
Abstract
Background:
The number of patients with type 2 diabetes mellitus and diabetes mellitus–associated chronic kidney disease varies considerably between countries. Next to differences in genetic as well as life style risk factors, varying practices in medical care delivery might cause this diversity.
Method:
The PROVALID study recruited 4000 patients with type 2 diabetes mellitus at the primary level of healthcare in five European countries (Austria, Hungary, The Netherlands, Poland and Scotland). Baseline data were used to describe patient characteristics and compare the adherence to ADA (American Diabetes Association) and KDIGO (Kidney Disease: Improving Global Outcomes) guidelines with respect to metabolic and blood pressure control, use of renin–angiotensin system–blocking agents, statins and acetylsalicylic acid between the countries.
Results:
About 34.8% of the population had evidence of diabetes mellitus–associated chronic kidney disease. The median HbA1c level of the cohort was 6.8% (ranging from 6.5 in Poland to 7.0% in Scotland). Mean blood pressure was 136/79 (±17/10) and significantly higher in subjects with elevated albuminuria. These individuals also were more often treated with renin–angiotensin system–blocking agents (74.1% vs 84.6%), whereas the use of statins was driven by cardiovascular comorbidity. Acetylsalicylic acid was used in only 28.9% subjects. Despite similar cardiovascular comorbidities and renal function, the use of renin–angiotensin system–blocking agents varied significantly between the countries from 66.7% to 87.4%. An even higher variability was observed for patients >40 years of age using statins (39.8%–82.7%) and administration of acetylsalicylic acid in patients older than 50 years (5.2%–43.8%).
Conclusion:
Our study shows that medical practice in type 2 diabetes mellitus patients with and without renal disease is different in European countries. Longitudinal follow-up will reveal if this diversity affects clinical endpoints.
Background
The Global Burden of Disease Study ranked chronic kidney disease (CKD) 19th on the list of all causes of mortality 1 and the age-standardized death rate due to renal failure increased from 11.6 to 15.8/100,000 between 1990 and 2013. Diabetes mellitus–associated CKD (DKD) is a major contributor and the number of diabetic patients with end-stage renal disease (ESRD) in Europe is expected to rise annually by 3.2% at least until the year 2025. 2 Next to issues directly related to renal replacement therapy (RRT), comorbidities (like premature cardiovascular events, increased incidence of fractures, cognitive impairment, and anaemia) make DKD not only an important global health but also socio-economical problem.3,4
In order to support clinical decision-making and healthcare policy planning, it is important to understand the epidemiology of CKD and identify factors associated with its incidence and progression, ideally not only in but also outside the setting of randomized controlled trials. Kramer at al. 5 analysed the 2013 EDTA-ERA registry data on incident patients to RRT. On average, DKD was listed as the cause of ESRD in 24% (26 pmp), but interestingly the differences between countries were remarkable (from 6 in the Ukraine and 12 pmp in Iceland to 58 and 70 pmp in Greece and Portugal). Regional variability was observed also in non-dialysis-dependent CKD in Europe, 6 the United States 7 and China. 8 Next to heterogeneities in study design, inclusion and/or exclusion criteria or laboratory methodology used for creatinine measurement, 9 genetic background driven disease susceptibility as well as dietary habits can affect serum creatinine values and/or incidence or progression of the disease. Regional differences in risk factors like smoking, physical activity, socioeconomic status and birth weight also have to be considered. As far as initiation of RRT is concerned, patterns of referral to dialysis and/or transplantation may vary and finally local healthcare policies and/or clinical practice pattern (e.g. metabolic or blood pressure control) also might influence CKD/DKD incidence, prevalence and progression.
In order to assess the latter, we analysed baseline data from the PROVALID (PROspective cohort study in patients with T2DM for VALIDation of biomarkers) study, a prospective cohort study that recruited subjects with T2DM at the primary level of healthcare in Austria, Hungary, Poland, Scotland and The Netherlands. The aim of our study was to describe whether the presence or absence of renal disease as defined by the KDIGO (Kidney Disease: Improving Global Outcomes) stages 10 affects major aspects of treatment in the total population and in the different participating countries. As a measure, we used the adherence pattern to ADA (American Diabetes Association) and KDIGO treatment guideline recommendations for metabolic, blood pressure and low-density lipoprotein (LDL) cholesterol (LDL-C) control as well as administration of aspirin.11–13
Methods
Study design
A detailed description of the PROVALID study is presented elsewhere. 14 In summary, PROVALID is a prospective cohort study of 4000 individuals with incident or prevalent T2DM (defined either as treatment with hypoglycaemic drugs or according to ADA guidelines). Subjects older than 18 years were recruited at the primary level of healthcare in five European countries (629 patients in Austria, 1420 in Hungary, 903 in The Netherlands, 537 in Poland and 511 in Scotland) and only those with active malignancy (defined as those currently receiving chemotherapy) or who declined to participate were excluded. Details on the recruitment procedure are described in the work by Eder et al. 14 This article uses individual patient data obtained at the time of recruitment into the study (2011–2015). According to the KDIGO classification system 10 DKD was considered absent in subjects with stages G1 and G2 [estimated glomerular filtration rate (eGFR) ≥60 mL/min/1.73 m2] and urinary albumin excretion <30 mg/g creatinine (A1, formerly called normoalbuminuria) in a morning spot urine sample.
Statistical analysis
Data are presented as mean ± SD, median and interquartile range or percentage as appropriate. Data adjusted for age, gender and diabetes duration were calculated by univariate linear regression. Comparisons between groups were performed using Student’s t test or one-way analysis of variance (ANOVA) followed by Bonferroni post hoc test, Mann–Whitney test, Kruskal–Wallis test or χ2 test as appropriate. Missing values were not included for any calculations. All statistics were done in IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp., Armonk, NY, USA).
Results
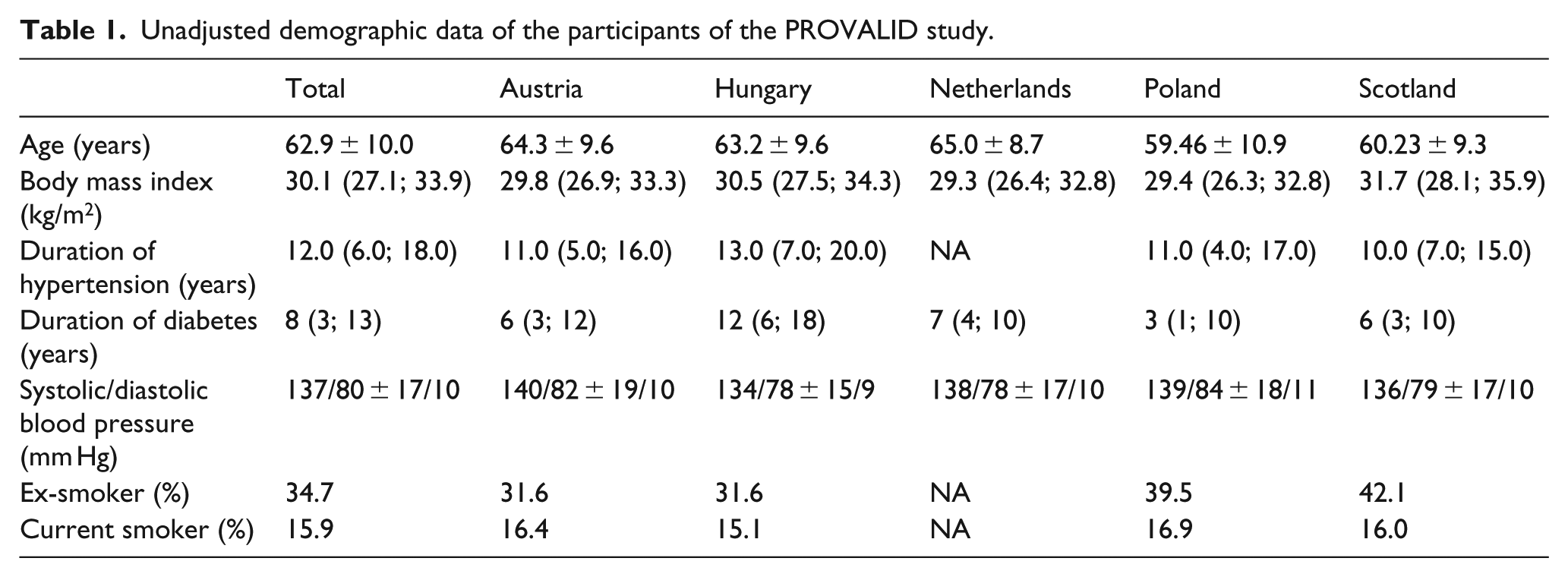
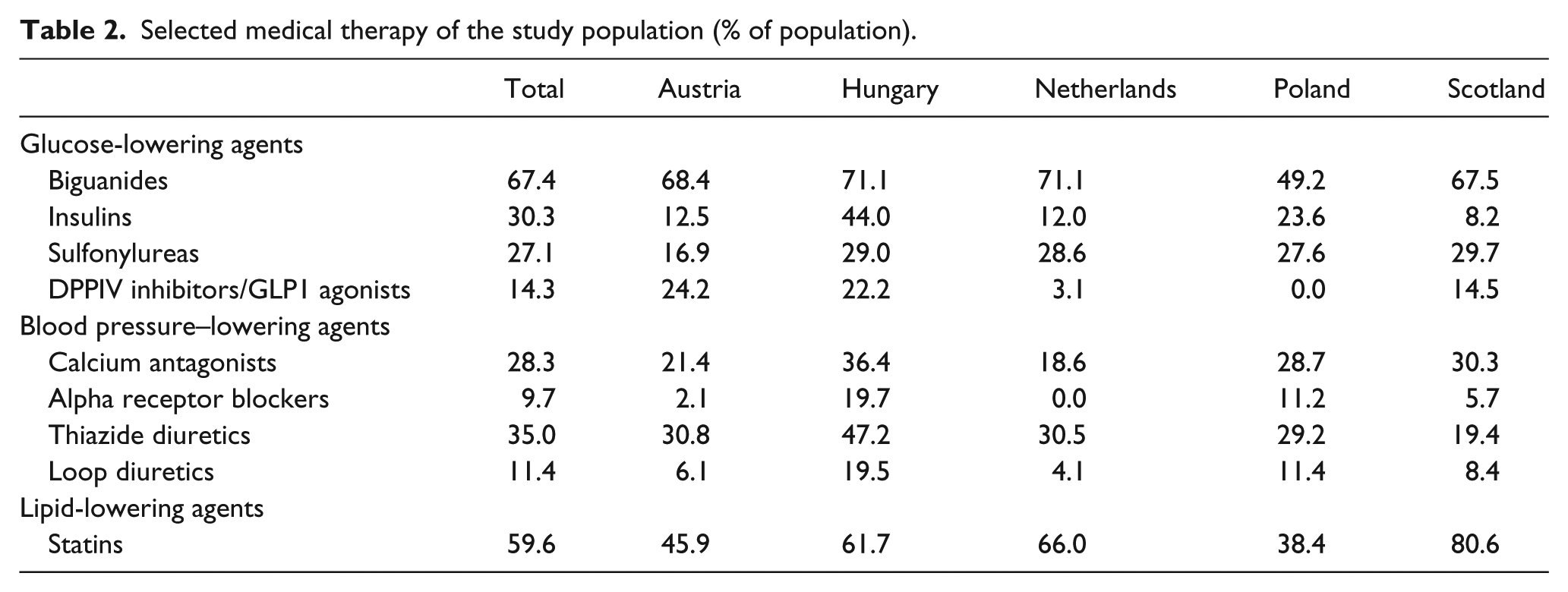
General and country-specific unadjusted demographic data are provided in Table 1, and Table 2 shows details on medical therapy not discussed in the article elsewhere. For further information, refer to the work by Eder et al. 14
Unadjusted demographic data of the participants of the PROVALID study.
Selected medical therapy of the study population (% of population).
Prevalence of CKD and cardiovascular comorbidities
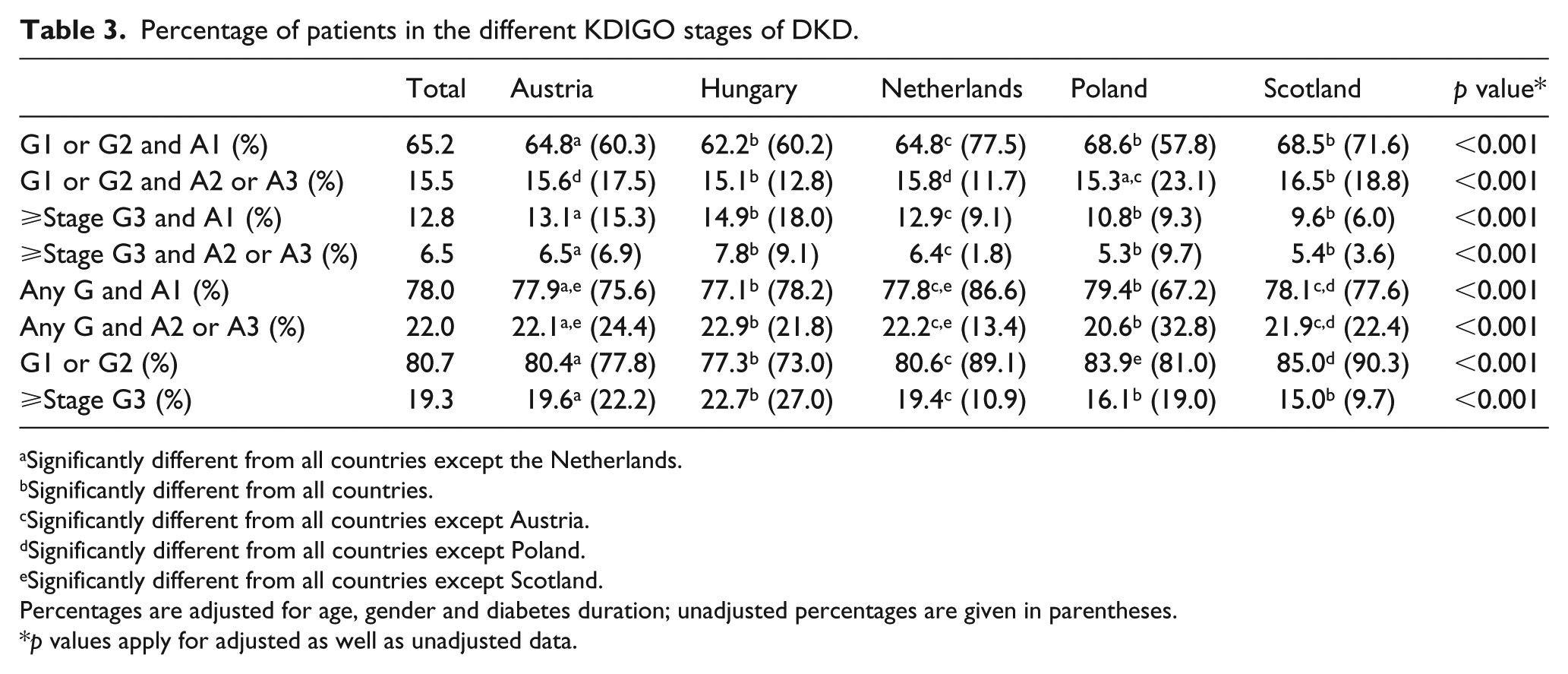
The percentage of patients in the different KDIGO stages of DKD (unadjusted as well as adjusted for age, gender and diabetes duration) in the total study population as well as the national sub-cohorts is given in Table 3.
Percentage of patients in the different KDIGO stages of DKD.
Significantly different from all countries except the Netherlands.
Significantly different from all countries.
Significantly different from all countries except Austria.
Significantly different from all countries except Poland.
Significantly different from all countries except Scotland.
Percentages are adjusted for age, gender and diabetes duration; unadjusted percentages are given in parentheses.
p values apply for adjusted as well as unadjusted data.
Even though the adjusted as well as unadjusted percentages of KDIGO stages differed statistically significantly between the countries, the populations were similar based on clinical judgement. About two-thirds of the subjects had normal renal function, 15% had maintained eGFR ≥60 mL/min/1.73 m2 but at least moderately increased albuminuria (stages A2 and A3, former micro- and macroalbuminuria). In approximately 20%, eGFR was decreased <60 mL/min/1.73 m2 (G3 or higher) and in this subgroup two-thirds were in albuminuria stage A1 and only 8% presented with a urinary albumin excretion >300 mg/g creatinine.
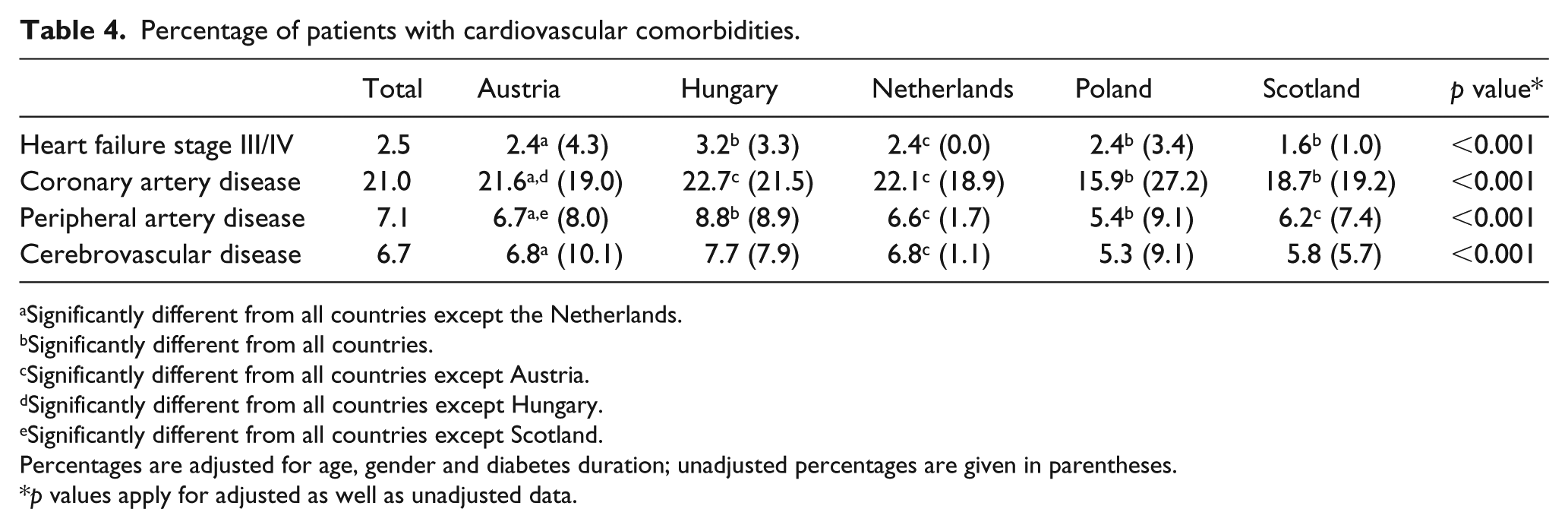
The percentage of patients with cardiovascular comorbidities in the total study population and the national sub-cohorts adjusted for age, gender and diabetes duration is presented in Table 4. The proportions in parentheses indicate the unadjusted cardiovascular comorbidity prevalence. The prevalence of comorbidities also differed significantly between the countries but in absolute terms these variations were small with some exceptions (e.g. less age, gender and diabetes duration adjusted coronary artery disease in the populations in Poland and Scotland). Supplementary Table 1 provides information on the prevalence of comorbidities in patients with normal renal function and those with CKD. Even though the latter were younger, their cardiovascular disease burden was significantly higher.
Percentage of patients with cardiovascular comorbidities.
Significantly different from all countries except the Netherlands.
Significantly different from all countries.
Significantly different from all countries except Austria.
Significantly different from all countries except Hungary.
Significantly different from all countries except Scotland.
Percentages are adjusted for age, gender and diabetes duration; unadjusted percentages are given in parentheses.
p values apply for adjusted as well as unadjusted data.
Metabolic control
The KDIGO guidelines recommend a target HbA1c value of 7% to prevent or delay progression of microvascular complications of diabetes including DKD. In individuals with comorbidities or limited life expectancy, the goal should be extended to >7%, whereas in those at risk for hypoglycaemia, HbA1c levels should not be below 7%10. The ADA11 recommends an HbA1c level around 7% for all T2DM patients except pregnant women but with individualization according to a number of factors. In those with a short disease duration, treatment with lifestyle measures or metformin only, a long life expectancy or no significant cardiovascular comorbidity the goal can be set for <6.5%. On the contrary, those with a risk for hypoglycaemia, advanced micro- or macrovascular disease-extensive comorbidities or long-standing diabetes might aim for <8%. Table 5 shows data on the median HbA1c levels and Table 6 shows the percentage of patients within specific ranges in the total study population and the national sub-cohorts. In all countries except Scotland, more than 80% of subjects included had an HbA1c of <8% suggesting that in general metabolic control was acceptable in the majority of patients.
Median HbA1c levels and the percentage of patients within specific ranges.
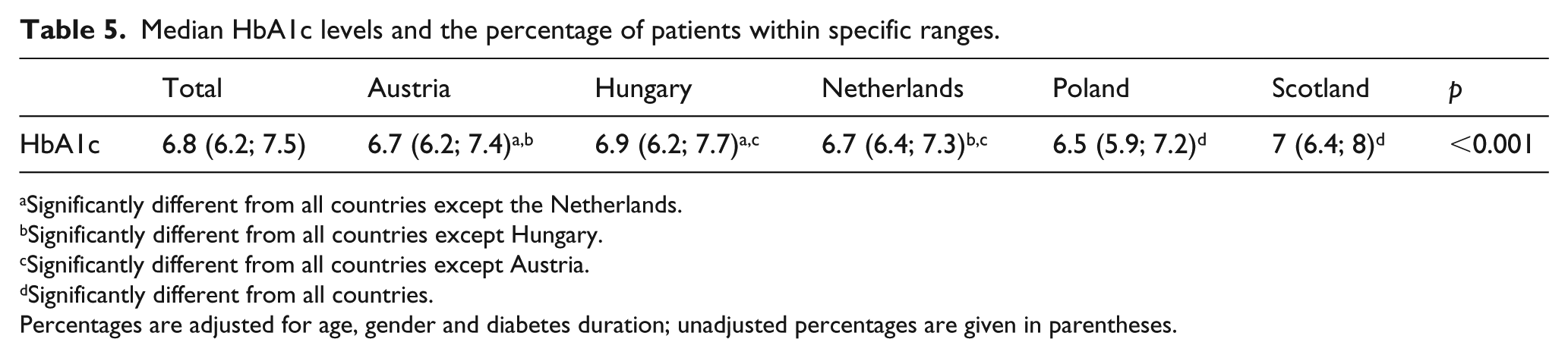
Significantly different from all countries except the Netherlands.
Significantly different from all countries except Hungary.
Significantly different from all countries except Austria.
Significantly different from all countries.
Percentages are adjusted for age, gender and diabetes duration; unadjusted percentages are given in parentheses.
Percentage of patients within specific ranges of HbA1c levels. Analysis done be Chi-square test, no poshoc analysis available.
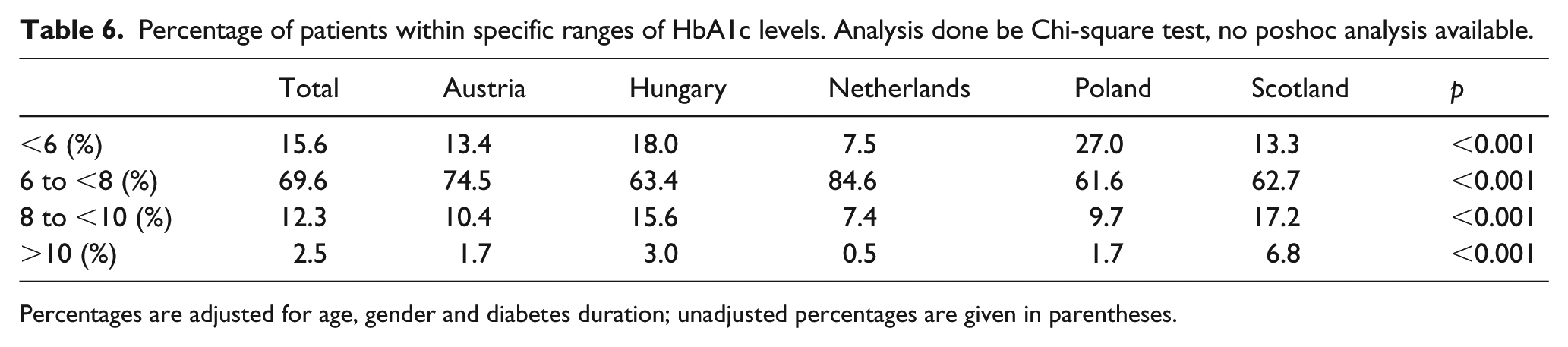
Percentages are adjusted for age, gender and diabetes duration; unadjusted percentages are given in parentheses.
Blood pressure control
Both KDIGO 10 and the ADA guidelines 12 recommend that blood pressure in patients with T2DM and urinary albumin excretion below 30 mg/day should not exceed 140/90 mm Hg. In subjects with an elevated urinary albumin excretion (A2 and A3), the goal blood pressure is reduced to 130/80. Table 7 shows the mean blood pressure values for the various groups and Table 8 shows the percentage of subjects within these recommendations in the total study population and in the various national sub-cohorts. Whereas about 75% of subjects reached goal blood pressure in diabetic patients with normal or mildly increased albuminuria (A1), blood pressure was <130/80 mm Hg in only 10%–20% of patients with higher urinary albumin excretion. Interestingly these patients not only reached goal blood pressure values less often but even had higher mean systolic blood pressure in all countries expect Poland when compared to normoalbuminuric study participants. Worse blood pressure control was achieved in patients in stages A2 and A3 when compared to A1 despite the fact that antihypertensive therapy was intensified (see Supplementary Table 2). Further analysis revealed that worse blood pressure control was observed in all countries expect Poland in patients at early stages (G1 and G2) of renal disease and at least moderately increased albuminuria (A2 and A3) (Supplementary Table 3) but not in subjects with more advanced renal failure.
Mean blood pressure values.
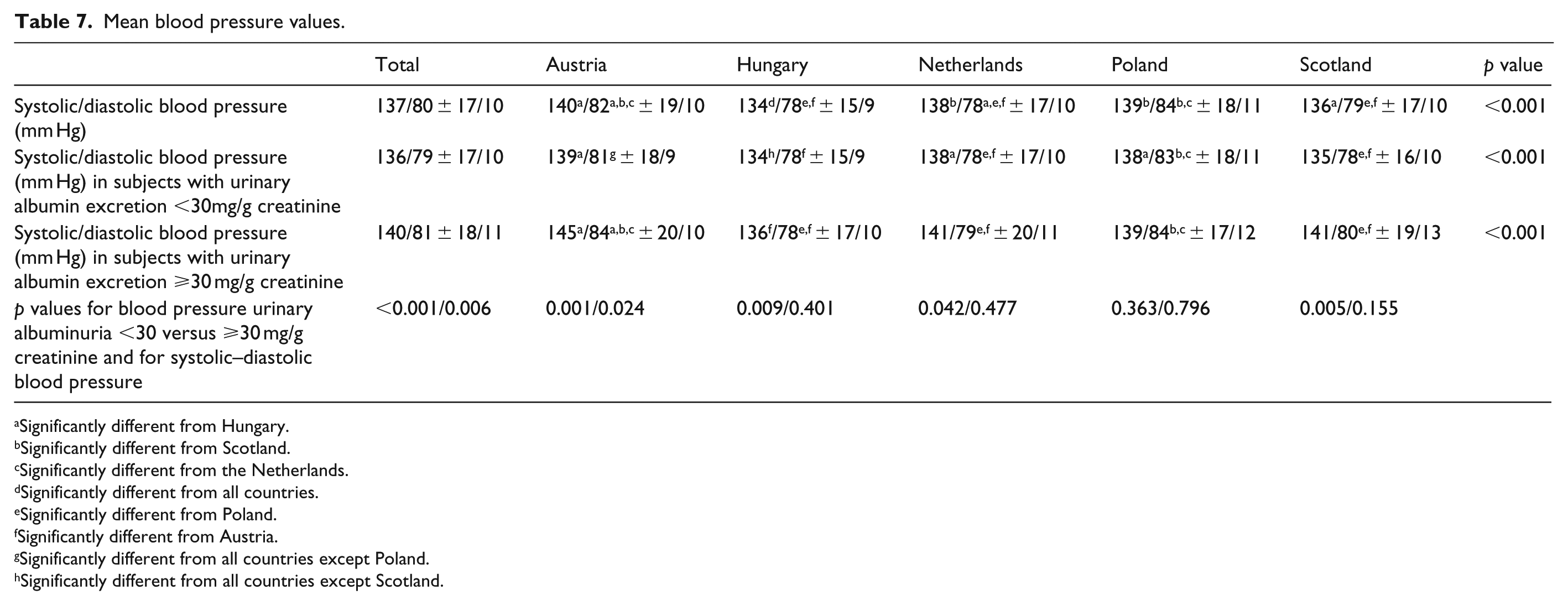
Significantly different from Hungary.
Significantly different from Scotland.
Significantly different from the Netherlands.
Significantly different from all countries.
Significantly different from Poland.
Significantly different from Austria.
Significantly different from all countries except Poland.
Significantly different from all countries except Scotland.
Percentage of subjects reaching recommended blood pressure goal levels.

Prescription of agents blocking the renin–angiotensin–aldosterone system, statins and aspirin
Both KDIGO 10 and the ADA 12 recommend ACE inhibitor or angiotensin receptor blocker (ARB) therapy in patients with T2DM and albuminuria >30 mg/g creatinine. Table 9 shows the percentage of subjects treated with these agents in the total study population and in the national subpopulations according to their albuminuria status.
Use of agents that block the renin–angiotensin system.
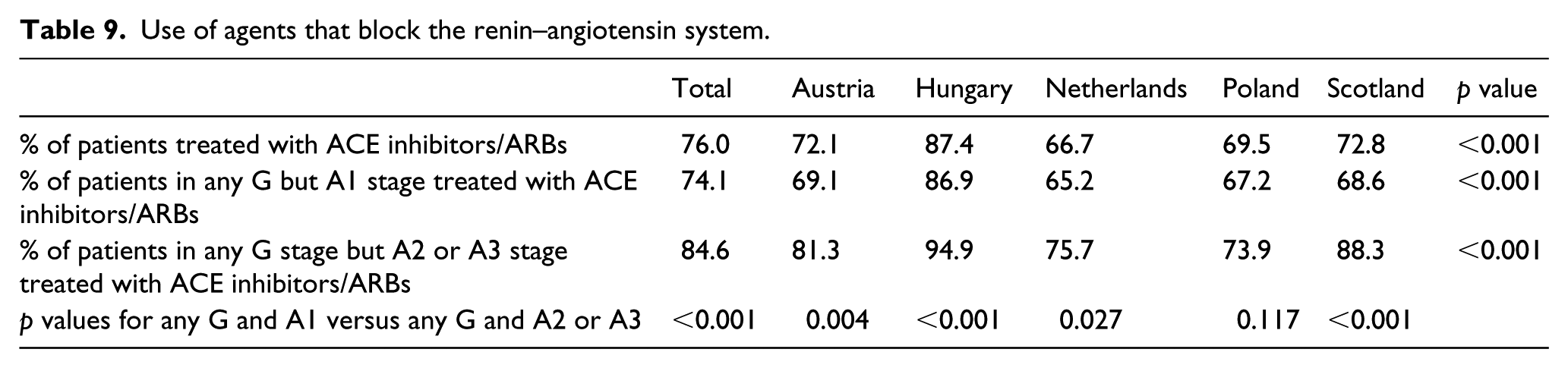
About three-quarters of all subjects included received RAS blocking therapy (66.7%–87.4%). The use of the agents was significantly higher in patients with KDIGO stages A2 and A3 in all countries expect in Poland. In addition, patients with KDIGO stages G3 or higher were also preferentially treated by RAS blockade (with the exception of expect for Poland and The Netherlands; Supplementary Table 4a). A more detailed analysis of RAS blocking therapy according to different KDIGO classification groups is provided in Supplementary Table 4b. RAS blocking therapy was more prevalent in subjects in stages A2 or A3 in G 1 and 2 stages of the disease. The same trend could not be observed in more advanced G stages, if anything the frequency of administration was lower in the presence of moderately or severely increased albuminuria. Additional analysis of this subgroup showed that normoalbuminuric patients with eGFR values below 60 mL/min/1.73 m2 had higher mean eGFR but lower blood pressure than their albuminuric counterparts [50.8 mL/min/1.73 m2, interquartile range (IQR) 42.4–55.2 vs 44.0 mL/min/1.73 m2, IQR 32.8–57.4; p < 0.001; 136/77 ± 17/10 vs 138/79 ± 18/11; p = 0.09/0.01]. In addition, the serum potassium levels were identical (4.5 mmol/L, IQR 4.2–4.8 vs 4.5 mmol/L, IQR 4.1–5.0; p = 0.277). Thus, based on these cross-sectional data, we cannot explain the lower use of ACE/ARB therapy in patients with advanced renal disease and moderately or severely increased albuminuria. It could be speculated that some initially albuminuric subjects had regressed to normoalbuminuria but stayed on RAS blocking therapy.
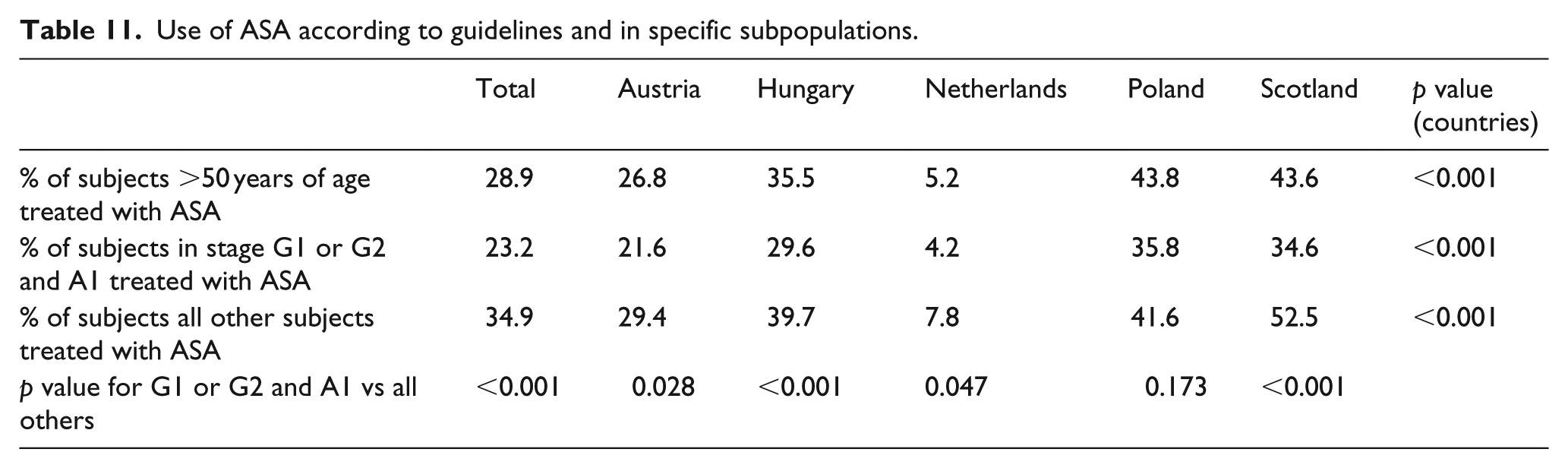
As far as cholesterol-lowering therapy is concerned, the ADA guidelines recommend that all diabetic patients over the age of 40 should receive a statin 12 . KDIGO suggests statin therapy for all patients with CKD 10 . Table 10 and Supplementary Table 5 show details on adherence to these guidelines. In Table 11, the use of aspirin is given, which is recommended for all diabetic patients >50 years of age by the ADA 13 and for all subjects with CKD by KDIGO. 10 Supplementary Table 6 shows more details on the use of ASA according to guidelines and on serum cholesterol levels, which were significantly different between the countries. A total of 3902 subjects were older than 40 years and thus generally eligible for statin therapy according to the ADA guidelines. In countries with high use of statins, the presence of renal disease did not affect statin prescription frequency. However, in the two countries with less than 50 statin use in general (Austria and Poland), subjects with renal disease were more likely to be prescribed statin therapy.
Serum cholesterol levels and use of statins according to guidelines and in specific subpopulations.
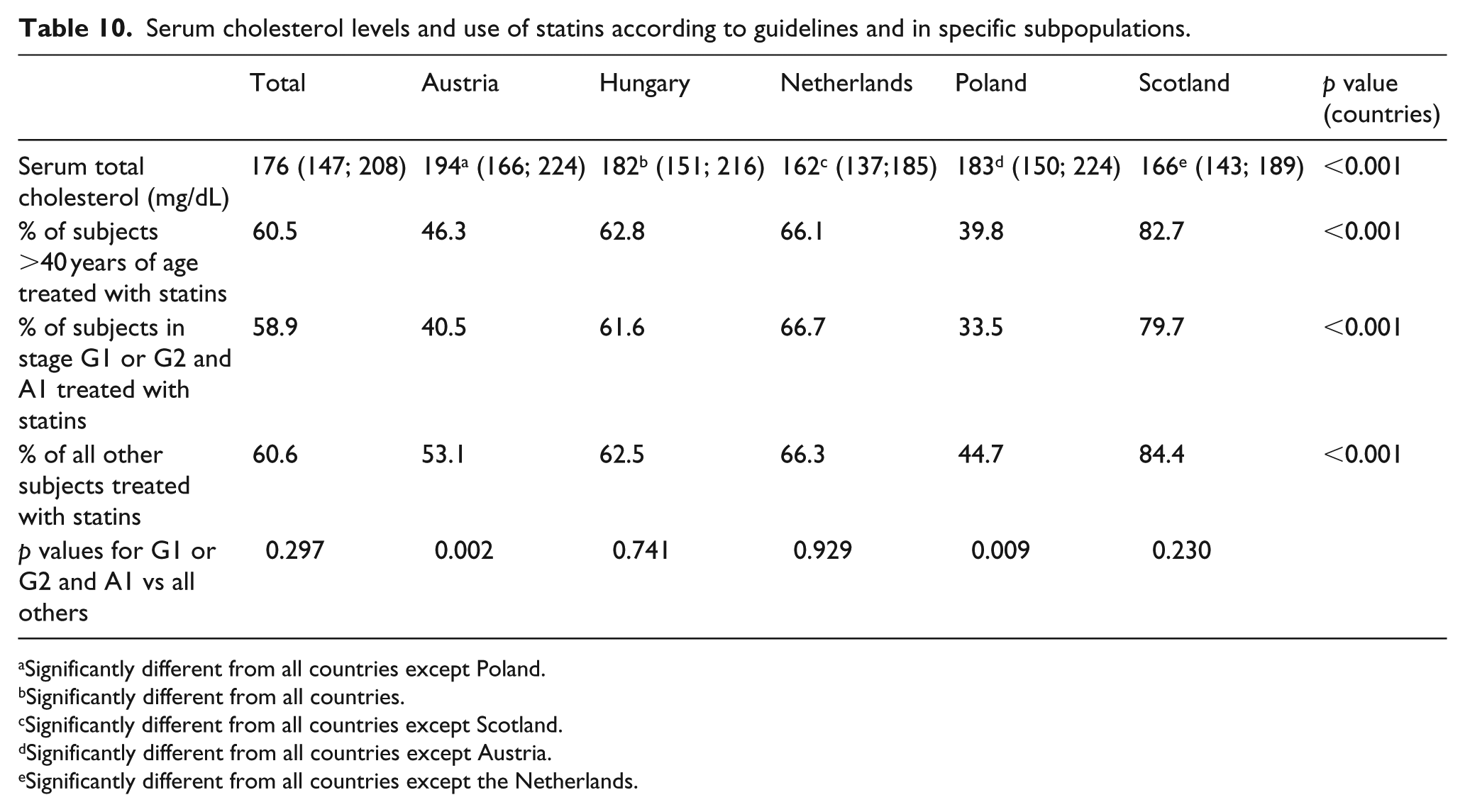
Significantly different from all countries except Poland.
Significantly different from all countries.
Significantly different from all countries except Scotland.
Significantly different from all countries except Austria.
Significantly different from all countries except the Netherlands.
Use of ASA according to guidelines and in specific subpopulations.
In general, patients on statin therapy were older, more likely to be male and had significantly lower cholesterol levels than those not treated. Their cardiovascular comorbidity was much higher leading to the conclusion that prescription of statin therapy was driven rather by cardiovascular comorbidity than guideline recommendation.
Overall, ASA use was low in all countries, of the 3560 patients older than 50 years only about 29% were treated. However, a huge difference between the countries was observed. On average, patients with renal disease were more likely to be treated. Similar to statin therapy, the administration of ASA was mostly driven by the presence of cardiovascular disease and especially coronary artery, peripheral or cerebrovascular disease. Interestingly, patients with advanced heart failure were significantly less likely to receive ASA-containing drugs.
Discussion
In general, our study shows that there is room for improvement regarding guideline adherence at the primary level of healthcare in patients with T2DM at least in the European countries included in PROVALID. Blood pressure control was poor in patients with elevated albuminuria with only 15% of all subjects reaching the recommended target values of <130/80 mm Hg. Both ADA and KDIGO suggest statin therapy in patients with T2DM or CKD without taking care of serum cholesterol levels, yet only about 60% of participants received medication. The rate of prescription was even lower for ASA (approximately 30%). Our data suggest that contrary to guideline recommendations, the latter two treatments were rather used because of the presence of cardiovascular comorbidities than in a ‘primary prevention’ effort.
An additional interesting aspect is the large variability of therapeutic practice pattern between the countries despite the fact that the populations recruited were quite similar with regard to patient history and the prevalence of risk factors and comorbidities. One reason for the observed diversity could be that GPs rather follow national guidelines. However, the Austrian Society of Nephrology has endorsed the KDIGO guidelines and the Austrian Diabetes Association 15 issued a statement that also closely follows the ADA/KDIGO suggestions. The situation is similar in Scotland, 16 Poland 17 and Hungary.18,19 Guidelines in the Netherlands also mostly follow KDIGO and ADA but suggest even lower blood pressure goals. However, statin therapy is recommended only in patients with serum cholesterol levels >2.5 mmol/L and thiazide diuretics should be administered as first-line therapy in patients without micro- or macroalbuminuria. 20 Neither the Netherlands nor Scotland local guidelines specifically recommend aspirin therapy for patients with T2DM.
Available evidence-based guidelines provide targets and performance measures for the treatment of T2DM patients, but obviously, a wide gap separates guidelines-driven recommendations from their clinical application, a phenomenon hindering the transfer of proven benefits to affected populations. In this regard, the results of our study replicate the findings of other authors in patients with diabetes and comorbidities like coronary artery or cerebrovascular disease. Bohn et al. 21 studied almost 30,000 German and Austrian patients with T2DM with respect to secondary prevention after myocardial infarction (MI) and stroke. HbA1c goal according to national guidelines <7.5% was achieved in 64.9% (MI) and in 61.1% (stroke) of patients; LDL-C <100 mg/dL was documented in 56.2% (MI) and in 42.2% (stroke). Target values of blood pressure (<130/80 mm Hg in MI, 120/70–140/90 in stroke) were reached in 67.0% (MI) and in 89.9 % (stroke). Prescription prevalence of inhibitors of platelet aggregation was 50.7% (MI) and 31.7% (stroke). About 57% (MI) and 40.1% (stroke) used statins. Similar data were reported by Modesti et al. 22 in Italy and Renard et al. 23 in Luxembourg. A total of 6187 patients with coronary artery disease were investigated in EUROASPIRE IV in 24 European countries 2012–2013. About 46% had no diabetes, 19% were newly diagnosed at enrolment and 35% were known diabetics. The optimum use of cardio-protective drugs in these groups was 53%, 55% and 60%, respectively. A blood pressure target of <140/90 mm Hg was achieved in 68%, 61% and 54%, and an LDL-C target of <1.8 mmol/L was achieved in 16%, 18% and 28%. Despite the fact that compared with data from previous surveys the use of cardio-protective drugs had increased and more patients were achieving the risk factor treatment targets, the authors concluded that there is further potential to improve the management of patients with diabetes and coronary artery disease. 24
Several efforts have been tested for their capacity to improve guideline adherence. In the United States, Kuo et al. compared care provided to patients with diabetes mellitus by nurse practitioners (NPs) and primary care physicians (PCPs) and found no significant difference. NPs and PCPs had similar rates of LDL-C testing and nephropathy monitoring, but NPs had lower rates of eye examinations and HbA1c testing. NPs were more likely to have consulted cardiologists, endocrinologists, and nephrologists. There was no statistically significant difference in adjusted Medicare spending between the two groups. 25
Another approach taken is to use incentive-based primary care, a fee for service-funding model. In British Columbia, these incentives, after controlling for patients’ age, sex, service needs level and continuity of care (defined as attachment to a general practice), reduced the net annual healthcare costs for patients with hypertension, chronic obstructive pulmonary disease and congestive heart failure, but not diabetes mellitus. 26 A recent Cochrane Database review concluded that the use of financial incentives is growing but the authors put forward that there is insufficient evidence to support or not support this trend. Implementation should proceed with caution and incentive schemes should be more carefully designed before implementation. 27 In line with this Boyd et al. 28 concluded for a group of elderly multi-morbid subjects pay for service incentives and the resulting adherence to guidelines lead to undesired polypharmacy and inadequate care. In this context, it is interesting to note that during the period of recruitment into PROVALID, primary care providers received financial reimbursement in Scotland for meeting audit and/or treatment targets for patients with diabetes under the arrangements of the Quality and Outcomes Framework (QOF). QOF is intended to standardize improvements in the delivery of primary medical services. For diabetes, specific QOF targets for reimbursement during the period of study included percentage of diabetic patients registered with that primary care provider with blood pressure <150/90 mmg and/or <140/80 mm Hg, respectively, percentage treated with an ACE inhibitor (or ARB) in the presence of micro/macroalbuminuria, percentage with IFCC HBA1c at various thresholds (59, 64 and 75 mmol/mol) and percentage with cholesterol <5 mmol/L.
Electronic health records might be an interesting tool to improve guideline adherence. In a study by Ancker et al. 29 (183,095 visits with 61,977 patients), condition-specific best-practice alerts and order sets were associated with better scores on clinical quality measures capturing processes in diabetes, cancer screening, tobacco cessation, and pneumonia vaccination. For example, providers above the median in use of tobacco-related alerts had higher performance on tobacco cessation intervention metrics and providers above the median in use of diabetes order sets had higher quality on diabetes LDL testing. However, post hoc examination of the results showed that the positive associations were with measures of healthcare processes (such as rates of LDL testing), whereas there were no positive associations with measures of healthcare outcomes (such as LDL levels). 29 Similar effects were reported by Benkert et al. 30
Finally, CME efforts might be applied. About 53% of 383 physicians completing a questionnaire reported using diabetes guidelines routinely. Mean diabetes knowledge score for guideline users was significantly higher than non-guideline users. The former were significantly more likely to report a good understanding of type 2 diabetes medications, less likely to report their unfamiliarity with insulin as an important barrier to early insulin use and with pharmacologic options as a barrier to prescribing intensive multifactorial interventions. Associations remained significant after adjusting for physician specialty, practice volume and frequency diagnosing or treating diabetes patients. 31
Conclusion
In summary, our study shows that international society guidelines for patients with T2DM are only partially followed at the primary level of healthcare in the European countries included in our study. In addition, treatment applied varies widely. It cannot be answered by our cross-sectional analysis if this diversity affects clinical outcomes. Only longitudinal follow-up data from our cohort will help us to understand whether our findings contribute to the reported national variability in the incidence of ESRD.
Supplemental Material
dvdres-feb-2018-00028-File003 – Supplemental material for Guidelines and clinical practice at the primary level of healthcare in patients with type 2 diabetes mellitus with and without kidney disease in five European countries
Supplemental material, dvdres-feb-2018-00028-File003 for Guidelines and clinical practice at the primary level of healthcare in patients with type 2 diabetes mellitus with and without kidney disease in five European countries by Susanne Eder, Johannes Leierer, Julia Kerschbaum, Laszlo Rosivall, Andrzej Wiecek, Dick de Zeeuw, Patrick B Mark, Georg Heinze, Peter Rossing, Hiddo L Heerspink and Gert Mayer in Diabetes & Vascular Disease Research
Footnotes
Acknowledgements
S.E. and J.L. have contributed equally.
Author’s contribution
All authors contributed to writing of the paper, results and discussion. S.E, J.L, J.K., G.H. and G.M. conducted data analysis. All authors except J.L. and J.K. were responsible for study design and conduct. H.L.H, L.R., A.W., P.B.M. and G.M. are national coordinators.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was in part funded by the European Union (7th Framework grant number 241544: ‘Systems Biology towards Novel Chronic Kidney Disease Diagnosis and Treatment’) and AbbVie.
Availability of data
The data sets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethical approval
The PROVALID study protocol was approved by the local IRB in each participating country.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.