
Abstract
Background:
Continuous-wave Doppler is frequently used for detecting peripheral arterial disease in patients with diabetes; however, there is limited evidence investigating diagnostic accuracy. This study aimed to determine sensitivity and specificity of continuous-wave Doppler for detecting peripheral arterial disease in populations with, and without, diabetes and to investigate the influence of disease severity on sensitivity of continuous-wave Doppler for detecting peripheral arterial disease.
Results:
Data from 396 participants were included. Using colour Duplex ultrasound as reference standard (N=66), printed continuous-wave Doppler waveform analysis sensitivity was 81.75% (95% confidence interval: 76.75 to 85.88) and specificity 89.34% (95% confidence interval: 82.62 to 93.67). Printed continuous-wave Doppler waveform analysis sensitivity for peripheral arterial disease was comparable to sensitivity calculated using angiography as the reference standard (81.67%; 95% confidence interval: 69.56 to 90.48). Sensitivity and specificity were unaffected by diabetes diagnosis (n = 176), sensitivity 82.76% (95% confidence interval: 74.86 to 88.55), and specificity 88.33% (95% confidence interval: 77.82 to 94.23).
Conclusion:
Continuous-wave Doppler is a fair assessment tool for peripheral arterial disease in a community-based sample with suspected peripheral arterial disease. Diagnostic accuracy of continuous-wave Doppler for peripheral arterial disease is unaffected by the presence of diabetes.
Keywords
Introduction
Continuous-wave Doppler (CWD) ultrasound examination is an essential part of the vascular laboratory examination. It is also utilised by nurses, general physicians and podiatrists as part of lower limb vascular assessment. The advantages of CWD include its accessibility, relative low cost of application and speed of measurement. While reliability can be variable,1,2 when performed by a skilled clinician, the repeatability in a small community-based sample has been shown to be acceptable. 3 CWD waveforms are interpreted based on their sound and/or visual shape, which changes with pathology. Multiphasic waveforms (two or three sounds) are non-pathological and have a distinct shape, representing high resistance and diastolic flow reversal. Monophasic waveforms (one sound) demonstrate pathology with their slow systolic acceleration, low resistance and lack of diastolic flow reversal. 4
CWD ultrasound is commonly used in conjunction with the ankle-brachial index (ABI) and is used to identify the presence and severity of peripheral arterial disease (PAD), and to monitor the progression of the disease.4,5 There is growing evidence that the diagnostic accuracy of the ABI is limited in specific populations including those with diabetes. Variable sensitivity of the ABI for PAD has been reported in diabetes cohorts,3,6 with multiple factors including the presence of medial arterial calcification (MAC); with increased likelihood of coexistent PAD 7 and distal anatomical distribution of atherosclerotic lesions, 8 likely to contribute to this. There is initial evidence in a small community-based sample with diabetes suggesting CWD may have high diagnostic accuracy for PAD. 3 However, the diagnostic accuracy of CWD for PAD has been relatively underexplored in either the general population or diabetes cohorts. The primary aim of this study was to determine sensitivity and specificity of CWD for detecting lower limb PAD in a population suspected to have the disease. The secondary aims were to investigate the sensitivity of CWD in a population with diabetes versus without, determine the sensitivity of CWD versus angiography and furthermore ascertain the effect of MAC visualised by colour Duplex ultrasound (CDU) and PAD severity on the sensitivity of CWD.
Methods
This retrospective study was performed under ethical approval from the University of Newcastle Human Research Ethics Committee (H-2010-1230) between 2016 and 2017 at a private vascular clinic in Lake Macquarie, New South Wales, Australia. A clinical note audit was completed and data were systematically extracted from consecutive records of eligible patients. Inclusion criteria were participants who were referred to the clinic by their general practitioner due to suspected PAD. Suspected PAD included signs and symptoms of PAD such as claudication, the presence of lower limb ulceration, or abnormal results of office-based vascular screening. Colour Duplex ultrasound (CDU) measurements, digital subtraction angiography (DSA) results and CWD waveforms were extracted where available along with data relating to participant age, gender, diabetes and smoking status by two researchers (A.L.B. and P.E.T.).
Procedure
Standard clinical protocol includes CDU and CWD testing being completed within the same appointment by a qualified vascular ultrasonographer; 10 min of rest is undertaken prior to CWD measurement. All clinical examination rooms are controlled between 23° and 25°C to avoid the influence of temperature on peripheral vessels. 9 All participants are also asked to avoid intake of alcohol, smoking, exercise and caffeine prior to the testing session and a 12 h fast is also undertaken prior to their testing session to limit the aorta and iliac vessels being obstructed by gas. 10 Participants are asked whether they have complied with fasting upon presentation at their appointment, and if they have not complied, they are re-booked for a later date.
A Parks Vascular Mini Lab 1050-C is used to measure CWD waveforms with an 8.2 MHz continuous-wave pencil-style Doppler probe. CWD measurements are completed with the probe held cephalad at approximately 45° with minimal pressure applied and the foot in a relaxed and plantarflexed position. 4 The posterior tibial and anterior tibial waveforms are printed and attached to the patient record.
CDU is then performed on the limb from the distal aorta to the foot using either a Phillips CX-50 or GE Logiq-I. Grading of stenosis is conducted in accordance with the following criteria: 11 50%–75% stenosis: focal increase in velocities 250–350 cm/s and greater than threefold increase in velocities; 75%–99% (>75%) stenosis: focal increase in velocities >350 cm/s and fourfold increase in velocities; and occlusion: vessel was well visualised and no colour or Doppler flow seen. Information on the presence and extent of stenosis and MAC was also collected during CDU imaging.12–14 Patients determined as requiring re-vascularisation after CDU then underwent DSA. For these participants, angiographic images were assessed by a vascular surgeon blinded to all other clinical assessment data. Arteries were classified as >50% stenosis but less than 75%, greater than 75% stenosis and >90% occlusive disease.
DSA is performed within 4 weeks of CDU if deemed necessary within the interventional suite at the Gateshead Private Hospital. Inter-tester reliability of printed Doppler waveform interpretation was determined by two researchers (A.L.B. and P.E.T.) evaluating 30 randomly extracted Doppler waveforms. Both researchers independently classified the waveforms as monophasic (pathological) or multiphasic (normal) and were blinded to all other test results and participant details. Inter-tester reliability of the CDU scans has been established previously and shown to be adequate. 15
Statistical analysis
Inter-tester reliability of CWD interpretation was calculated with Cohen’s kappa. For sub-group analyses, data were separated into those with diabetes (diabetes group) and those without (no diabetes group). To evaluate differences between the diabetes and no diabetes groups, gender, smoking history and PAD severity were compared using Pearson’s chi square. An independent samples t-test was used for between-group comparison of age. All comparative analyses were conducted using SPSS version 24 statistical software and significance was set at <0.05.
All calculations of diagnostic accuracy were performed using Microsoft Excel. For the purposes of performing calculations relating to diagnostic accuracy, PAD was defined as one or more arteries with ⩾50% luminal stenosis for both CDU and angiographic data. Categorisation of CWD data was as follows: Multiphasic waveforms were classified as non-pathological, that is, no significant PAD. Monophasic waveforms were classified as pathological, that is, significant PAD present with ⩾50% luminal stenosis for both CDU and angiographic data. If one or more monophasic/absent Doppler waveforms were present, the limb was considered positive for PAD.
To determine the effect of disease severity on sensitivity of CWD, participants were categorised by the following severities of PAD: >50% luminal stenosis but <75%, >75% luminal stenosis but <90% and 90% luminal stenosis to occlusive disease. Sensitivity of CWD for PAD according to disease severity category was calculated for the whole group and then for the diabetes and no diabetes groups. Likewise, sensitivity and specificity of CWD for participants with visualised MAC on CDU were calculated for the participants with visualised MAC, and then, sub-analysis was conducted for those with visualised MAC with, and without, diabetes.
Sensitivity and positive likelihood ratios were also calculated for angiographic data. Due to the limited amount of data available (66 participants), sub-analysis by diabetes diagnosis was not conducted.
Results
A total of 396 participants were included in this study: 176 with diabetes (diabetes group) and 220 without diabetes (no diabetes group). Participant characteristics are included in Table 1. The diabetes and no diabetes groups were compared and there were no significant differences in gender (p = 0.22), prevalence of PAD (p = 0.16) and smoking history (p = 0.16; Table 1). There was a significant difference in age between groups (p = 0.001), with the no diabetes group older (no diabetes group mean age = 78.11 years and diabetes group mean age = 74.65 years). In all, 66 participants underwent angiography and these participant characteristics are in Table 2. Inter-tester reliability for interpretation of CWD waveforms was substantial [К: 0.66; 95% confidence interval (CI): 0.36 to 0.95].
Participant characteristics: Doppler versus CDU.
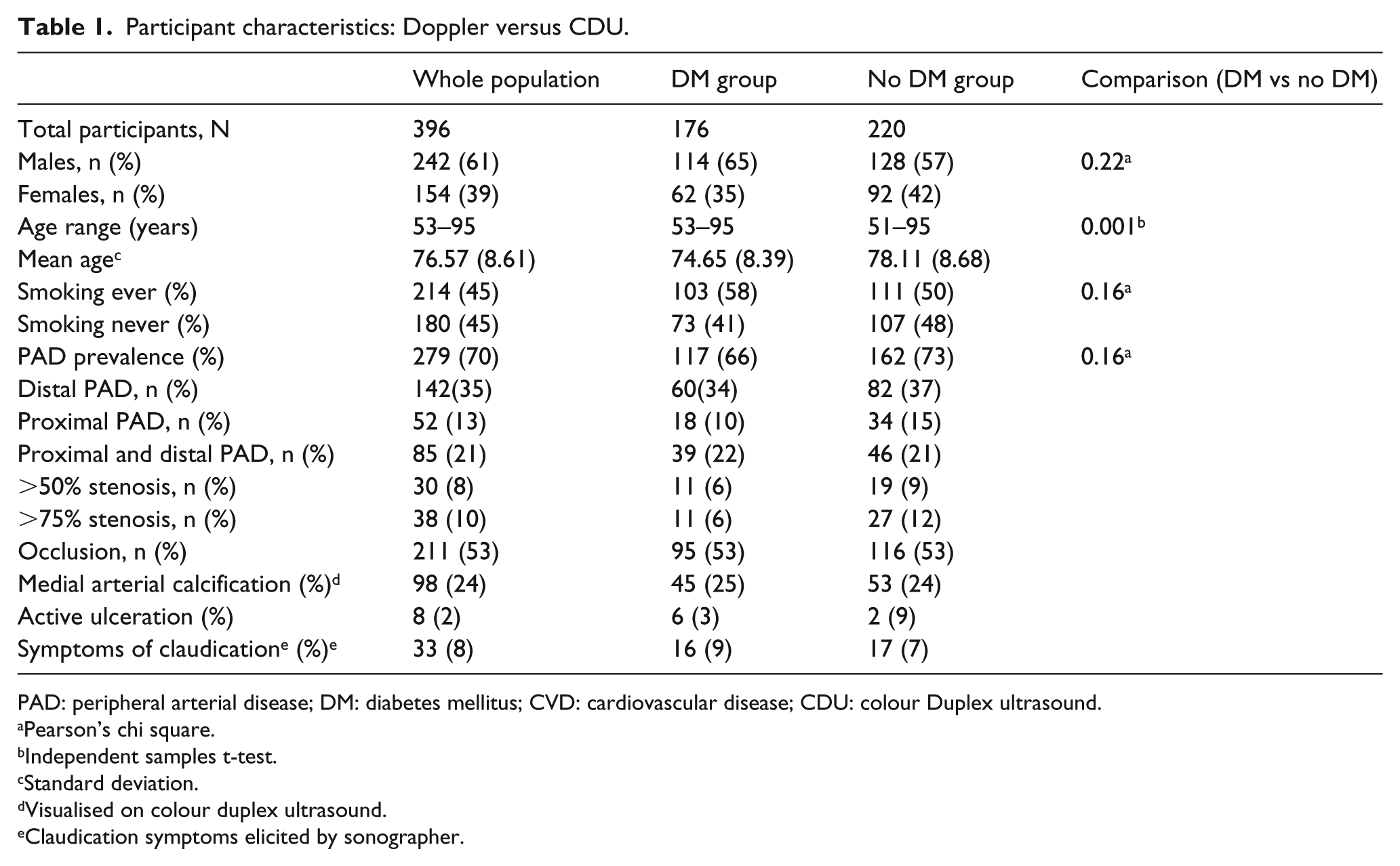
PAD: peripheral arterial disease; DM: diabetes mellitus; CVD: cardiovascular disease; CDU: colour Duplex ultrasound.
Pearson’s chi square.
Independent samples t-test.
Standard deviation.
Visualised on colour duplex ultrasound.
Claudication symptoms elicited by sonographer.
Participant characteristics: Doppler versus angiography.
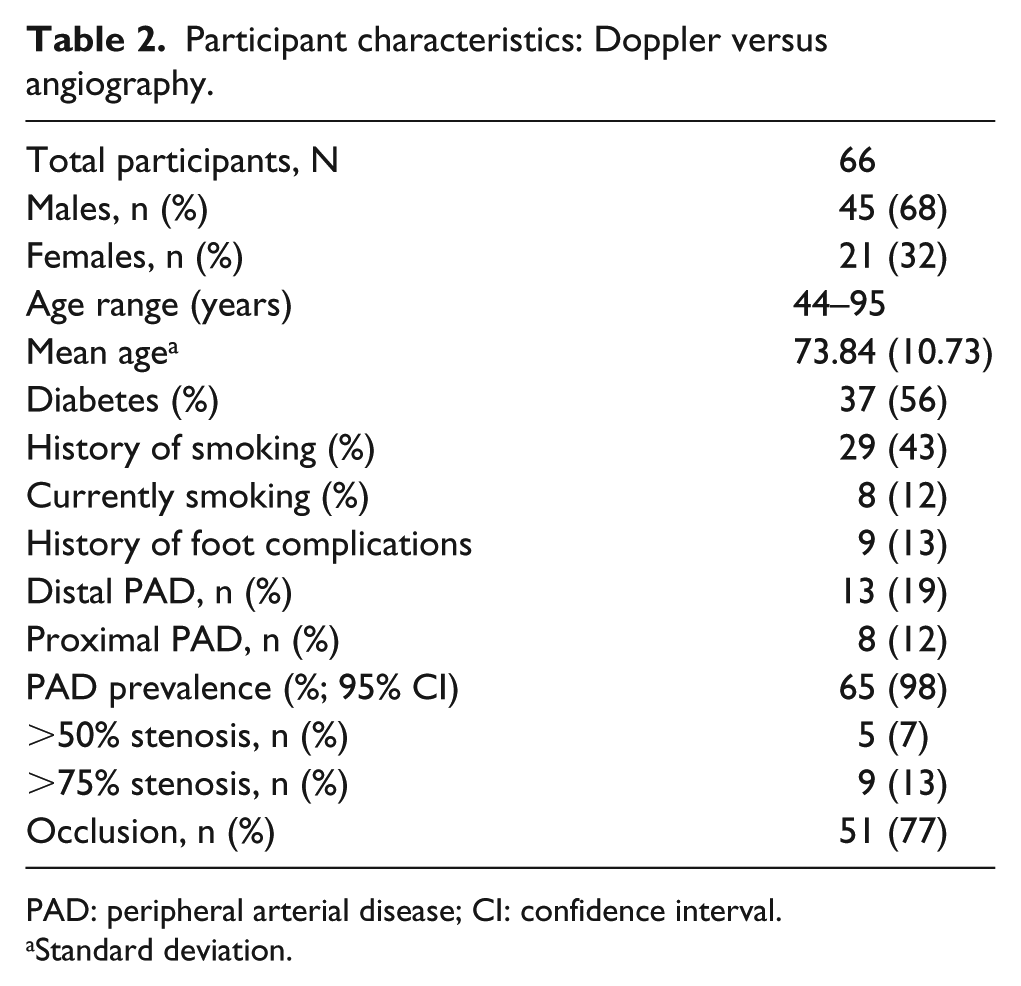
PAD: peripheral arterial disease; CI: confidence interval.
Standard deviation.
Sensitivity, specificity and positive and negative likelihood ratios are all shown in Table 3. Overall, CWD was 81.75% sensitive (95% CI: 76.75 to 85.88) for identifying PAD and 89.34% specific (95% CI: 82.62 to 93.67) in the whole population with suspected PAD, using CDU as the reference standard. Positive and negative likelihood ratios were relatively important (7.67) and nearing importance (0.20), respectively. The group who underwent angiography (N = 66) had an overall sensitivity of 81.67% (95% CI: 69.56 to 90.48) for CWD detecting PAD.
Validation table: all groups with suspected PAD.
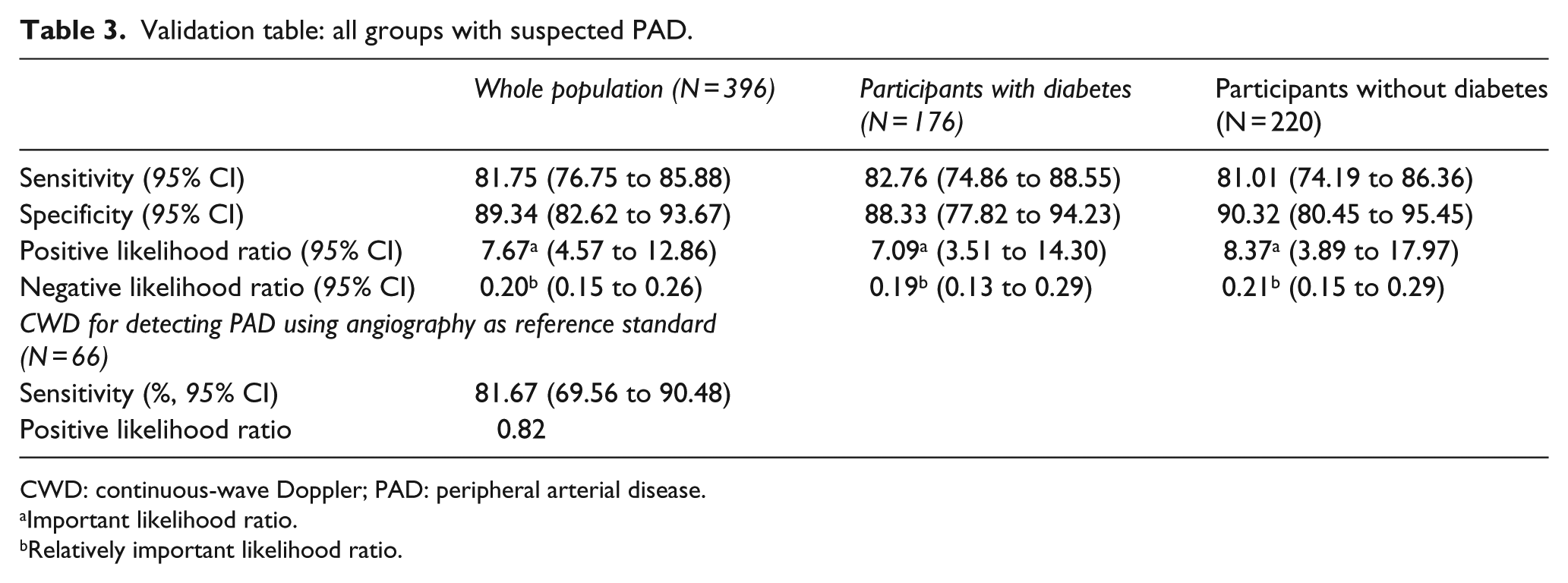
CWD: continuous-wave Doppler; PAD: peripheral arterial disease.
Important likelihood ratio.
Relatively important likelihood ratio.
Sub-group analyses showed that sensitivity was similar for the diabetes (82.76%) and no diabetes groups (81.01%; Table 3). This was also the case for specificity (diabetes group: 88.33%, no diabetes group: 90.32%).
Sensitivity of CWD for PAD by disease severity is shown in Table 4. Of note, CWD had the highest sensitivity for detecting PAD when occlusive disease was present in the whole population (85.31%) as well as in the sub-analysis of no diabetes (85.34%) and diabetes (85.26%) groups. For the whole population and the no diabetes group, milder disease (>50%–74% stenosis) was associated with poorer sensitivity (whole population: 58.62%, no diabetes group: 50.00%; Table 4). In the diabetes group, sensitivity was lowest in the >75% category (54.55%; Table 4).
Sub-group analysis of CWD in diabetes group and no diabetes group.
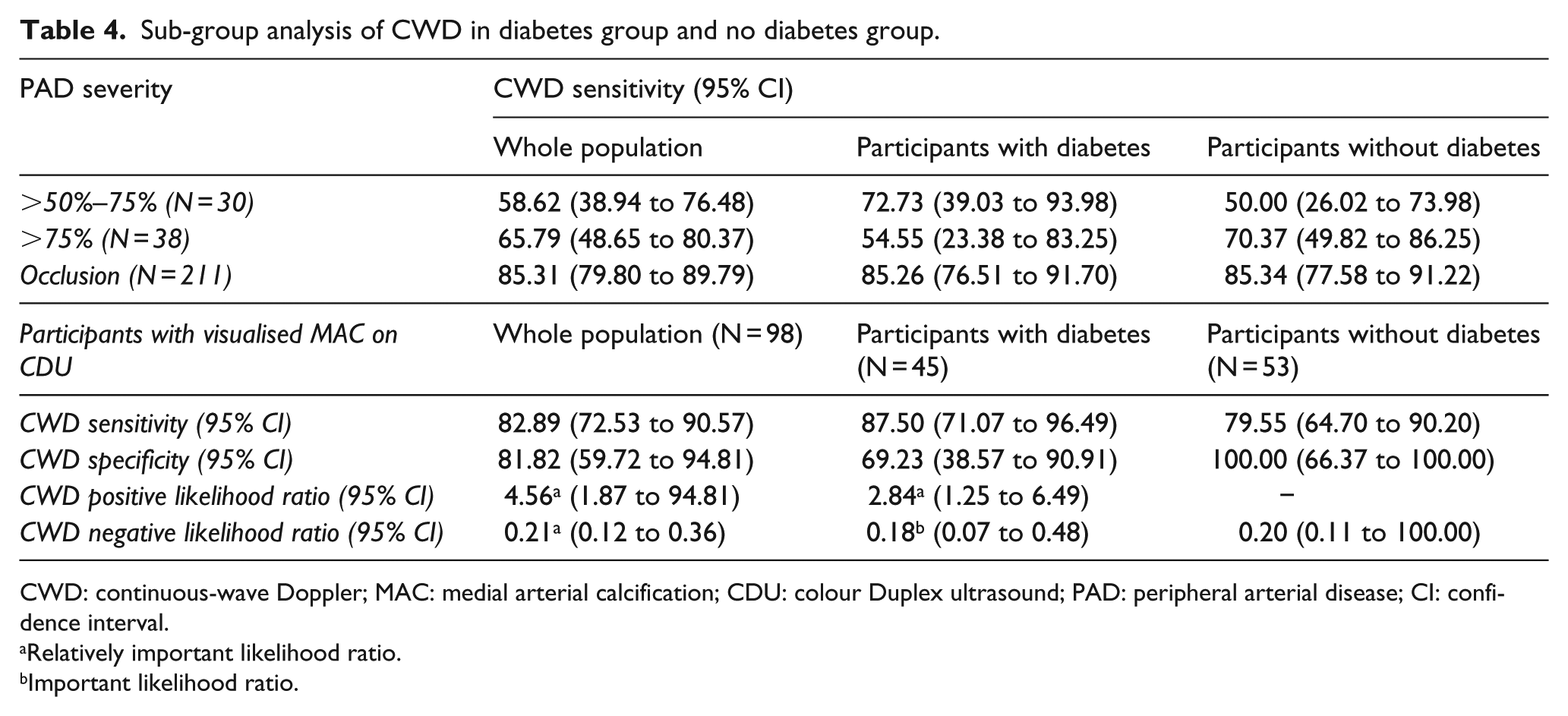
CWD: continuous-wave Doppler; MAC: medial arterial calcification; CDU: colour Duplex ultrasound; PAD: peripheral arterial disease; CI: confidence interval.
Relatively important likelihood ratio.
Important likelihood ratio.
Sensitivity and specificity of CWD for PAD in participants with visualised MAC are reported in Table 4. In the group with visualised MAC (N = 98), sensitivity (82.89%; 95% CI: 72.53 to 90.57) was similar to the sensitivity of CWD for PAD in the whole group (N = 396; 81.75%; 95% CI: 76.75 to 85.88). However, specificity was lower in those with visualised; MAC = 81.82% (95% CI: 59.72 to 94.81) compared to the whole group (89.34; 95% CI: 82.62 to 93.67). Within the group of participants with visualised MAC, sub-analysis by diabetes status showed that the presence of diabetes was associated with higher sensitivity of CWD for PAD (87.50%) but lower specificity (69.23%) compared to those without diabetes (sensitivity 79.5% and specificity 100%).
Discussion
The primary aim of this study was to investigate the sensitivity and specificity of CWD for PAD in people with suspected disease. This research has demonstrated that both sensitivity and specificity of CWD for detecting PAD (defined as one or more arteries >50% stenosis) using CDU as the reference standard are high and that this is relatively unaffected by the presence of diabetes. Overall sensitivity of CWD for detecting PAD in the whole population using CDU as a reference standard was good (81.75%), with relatively important positive likelihood ratios (7.67). Sensitivity was unaffected by the presence of diabetes (sensitivity diabetes group: 82.76%, no diabetes group: 81.01%). Similar sensitivity was determined in the angiography sub-group (n = 66), with an overall sensitivity of 81.67%. These general findings suggest that CWD is a useful clinical test, with a positive or pathological test result associated with a moderate increase in probability of the disease. 16 These findings are consistent with previous prospective investigations in a smaller community-based sample which demonstrated similar sensitivities in groups with and without diabetes. 6 The similar performance of this test in the diabetes group compared to the no diabetes group may be due to the fact that CWD appears to have higher sensitivity in more severe disease groups. This is typically found more frequently in diabetes populations,3,6 and this was the case in this diabetes cohort in this study, where the majority of PAD was occlusive.
The specificity for CWD for detecting PAD using CWD as the reference standard for the whole population was good 16 (88.39%) and, again, appeared to be unaffected by the presence of diabetes (diabetes group: 88.33%, no diabetes group: 90.32%). These results indicate that CWD is unlikely to result in a false diagnosis of PAD, consistent with previous findings.3,6 Negative likelihood ratios approximately 0.20 in both groups indicate that a negative CWD result is associated with a moderate decrease in probability of PAD. 16
Investigation of the sensitivity of CWD for PAD by severity and location of disease identified several potential limitations of this form of assessment. Although findings should be interpreted with caution due to small numbers of limbs with mild and moderate disease, overall CWD was a more effective diagnostic tool in the presence of occlusive disease, and this was the case regardless of diabetes diagnosis. Results for those with occlusive disease were similar across all groups, with the whole group sensitivity of CWD for detecting PAD 85.31%, the group with diabetes 85.26% and the no diabetes group 85.34%. Generally, the lowest sensitivities were found in the least severe disease groups (>50%–74% stenosis), indicating that CWD may not be the ideal diagnostic tool in the early or less severe stages of PAD. However, the poorer performance of CWD for detecting mild PAD needs to be considered in light of the small number of participants with mild disease (n = 30). Further exploration of this finding in a larger population with mild disease needs to be undertaken to confirm these findings.
The presence of visualised MAC (N = 98) was associated with similar sensitivity (82.89 %), but reduced specificity (81.82%) of CWD for the presence of PAD compared to results for the whole group of participants (n = 396; sensitivity 81.75% and specificity 89.34%). The reduction in specificity equates to an increased likelihood of false-positive test result, that is, the PAD is identified by the test as being present when it is not. This suggests that an abnormal CWD waveform can also occur in the presence of MAC. This is clinically relevant because similar to the presence of PAD, MAC has been demonstrated to be an indicator of systemic vascular disease. Specifically, MAC has been shown to have strong predictive capacity for cardiovascular morbidity and mortality, development of diabetes-related microvascular complications and increased risk of lower limb amputation.17,18 Therefore, while this may reduce the specificity of CWD for identifying PAD, it does provide a mechanism for identifying more generalised lower limb vascular disease.
The findings of this study need to be considered in light of a number of limitations. The generalisability of these results is limited to similar populations, and the participants with PAD in this study tended to have occlusive disease. In addition, collection and interpretation of Doppler waveforms is operator dependent. Although we conducted a reliability study as part of this research and in previous studies with adequate results, reliability of Doppler waveform interpretation in the literature is variable. Categorising Doppler waveforms as normal or abnormal also does not take into account the nuances of waveform interpretation, including data on disease location and severity, which can sometimes be determined. While the sonographers involved in this study always follow clinical protocol, the retrospective nature of this study made tight control of examination conditions not possible and there was a lack of blinding for CWD and CDU results. While CDU is used clinically, and also in many research studies as a valid reference standard, it is not considered the gold standard imaging technique and was used as the reference standard for the largest group in this study. However, given the results were not significantly different between our angiography and CDU groups, this further suggests that CDU can be used as a reference standard for this study type. Also, the high percentage of participants with PAD (70%) may have led to spectrum bias which may lead to overestimation of the overall accuracy of the index test. Furthermore, a previous study in a community-based population demonstrated that sensory neuropathy has a negative effect on diagnostic accuracy of CWD. 6 Due to the retrospective nature of this study, data pertaining to neurological status were not available as neurological screening is not part of routine practice in the vascular laboratory. Future studies of diagnostic accuracy in diabetes populations should include neurological status of participants.
Conclusion
CWD is a fair assessment tool for PAD, particularly in diabetes cohorts, and cohorts with moderate to severe disease. Positive and negative likelihood ratios and the subjective nature of the assessment suggest this should not be used as standalone vascular assessment but has good clinical utility for use in combination with other objective vascular assessment tools such as the ABI or toe-brachial index.