
Abstract
Aim:
To evaluate whether a combination of isosorbide dinitrate spray and chitosan gel (10%) topically applied can have additive benefits for management of diabetic foot ulcers.
Methods:
In a randomized, placebo-controlled, double-blinded clinical trial, 68 patients were divided into four groups: Group 1: treated with chitosan gel; Group 2: isosorbide dinitrate spray; Group 3: combination of isosorbide dinitrate spray and chitosan gel; Group 4: placebo.
Results:
Histological analyses showed a significant regeneration in all groups (p < 0.001). On the final assessment of the ulcer, using the combination was found a wound closure percentage of 71 ± 30, 70 ± 27 using isosorbide dinitrate, 58 ± 30 with chitosan and 50 ± 16 with placebo. The number of patients who achieved complete ulcer closure was six using the combination, four with isosorbide dinitrate, three with chitosan and one with placebo. The progression in the healing process of the ulcer showed marked inmunohistochemical differences of Von Willebrand Factor, desmin, vascular endothelial growth factor-A and α-smooth muscle actin in all groups (p < 0.001), but without notable differences between them.
Conclusion:
The combination was better than placebo to reduce the dimensions of the ulcer, accelerate healing and increase the number of patients who achieved complete closure of the ulcer, but the combination was not better than chitosan or isosorbide dinitrate used separately.
Introduction
Foot ulcers affect about 15% of patients with diabetes, remain one of the most common causes of hospitalization and comprise 85% of lower-limb amputations in diabetic patients. 1 The risk of leg amputation is correlated with the grade and stage of the wound and other determinants such as peripheral sensomotoric neuropathy, ulceration, infection and peripheral vascular disease. 2 The management of diabetic foot ulcers (DFU) requires a multi-disciplinary approach, including control of the diabetes, orthotic shoes, off-loading devices, wound care and surgery in selected cases. 3 However, treatment of DFU remains challenging because of frequent unsatisfactory results from both surgical and non-surgical treatments.
Isosorbide dinitrate (ISDN) is an organic nitrate and a vasodilator with effects on arteries and veins. The chemical name of ISDN is 1,4:3,6-dianhydro-2,5-di-O-nitro-D-glucitol. The principal pharmacological action of ISDN is relaxation of the vascular smooth muscle and consequent dilatation of peripheral arteries and veins. This process is mediated by the synthesis of nitric oxide (NO). Chitosan composed of randomly distributed Beta-D-glucosaminyl-(1->4)-beta-D-glucosamine and N-Acetyl-D-Glucosamine is a polymer with good haemostatic properties, natural biocompatibility, low cytotoxicity, antimicrobial activity and excellent biodegradable properties. 4 The objective of this study was to evaluate whether the combination of a vasodilation agent and a barrier therapy such as 10% chitosan gel topically applied takes advantage of each agent’s individual characteristics to render it suitable for management of DFU.
Methods
A randomized, placebo-controlled, double-blinded clinical trial was designed. Sixty-eight patients with DFU, Wagner grades I and II, 1 Ankle–brachial index >0.8 and no prior treatments for foot ulcers were included. The regular treatment each patient received was not altered for the investigation and was maintained without changes, allowing every patient to continue with their regular medications and indicated doses. If infection was encountered at the beginning of the study, patients were excluded from the study and appropriate therapy to facilitate healing was employed. If patients presented infection during follow-up, they were treated appropriately without exclusion from the study. All patients gave written informed consent and the protocol was approved by the local bioethics committee of the Health Sciences University Center of the University of Guadalajara (number 030-2010) and published under clinical trial (NCT02789033).
The patients were divided into four groups of 17 patients each. Group 1 treated with chitosan gel and placebo spray, Group 2 with ISDN spray and placebo gel, Group 3 patients with a combination of ISDN spray and chitosan gel and Group 4 patients with placebo gel and placebo spray. Before to start the medication, the ulcerated area was calculated by multiplying the largest, times, the smallest diameter (100% of ulcerated area). All patients’ wounds were cleaned using Microcyn and sterile gauze. Seven patients were eliminated because they failed to keep scheduled appointments (two each from Groups 1, 2 and 4, and one from Group 3).
Preparation of the interventions
The chitosan gel was prepared by VIDRIO Pharmaceutical (Guadalajara, Jalisco, Mexico). High-purity (90%) chitosan was acquired from Bioextracto (Mexico, D.F.) and mixed with 10 mL acetic acid solution (2%) in a porcelain mortar and agitated to obtain a homogenous mix. This was then incorporated into a base gel of the following composition: acetic acid 500 mg, methylparaben 97.5 mg, carbopol 520 mg, triethanolamine 520 mg, chitosan 10 g and distilled water to make for a total volume of 100 mL. The gel had good viscosity and a final pH of 6.0.
ISDN spray (ISOKET) was acquired from ABBOTT Laboratories (Mexico). Placebo gel was prepared under the same conditions and stored in sterile bottles at room temperature. Placebo spray consisted of saline solution. Bacteriological cultures were reported negative. Two squirts of ISDN spray (total dose of 2.5 mg) and chitosan gel 10% in a thin layer were applied under aseptic conditions every day and covered with sterile bandages.
Histological analysis
To show the host’s response of tissue reparation, including neo-angiogenesis and fibroplasia, a 4-mm punch biopsy of the periphery of the ulcer was performed with local anaesthesia, fixed in 4% PBS-buffered formaldehyde and embedded in paraffin wax, then cut longitudinally into 5-µm-thick sections and transferred to electrostatically charged slides. Specimens were analyzed using immunohistochemical staining with specific reagents for Von Willebrand Factor (vWF) (Chemicon, CA), desmin (Abcam, Cambridge, MA), vascular endothelial growth factor-A (VEGF-A) (Abcam, Cambridge, MA) and α-smooth muscle actin (α-SMA) (Abcam, Cambridge, MA). Immunoactivities were quantified from 10 images of the same specimen using a Zeiss Axioskop 2 Plus microscope (Carl Zeiss, Göttingen, Germany). All images of each specimen were captured using a Cool CCD camera (SNAP-Pro c.f. Digital kit; Media Cybernetics, Silver Spring, MD, USA). Images were analysed using Image-Pro1 Plus image-analysis software (Media Cybernetics, Silver Spring, MD, USA).
Statistical analysis
The Shapiro–Wilk test was used to evaluate normal distribution. Intragroup and intergroup values were tested using one-way analysis of variance, followed by an independent Student’s t test; p < 0.05 was considered significant; complete wound closure in each group was analysed using Fisher’s exact test. Cohen’s d test was applied to estimate the magnitude of the effect in the primary outcome after 75 days.
Results
Of the 61 patients who completed the study, 26 patients were men and 35 were women. Wagner grading was not significantly different between groups at baseline; 29 patients were Grade I and 32 were Grade II. No differences were detected between groups in demographic and other confounding variables. Our results showed a notable reduction in the diameter of the ulcer regarding baseline values in all groups, even in placebo (p < 0.001).
Iconography showed a notable tissue regeneration with granulation tissue before and after treatment in all groups, but significant recuperation was observed using the combination and also in ISDN regarding the placebo group. No serious adverse events were observed in any group. The recovery progress of the ulcer was higher using the combination compared to chitosan or placebo at 30 and 45 days (p < 0.05) but not superior to ISDN spray. At 60 and 75 days, the difference with chitosan disappeared, still being superior to placebo. At the end of the study, the percentage reduction in ulcer size using the combination was 71± 30.2, using ISDN spray 70 ± 27.1, using chitosan 58 ± 30.2 and using placebo 50 ± 16 (Figure 1).
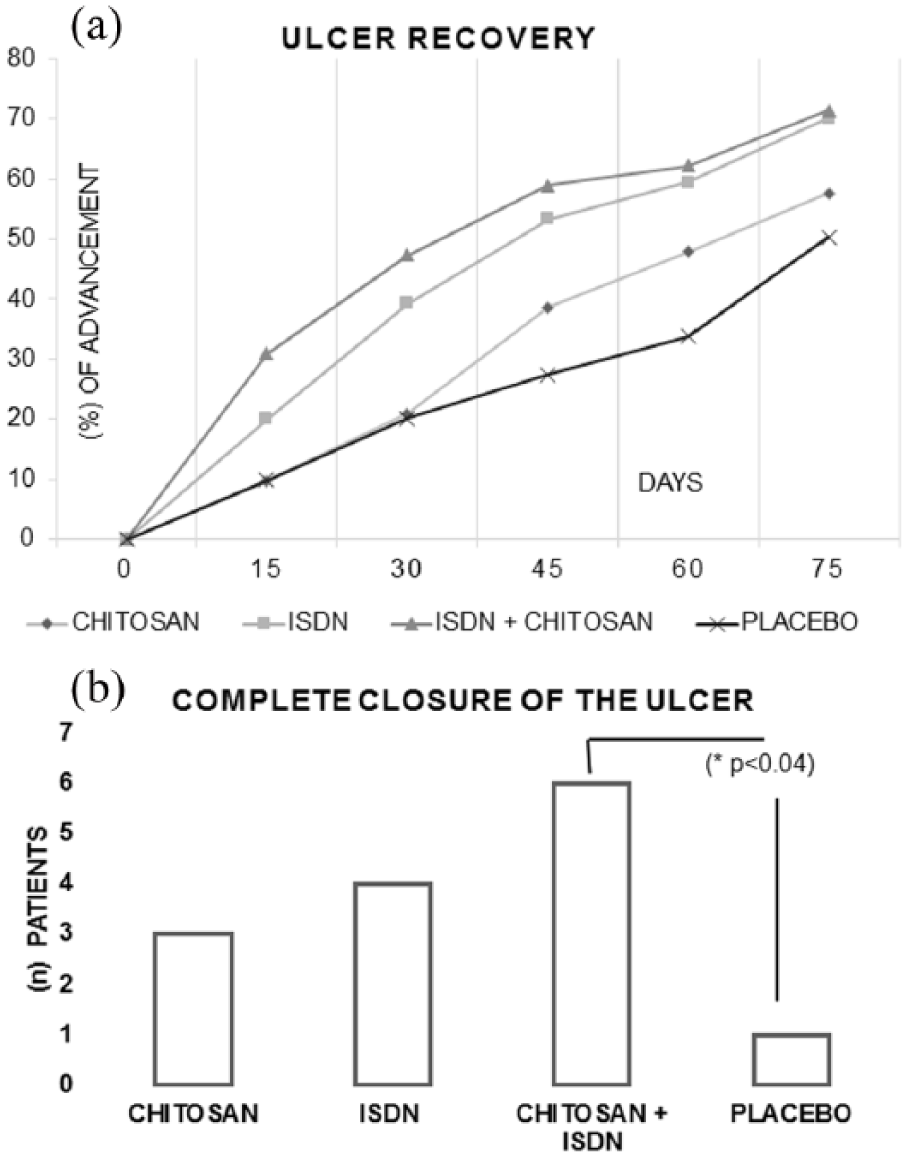
(a) Curve of the comparative effect in recovering area and (b) number of patients who achieved complete closure of the ulcer.
Although significant statistical differences were detected, Cohen’s d effect size test revealed only a ‘small effect’ using the combination or ISDN separately. The number of patients who achieved complete closure was six using the combination, four with ISDN spray, three with chitosan and one with placebo (Figure 1).
Immunohistochemical expressions of vWF, desmin, VEGF-A and α-SMA were similar in all groups before treatment but statistically significant differences appeared after treatment (p < 0.05, IC: 95%), with a slight increase in vWF in patients treated with chitosan, desmin in patients using the combination, VEFG-A in patients treated with ISDN separately and with the combination and an increase in α-SMA in patients using chitosan alone or in combination.
Discussion
Evaluating the impact of the pharmacological intervention in DFU is complex, due to the difficulty in estimating the impact of the intervention over other factors that influence the healing process and co-exist in all patients, such as the metabolic control of the patients, the time of evolution of the ulcer, the presence of infection–contamination, 5 neuropathy 6 and peripheral vascular disease, 7 all of which were taken into consideration to assure the homogeneity of the groups. 8 All of the participants received treatment for DFU in a conventional way, which contributed to the improvement observed in all of them, including the ones that received placebo. 9
Although the combination of ISDN and chitosan, or ISDN as monotherapy presented statistically significant differences compared to placebo, they only showed a ‘small effect’ (Cohen’s d test) compared to conventional treatment using microcyn and sterile gauze to clean the wound.9,10 Although progression of the ulcer was the primary outcome in the present study, we consider that complete closure of the ulcer should be more important to avoid infection and the consequent recurrence. Our results showed that the combination of ISDN and chitosan increased the number of patients who reach complete ulcer closure compared with placebo, but the sample was small to make definitive statements. Histological analysis showed an increase in vWF, desmin, VEFG-A and α-SMA in accordance with the healing evolution and not by the type of intervention. The increase in VEFG-A, secondary to wound healing, might suggest an increase in angiogenesis, which allows the activity of growth factors and cytokines.
Conclusion
The wound healing progression of the ulcerated area using ISDN plus chitosan was better at 30 and 45 days compared with chitosan or placebo, but not compared to ISDN as monotherapy, and at 60 and 75 days the progress of the ulcerated area using the combination was only greater than placebo. The use of chitosan and ISDN spray increased the number of patients who achieved complete closure of the ulcer.
Footnotes
Acknowledgements
The authors thank Leonel Garcia Valdes for the help in the preparation of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was supported by the Coecytjal, Mexico (grant number: PS-2009-752).