhibit this interference caused by the more automated task.19,20 Participants had to guard against reading the colour represented by the word. They were also encouraged to progress as fast as possible within 1 min and were interrupted to correct wrong answers. An interference score (STROOP-CWT) was calculated that represents the number of correct answers produced during the fixed period of 1 min. A lower score thus indicates that the individual found it more difficult to inhibit the interference. 19 The same two scientists obtained STROOP-CWT scores of teachers at baseline. Participants received a monetary incentive according to their performance on completion of the task.
Statistical analyses
Statistical analyses were performed with Statistica version 13 (TIBCO Software Inc., Palo Alto, CA, USA, 2018). Normal distributions were computed to reveal symmetrical data. Logarithmic transformations were done for variables with skewed distributions. Baseline characteristics of the two ethnic groups were determined with independent t-tests. Chi-square tests (χ2) were used to determine prevalence as well as proportions. Single two-way general linear model interaction on main effects (ethnicity × sex) was computed for all cardiovascular risk markers, independently of a priori defined covariates. 15 Dependent t-tests were used to calculate differences over time in each ethnic group. Percentage changes over time (%Δ) were calculated using the formula: %Δ = (follow-up − baseline)/baseline*100. McNemar’s case–control tests were used to demonstrate changes when participants without diabetes (negative) at baseline become positive at follow-up, and diabetes-positive people at baseline recover to negative at follow-up. Forward stepwise regression analyses determined associations between dependent variables (%∆cTnT, %∆NT-proBNP, %∆HbA1c, %∆HOMA-IR and baseline STROOP-CWT) and independent variables (%∆cTnT, %∆NT-proBNP, %∆HOMA-IR, baseline STROOP-CWT, a priori covariates and TNF-alpha in several separate models. For all of the above-mentioned analyses, significant values were noted when adjusted R2 ⩾ 0.25 and p ⩽ 0.05.
Results
Cross-sectional data analyses
Table 1 depicts the clinical characteristics of the South African bi-ethnic sex cohort at baseline. Blacks had higher γGT, HbA1c, insulin and blood pressure values than Whites. In turn, higher body surface area, physical activity, STROOP-CWT scores and cTnT levels were found in the Whites. More Blacks than Whites showed hyperglycaemia (HbA1c > 5.7%), compatible with a pre-diabetic state (62% vs 31%; p < 0.001).
Clinical characteristics of a South African bi-ethnic sex cohort at baseline.
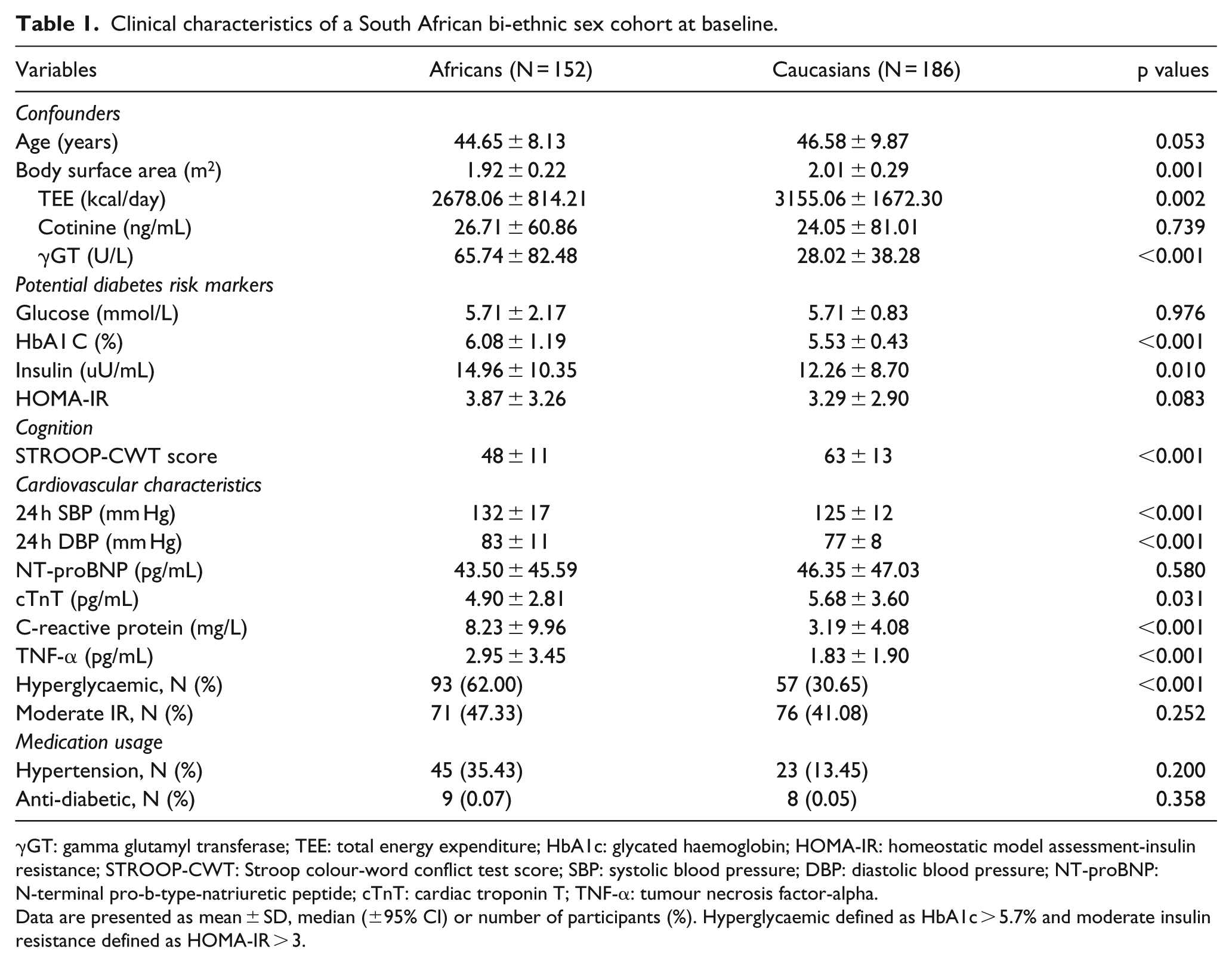
γGT: gamma glutamyl transferase; TEE: total energy expenditure; HbA1c: glycated haemoglobin; HOMA-IR: homeostatic model assessment-insulin resistance; STROOP-CWT: Stroop colour-word conflict test score; SBP: systolic blood pressure; DBP: diastolic blood pressure; NT-proBNP: N-terminal pro-b-type-natriuretic peptide; cTnT: cardiac troponin T; TNF-α: tumour necrosis factor-alpha.
Data are presented as mean ± SD, median (±95% CI) or number of participants (%). Hyperglycaemic defined as HbA1c > 5.7% and moderate insulin resistance defined as HOMA-IR > 3.
Significant interactions with sex were revealed for NT-proBNP [F(1, 316), 8.19, p = 0.005], cTnT [F(1, 322), 12.44, p < 0.001] and with ethnicity for insulin [F(1, 324), 4.40, p = 0.04]. Furthermore, interactions between ethnicity and sex were revealed for cognitive interference [F(1, 324), 97.20, p < 0.001]; [F(1, 324), 21.73, p < 0.001] that motivated further stratification into ethnic–sex groups.
Longitudinal data analyses
A total of 33 participants had incomplete data for the main variables that included HbA1c (N = 8), HOMA-IR (N = 4), cTnT (N = 9), NT-proBNP (N = 11) and STROOP-CWT (N = 1). Participants with incomplete data (N = 33) were, however, included in all analyses as their exclusion did not change the outcome of the results.
Over the 3-year period, insulin and IR decreased, whereas NT-proBNP increased in Blacks and Whites (Supplementary Table S1). In addition, Whites revealed decreases in cTnT and glucose. In Black men, ∆NT-proBNP increased over the 3-year period, whereas no significant % changes (%∆) were revealed for cTnT, HbA1c and IR (Table 2). In Black men, incidence of diabetes changed significantly over the 3-year follow-up period [%Δ 7.36 (odds ratio (OR) 0.1 (0.01, 0.78)), p = 0.007]. Here, 10 participants developed diabetes over the 3-year period, with only 1 participant recovering from baseline to follow-up.
Unadjusted differences over a period of 3-years in Black men.
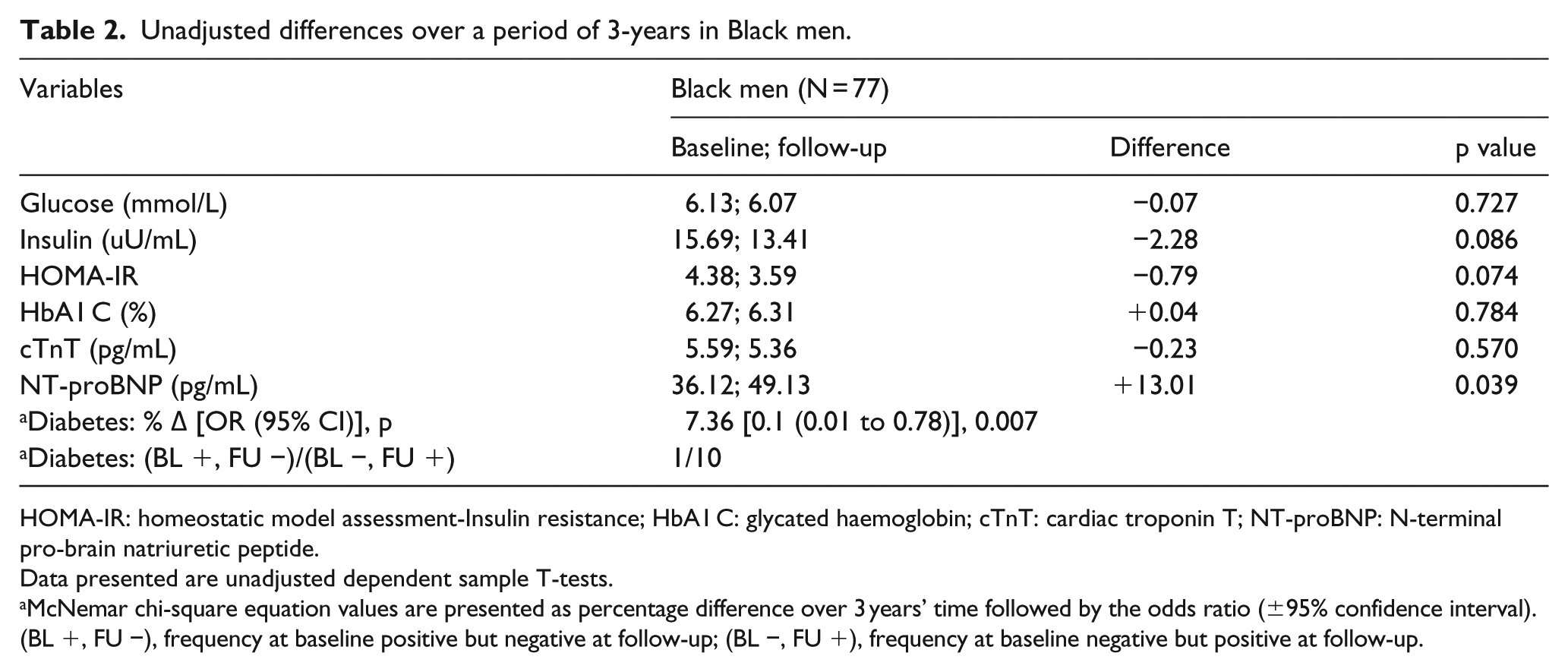
HOMA-IR: homeostatic model assessment-Insulin resistance; HbA1 C: glycated haemoglobin; cTnT: cardiac troponin T; NT-proBNP: N-terminal pro-brain natriuretic peptide.
Data presented are unadjusted dependent sample T-tests.
McNemar chi-square equation values are presented as percentage difference over 3 years’ time followed by the odds ratio (±95% confidence interval). (BL +, FU −), frequency at baseline positive but negative at follow-up; (BL −, FU +), frequency at baseline negative but positive at follow-up.
Forward stepwise regression analyses determined associations between changes (%Δ) in cardiac stress markers (NT-proBNP and cTnT), STROOP-CWT, IR and HbA1c over a 3-year period. No associations were evident in women (of either ethnicity) and in White men; therefore, we will only report associations found in Black men as shown in Table 3. In Black men, constant high HbA1c (>5.7%) was associated with constant high IR (HOMA-IR > 3) [adj R2 = 0.28, β = 0.43; 95% confidence interval (CI) 0.22 to 0.64; p < 0.001] as well as increases in %ΔNT-proBNP (adj R2 = 0.28, β = 0.26; 95% CI 0.05 to 0.48; p = 0.02). Also in Black men, baseline STROOP-CWT score was inversely associated with constant high cTnT (>4.2 ng/mL) (adj R2 = 0.24, β = −0.36; 95% CI −0.57 to −0.15; p = 0.001) and constant high IR (adj R2 = 0.24, β = −0.28; 95% CI −0.49 to −0.06; p = 0.01).
Independent associations between cardiac stress markers, insulin resistance and cognitive interference scores in a Black male cohort.
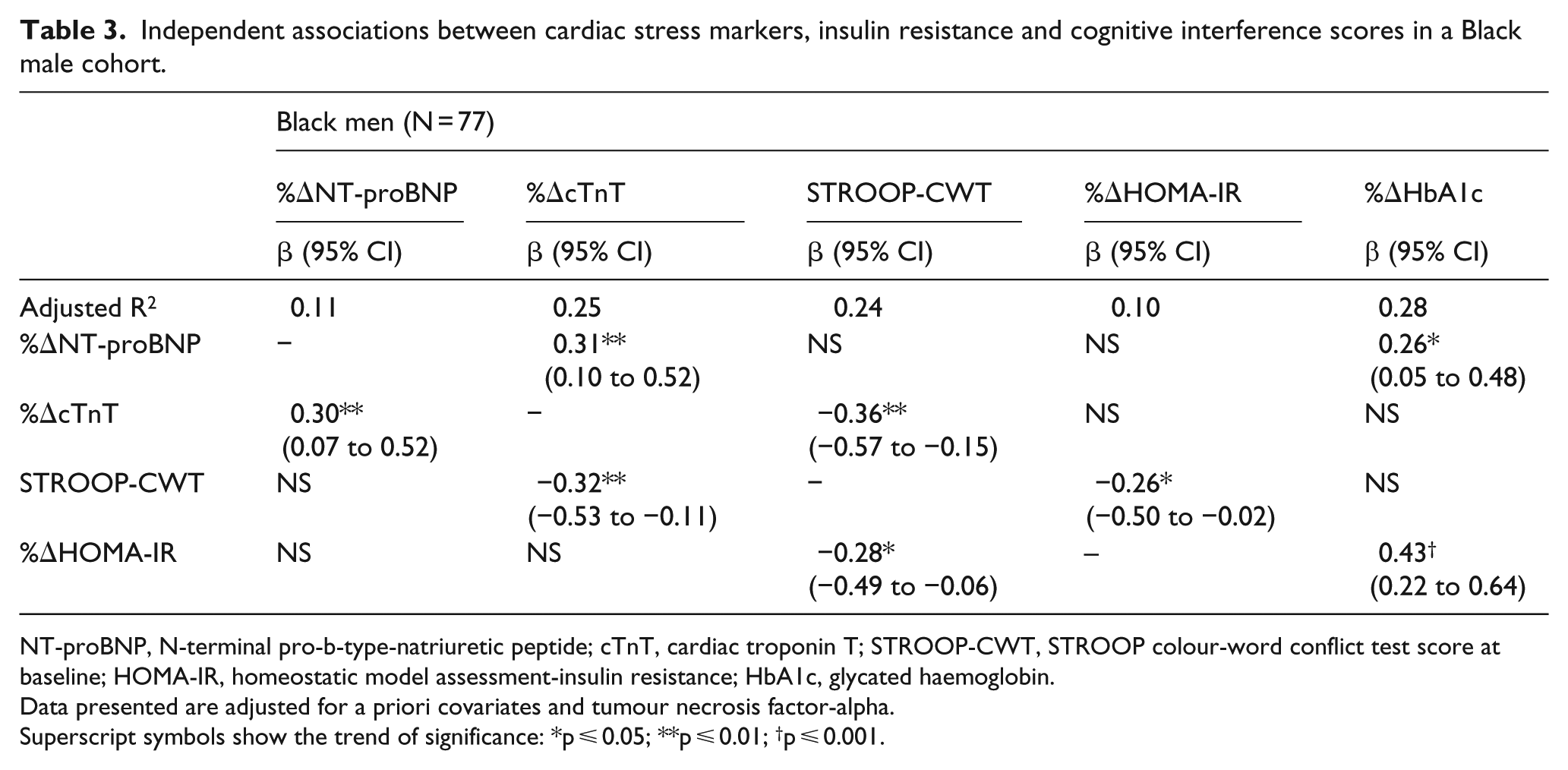
NT-proBNP, N-terminal pro-b-type-natriuretic peptide; cTnT, cardiac troponin T; STROOP-CWT, STROOP colour-word conflict test score at baseline; HOMA-IR, homeostatic model assessment-insulin resistance; HbA1c, glycated haemoglobin.
Data presented are adjusted for a priori covariates and tumour necrosis factor-alpha.
Superscript symbols show the trend of significance: *p ⩽ 0.05; **p ⩽ 0.01; †p ⩽ 0.001.
Discussion
The aim of this study was to determine whether changes in markers of cardiac stress were associated with changes in IR, hyperglycaemia and a cognitive test score in a bi-ethnic male and female cohort. Over a 3-year period, cardiac stress (NT-proBNP and cTnT) was associated with dysregulated glucose metabolism (IR and hyperglycaemia) that may interfere with the ability to inhibit cognitive interference.
Executive cognitive function, cardiomyocyte injury and glucose metabolism
In this study, Blacks revealed a lower STROOP-CWT score than Whites indicating that Blacks had more difficulty to inhibit cognitive interference than Whites. One of many reasons why Blacks revealed lower STROOP-CWT scores than Whites might be explained by the inverse association found between STROOP-CWT with constant high (⩾4.2 ng/L) cTnT levels 21 in this study, as higher cTnT might lead to subclinical cerebral injury expressed as silent brain infarcts and white matter lesions on magnetic resonance imaging. 22 Wijsman et al. 23 reported that participants with higher hs-cTnT levels had steeper STROOP-CWT declines over a period of 3.2 years. Indeed, in Black men high levels of cTnT > 4.2 ng/L indicative of ischaemic heart disease risk 24 was sustained and associated with reduced cardiac output, 25 possibly leading to cerebral hypoperfusion resulting in executive functional decline. 21
Other factors may also influence cognitive interference scores such as neural activation 26 rather than increased cerebral perfusion in low-level alcohol users when compared with non-users. 27 As alcohol use increases, the difficulty score pertaining to the STROOP-CWT increases 28 indicating that high levels of alcohol abuse 29 and neural activity 23 previously described in the Black cohort should be considered for the lower cognitive interference scores evident in the Blacks.
Cognitive interference was also inversely associated with IR in the current Black male cohort. Studies have shown IR to be associated with memory impairments and atrophy of brain regions leading to cognitive deficits. 30 Usually, atrophy of these brain regions occur in early-onset Alzheimer’s disease (AD). 30 Indeed, individuals with diagnosed AD showed reduced resistance to cognitive interference 31 and hypo-activation of brain areas involved in this inhibitory control. 32 The exact mechanism of how peripheral IR affects cognitive inhibitory control is, however, unclear. Numerous mechanisms leading to impaired cognition may apply including excessive amyloid beta accumulation and tau hyper-phosphorylation. 33 Therefore, regulation of blood glucose and correction of IR in a clinical setting may be of crucial importance for improved cognitive control and health.
Dysregulated glucose and myocyte stretch
IR has been reported in Black women of South Africa before. 34 We expand current findings by showing moderate IR (HOMA-IR >3, <5) 35 also in Black men. Different cellular mechanisms may be involved in the pathogenesis of IR that includes inflammation. 36 The Insulin Resistance Atherosclerosis Study reported associations between the inflammatory marker, TNF-α with higher glucose levels and IR. 37 However, statistical adjustments of TNF-α in our study indicated that moderate IR was evident in Black men, independent of inflammation.
The association found between hyperglycaemia and IR in our Black male/female cohort may underscore their pre-diabetic state (HbA1c > 5.7%), 35 as previously reported by Lammertyn et al. 38 Insulin is responsible for the regulation of metabolism as it promotes glycogen synthesis and glucose uptake into the cells while inhibiting glucose release into the circulation. 36 With IR, the tissues thus show reduced sensitivity to insulin-mediated biological activity. 36 This results in a disrupted balance between glucose uptake and release into the circulation leading to excessive glucose accumulation in blood vessels.2,3
Again, increased neural activity or depressed heart rate variability in the SABPA Black cohort, particularly men,23,39 might be one mechanism to explain the chronic hyperglycaemia. Indeed, non-dipping Black men revealed higher HbA1c values, and associations were demonstrated between chronically elevated blood glucose and a blunted nocturnal blood pressure dipping. 38 The latter is indicative of autonomic dysfunction and volume overload. 40 NT-proBNP is a valuable marker to assess volume overload as it is released in response to myocyte stretch along with BNP that may lead to sympathetic nervous system inhibition, as well as the induction of natriuresis and diuresis. 41 In this study, we saw that constant elevated cTnT and HbA1c levels were associated with increases in NT-proBNP. Other studies reported an association between chronic hyperglycaemia and subclinical myocardial injury, as indicated by increased cTnT levels. 5 We cautiously suggest that progressive increases in NT-proBNP may act as compensatory protective mechanism against chronic hyperglycaemia and cardiomyocyte injury in the current Black male cohort over a 3-year period.
Limitations and conclusion
Although this study is the first to present associations between cardiac stress, hyperglycaemia, IR and cognitive interference in Blacks, there are limitations. The results cannot be attributed to the African population at large as participants consisted of a small prospective cohort in South Africa. We did not perform a mechanistic study, so even plausible inferences about the interplay of discussed relationships must remain speculative. The clinical relevance of our findings needs to be shown beyond a 3-year observation period.
In conclusion, as depicted in Figure 2, we propose that progression of mycocyte stretch is associated with chronic myocyte injury and hyperglycaemia in Black men. Furthermore, hyperglycaemia is associated with IR that may interfere with the inhibition of cognitive interference in these men. Therefore, in Black men, progressive myocyte stretch and chronic myocyte injury, coupled with dysregulation of glucose metabolism, may interfere with processes related to interference control.
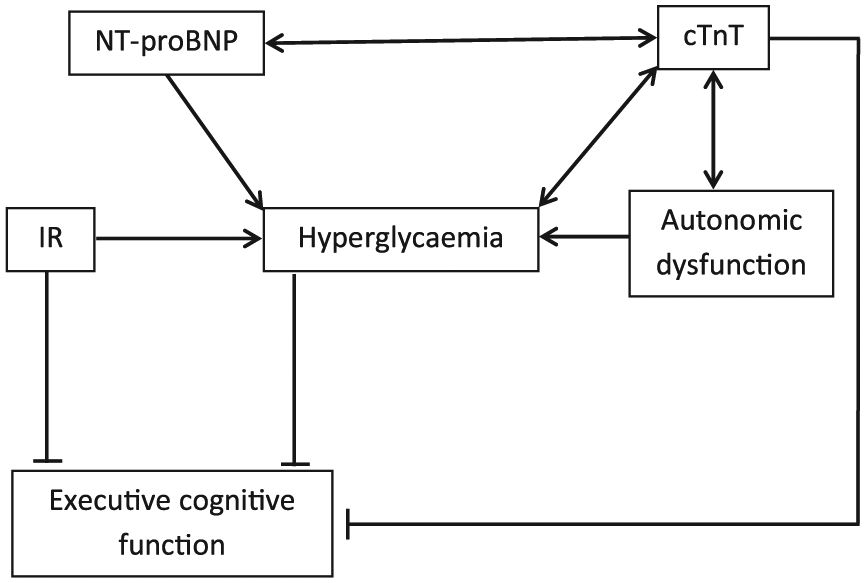
Proposed mechanism of cardiac stress markers and glucose dysregulation associating with executive cognitive function in Black men.
Key messages
This longitudinal study is the first to assess the associations between glucose dysregulation, myocardial stress and injury as well as executive cognitive function in a South African cohort.
In Black men, chronic hyperglycaemia raised HbA1c levels was associated with NT-proBNP upregulation and moderate insulin resistance over a 3-year period.
Executive cognitive function was also inversely associated with moderate insulin resistance and chronic raised cTnT levels in Black men.
Progressive myocyte stretch and chronic myocyte injury, coupled with glucose dysregulation, may interfere with processes related to interference control in Black men.
Supplemental Material
dvdres-sep-2018-00172-File007 – Supplemental material for Prospective associations between cardiac stress, glucose dysregulation and executive cognitive function in Black men: The Sympathetic activity and Ambulatory Blood Pressure in Africans study
Supplemental material, dvdres-sep-2018-00172-File007 for Prospective associations between cardiac stress, glucose dysregulation and executive cognitive function in Black men: The Sympathetic activity and Ambulatory Blood Pressure in Africans study by Esmé Jansen van Vuren, Leoné Malan, Roland von Känel, Martin Magnusson, Leandi Lammertyn and Nicolaas T Malan in Diabetes & Vascular Disease Research
Footnotes
Acknowledgements
The authors would like to thank all the individuals who volunteered to participate in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was financially supported by the following institutions: North West University, Potchefstroom, South Africa; National Research Foundation (NRF); South African Medical Research Council (MRC); Department of Education, North West Province, South Africa; Roche Diagnostics; Metabolic Syndrome Institute, France. Any opinion, findings and conclusions or recommendations expressed in this material are those of the author(s) and therefore funders do not accept any liability in regard thereto.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.