
Abstract
Objective:
This study assessed the association of metabolic syndrome and metabolic syndrome score with the predicted forced vital capacity and predicted forced expiratory volume in 1 s (predicted forced expiratory volume in 1 s) values in Korean non-smoking adults.
Methods:
We analysed data obtained from 6684 adults during the 2013–2015 Korean National Health and Nutrition Examination Survey.
Results:
After adjustment for related variables, metabolic syndrome (p < 0.001) and metabolic syndrome score (p < 0.001) were found to be inversely associated with the predicted forced vital capacity and forced expiratory volume in 1 s values. The odds ratios of restrictive pulmonary disease (the predicted forced vital capacity < 80.0% with forced expiratory volume in 1 s/FVC ⩾ 70.0%) by metabolic syndrome score with metabolic syndrome score 0 as a reference group showed no significance for metabolic syndrome score 1 [1.061 (95% confidence interval, 0.755–1.490)] and metabolic syndrome score 2 [1.247 (95% confidence interval, 0.890–1.747)], but showed significant for metabolic syndrome score 3 [1.433 (95% confidence interval, 1.010–2.033)] and metabolic syndrome score ⩾ 4 [1.760 (95% confidence interval, 1.216–2.550)]. In addition, the odds ratio of restrictive pulmonary disease of the metabolic syndrome [1.360 (95% confidence interval, 1.118–1.655)] was significantly higher than those of non-metabolic syndrome.
Conclusion:
Metabolic syndrome and metabolic syndrome score were inversely associated with the predicted forced vital capacity and forced expiratory volume in 1 s values in Korean non-smoking adults. In addition, metabolic syndrome and metabolic syndrome score were positively associated with the restrictive pulmonary disease.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality in high- and middle-income countries. Estimates from WHO’s Global Burden of Disease and Risk Factors project show that in 2015, COPD was the fifth leading cause of death in high-income countries (5.0% of total deaths) and was the third leading cause of death in middle- to high-income countries (6.9% of total deaths). 1 Impaired lung function, which is indicated by reduced forced expiratory volume in forced vital capacity (FVC) and first second of exhalation [forced expiratory volume in 1 s (FEV1)], contributes significantly to cardiovascular and all-cause mortality.2–4 Impaired lung function may also occur due to smoking, hypertension, insulin resistance and type 2 diabetes mellitus (DM).5–9
Metabolic syndrome (MetS) is characterized by insulin resistance and is indicated by the presence of more than three out of the five MetS components [abdominal obesity, elevated blood pressure (BP), elevated fasting blood glucose (FBG), elevated triglycerides (TGs) and reduced high-density lipoprotein cholesterol (HDL-C)]. 10 MetS has been associated with increased risks of cardiovascular disease and all-cause mortality.11–13
Recently, research on MetS and pulmonary function has gained momentum worldwide.14–18 However, to our knowledge, no study involving large-scale populations to assess the relationship between MetS and decreased pulmonary function in non-smoking adults has been conducted. In addition, it is unclear whether the association can be observed in Korean populations. As such, this study aimed to investigate the association between the predicted FVC and FEV1 values and MetS and metabolic syndrome score (MSS) in Korean non-smoking adults aged ⩾20 years using the data obtained in 2013–2015 during the sixth Korean National Health and Nutrition Examination Survey (KNHANES-VI).
Methods
Study subjects
This study was based on most recent data from the KNHANES-VI (2013–2015). The KNHANES is a cross-sectional survey conducted nationwide by the Division of Korean National Health and Welfare. KNHANES comprises a health interview survey, a health behaviour survey, a health examination survey and a nutrition survey. Households as sampling units were stratified and collected through a multistage, probability-based sampling design based on sex, age and geographic area, using household registries. At the time each survey was done, participants provided written informed consent for use of their data in further analyses and were given the right to refuse to participate, in accordance with the National Health Enhancement Act. In the KNHANES-VI, 22,948 individuals over age 1 were sampled for the survey. We excluded 13,524 subjects who were missing for pulmonary function test and those (592 subjects) for whom data were missing for important analytic variables, such as various blood chemistry tests. In addition, we excluded the current smoker (2148 subjects who smoked more than one cigarette a day). Finally, 6684 subjects were included in the statistical analysis. The KNHANES-VI study has been conducted according to the principles expressed in the Declaration of Helsinki (2013-07CON-03-4C, 2013-12EXP-03-5C, 2015-01-02-6C). All participants in the survey signed an informed written consent form. Further information can be found in ‘The KNHANES-VI Sample’, which is available on the KNHANES website. The data from KNHANES are available on request by email if the applicant logs onto the ‘Korea National Health and Nutrition Examination Survey’ website.
General characteristics and blood chemistry
Research subjects were classified by gender and by age into less than 50, 50–59, 60–69 and 70 years or older. Research subjects were classified by sex (males and females), alcohol drinking (yes or no) and regular exercise (yes or no). Alcohol drinking was indicated as ‘yes’ for participants who had consumed at least one glass of alcohol every month over the last year. Regular exercise was indicated as ‘yes’ for participants who had exercised on a regular basis regardless of indoor or outdoor exercise. Regular exercise was defined as 30 min at a time and 5 times/week in the case of moderate exercise, such as swimming slowly, doubles tennis, volleyball, badminton, table tennis and carrying light objects; and for 20 min at a time and 3 times/week in the case of vigorous exercise, such as running, climbing, cycling fast, swimming fast, football, basketball, jump rope, squash, singles tennis and carrying heavy objects. Anthropometric measurements included body mass index (BMI), waist measurement (WM), systolic blood pressure (SBP) and diastolic blood pressure (DBP). Blood chemistry included measurement of total cholesterol (TC), HDL-C, TGs, FBG, predicted FVC, predicted FEV1 and FEV1/FVC.
MetS and MSS and decreased pulmonary function
MetS was defined using the diagnostic criteria of the Revised National Cholesterol Education Program–Adult Treatment Panel III (Revised NCEP-ATP III) based on common clinical measures, including TGs, HDL-C, BP, FBG and WM. TGs over 150 mg/dL was set as the criteria for elevated TGs. The criteria for reduced HDL-C were HDL-C of less than 40 and 50 mg/dL for males and females, respectively. FBG over 100 mg/dL was set as the criteria for elevated FBG. SBP over 130 mm Hg or DBP over 85 mm Hg was set as the criteria for elevated BP. The criteria for abdominal obesity were abdominal measurements of over 90 and 80 cm for men and women, respectively, according to the Asia-Pacific criteria. 19 The presence of defined abnormalities in any three of these five measures constitutes a diagnosis of MetS. The MSS indicates the presence of abdominal obesity, elevated BP, elevated FBG, elevated TGs or reduced HDL-C. Subjects without any of the five risk factors received an MSS 0, and those with one, two, three and four or more of the risk factors received an MSS score of 1, 2, 3 and ⩾4, respectively. 20 The obstructive pulmonary diseases (OPDs) were defined FEV1/FVC < 70.0%, and restrictive pulmonary diseases (RPD) were defined the predicted FVC < 80.0% with FEV1/FVC ⩾ 70.0%.21,22
Statistical analysis
The collected data were statistically analysed using SPSS WIN version 18.0 (SPSS, Inc., Chicago, IL, USA). The distributions of the participant characteristics were converted into percentages, and the successive data were presented as means with standard deviations. The average differences in the predicted FVC and FEV1 for MetS characteristics were calculated using an independent t-test. We conducted the analysis of covariance (ANCOVA) test for the predicted FVC and FEV1 according to MetS or MSS after adjusted for age, gender, drinking alcohol, regular exercise, and BMI. In the case of logistic regression for odds ratio (OR) of the RPD and OPD, the four models constructed were as follows: (1) MSS or MetS, (2) further adjusted for age and gender, (3) further adjusted for drinking alcohol and regular exercise and (4) further adjusted for BMI. The significance level for all of the statistical data was set as p < 0.05.
Results
Clinical characteristics of research subjects
The clinical characteristics of the research subjects are shown in Table 1. The prevalence rates of MetS in males and females were 708 (30.2%) and 1408 (32.5%), respectively. The prevalence rates of RPD and OPD were 569 (9.7%) and 828 (13.5%), respectively. The following parameters were significantly higher (p < 0.001) in males than in females: alcohol drinkers, regular exercise, SBP, DBP, BMI, WM, TC, FBG, RPD and OPD. However, the following were significantly lower (p < 0.001) in males than in females: TGs, HDL, predicted FVC, predicted FEV1 and FEV1/FVC.
General characteristics of research subjects.
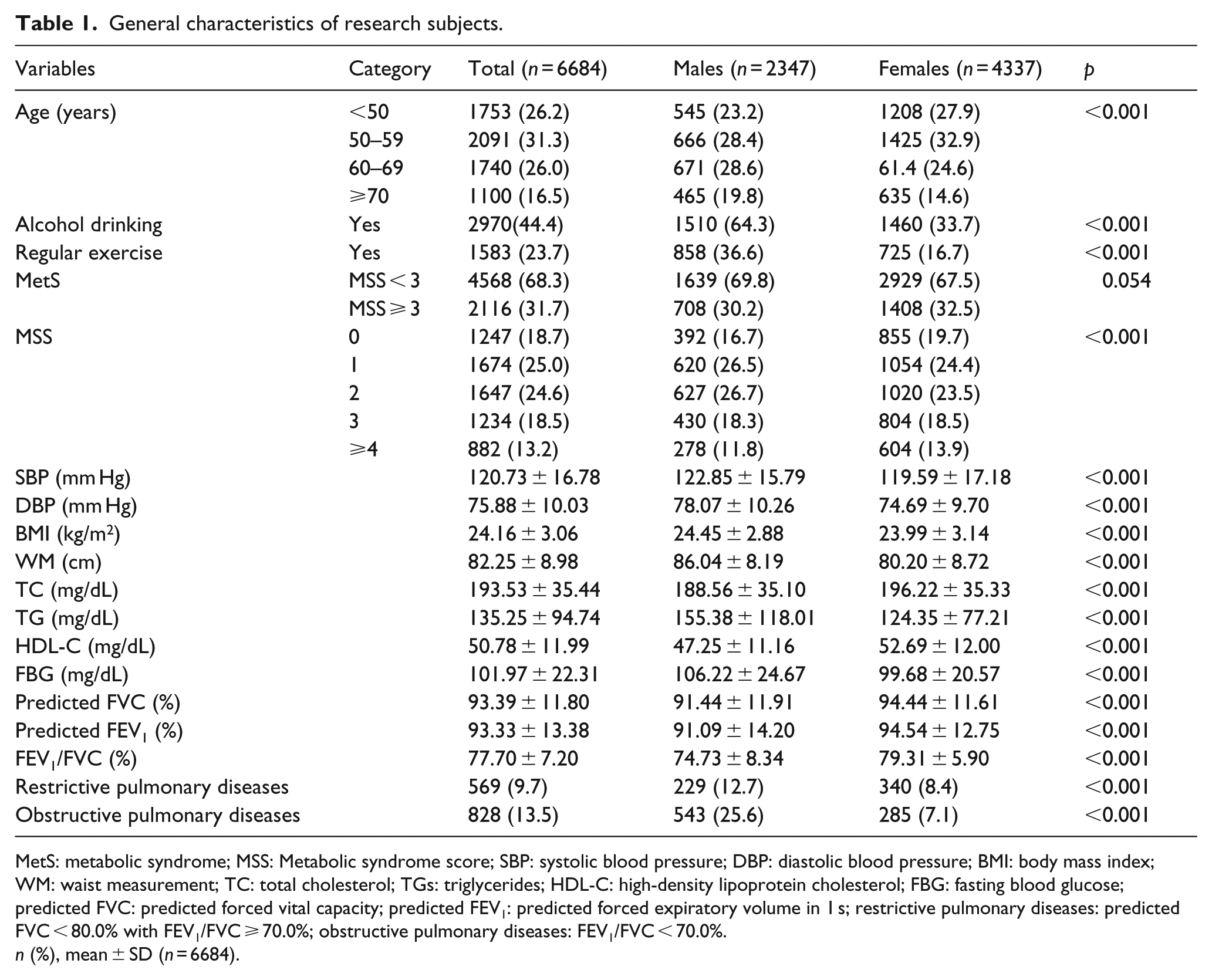
MetS: metabolic syndrome; MSS: Metabolic syndrome score; SBP: systolic blood pressure; DBP: diastolic blood pressure; BMI: body mass index; WM: waist measurement; TC: total cholesterol; TGs: triglycerides; HDL-C: high-density lipoprotein cholesterol; FBG: fasting blood glucose; predicted FVC: predicted forced vital capacity; predicted FEV1: predicted forced expiratory volume in 1 s; restrictive pulmonary diseases: predicted FVC < 80.0% with FEV1/FVC ⩾ 70.0%; obstructive pulmonary diseases: FEV1/FVC < 70.0%.
n (%), mean ± SD (n = 6684).
Comparisons of restrictive and OPDs and the predicted FVC and FEV1 values according to MetS characteristics
Comparisons of RPD, OPD, and the predicted FVC and FEV1 values according to the MetS characteristics are shown in Table 2. The mean predicted FVC was significantly lower in all reduced or elevated groups than in the normal group. The mean predicted FEV1 was significantly lower in abdominal obesity (p = 0.003), elevated BP (p = 0.013), elevated TGs (p < 0.001) and elevated FBG (p < 0.001) than in the normal group; however, the trend of reduced HDL-C (p = 0.178) in the former was not significant. The prevalence of RPD was significantly lower in abdominal obesity (p < 0.001), elevated BP (p < 0.001), elevated TGs (p = 0.009), reduced HDL-C (p = 0.001) and elevated FBG (p < 0.001) than in the normal group. The prevalence of OPD was significantly lower in elevated BP (p < 0.001) and elevated FBG (p < 0.001) than in the normal group; however, the increased abdominal obesity (p = 0.879), elevated TGs (p = 0.130) and reduced HDL-C (p = 0.345) in the former were not significant.
Comparisons of restrictive and obstructive pulmonary diseases and the predicted FVC and FEV1 values according to metabolic syndrome characteristics.
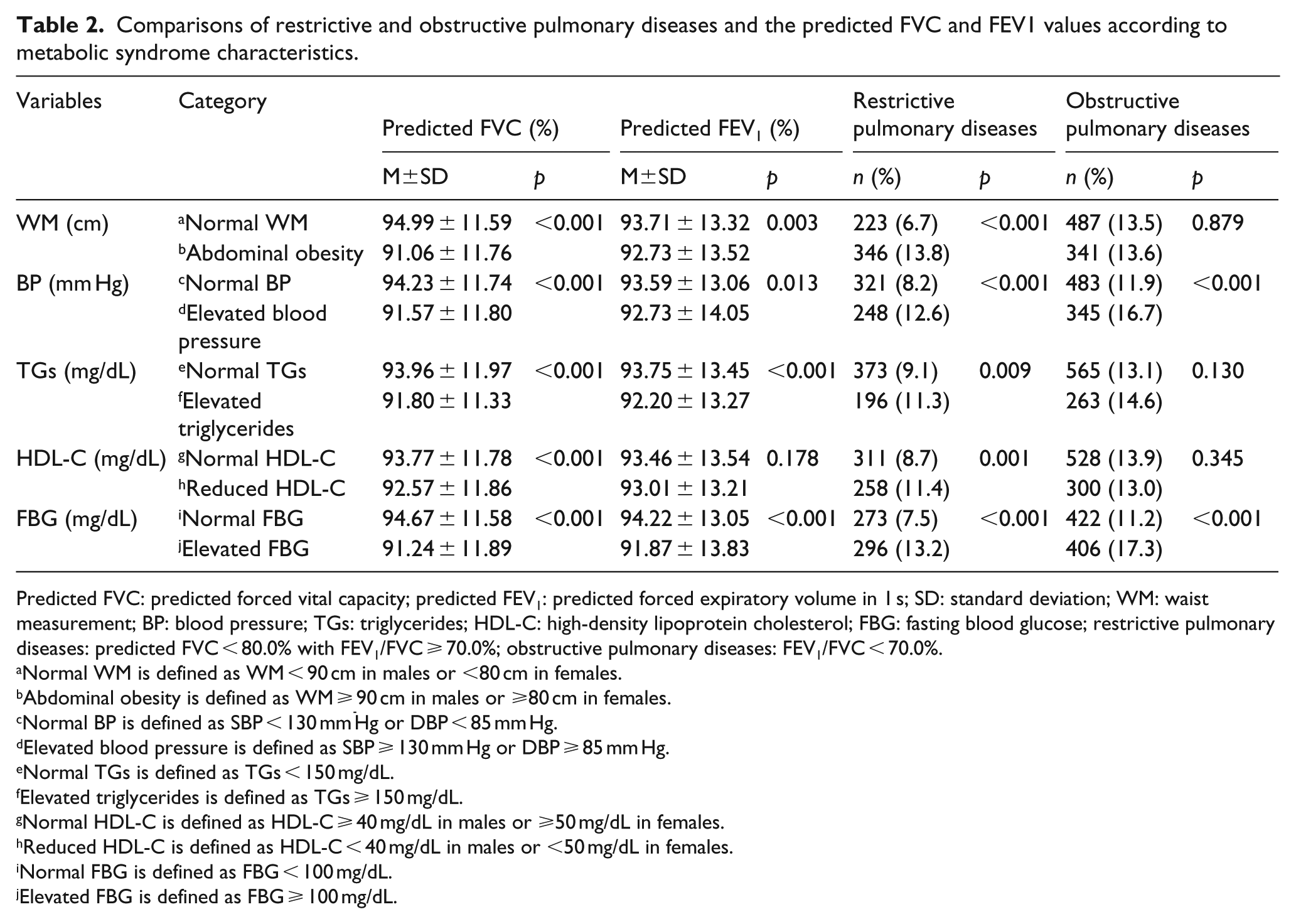
Predicted FVC: predicted forced vital capacity; predicted FEV1: predicted forced expiratory volume in 1 s; SD: standard deviation; WM: waist measurement; BP: blood pressure; TGs: triglycerides; HDL-C: high-density lipoprotein cholesterol; FBG: fasting blood glucose; restrictive pulmonary diseases: predicted FVC < 80.0% with FEV1/FVC ⩾ 70.0%; obstructive pulmonary diseases: FEV1/FVC < 70.0%.
Normal WM is defined as WM < 90 cm in males or <80 cm in females.
Abdominal obesity is defined as WM ⩾ 90 cm in males or ⩾80 cm in females.
Normal BP is defined as SBP < 130 mm Hg or DBP < 85 mm Hg.
Elevated blood pressure is defined as SBP ⩾ 130 mm Hg or DBP ⩾ 85 mm Hg.
Normal TGs is defined as TGs < 150 mg/dL.
Elevated triglycerides is defined as TGs ⩾ 150 mg/dL.
Normal HDL-C is defined as HDL-C ⩾ 40 mg/dL in males or ⩾50 mg/dL in females.
Reduced HDL-C is defined as HDL-C < 40 mg/dL in males or <50 mg/dL in females.
Normal FBG is defined as FBG < 100 mg/dL.
Elevated FBG is defined as FBG ⩾ 100 mg/dL.
Comparisons of restrictive and OPDs and the predicted FVC and FEV1 values according to MetS and MSS
Comparisons of the RPD, OPD and the predicted FVC and FEV1 values for MetS and MSS are shown in Figures 1 and 2 and Tables 3 and 4. After adjustment for related variables (age, gender, alcohol drinking, regular exercise and BMI), MetS (p < 0.001) and MSS (p < 0.001) were found to be inversely associated with the predicted FVC and FEV1 values (Figures 1 and 2). The ORs of OPD of MetS and non-MetS were not significantly different (Table 3). The ORs of RPD by MSS with MSS 0 as a reference group showed no significant difference for MSS 1 [1.061 (95% confidence interval (CI), 0.755–1.490)] and MSS 2 [1.247 (95% CI, 0.890–1.747)] but showed significant difference for MSS 3 [1.433 (95% CI, 1.010–2.033)] and MSS ⩾4 [1.760 (95% CI, 1.216–2.550)]. In addition, the OR of RPD of MetS [1.360 (95% CI, 1.118–1.655)] was significantly higher than of those of non-MetS (Table 4).
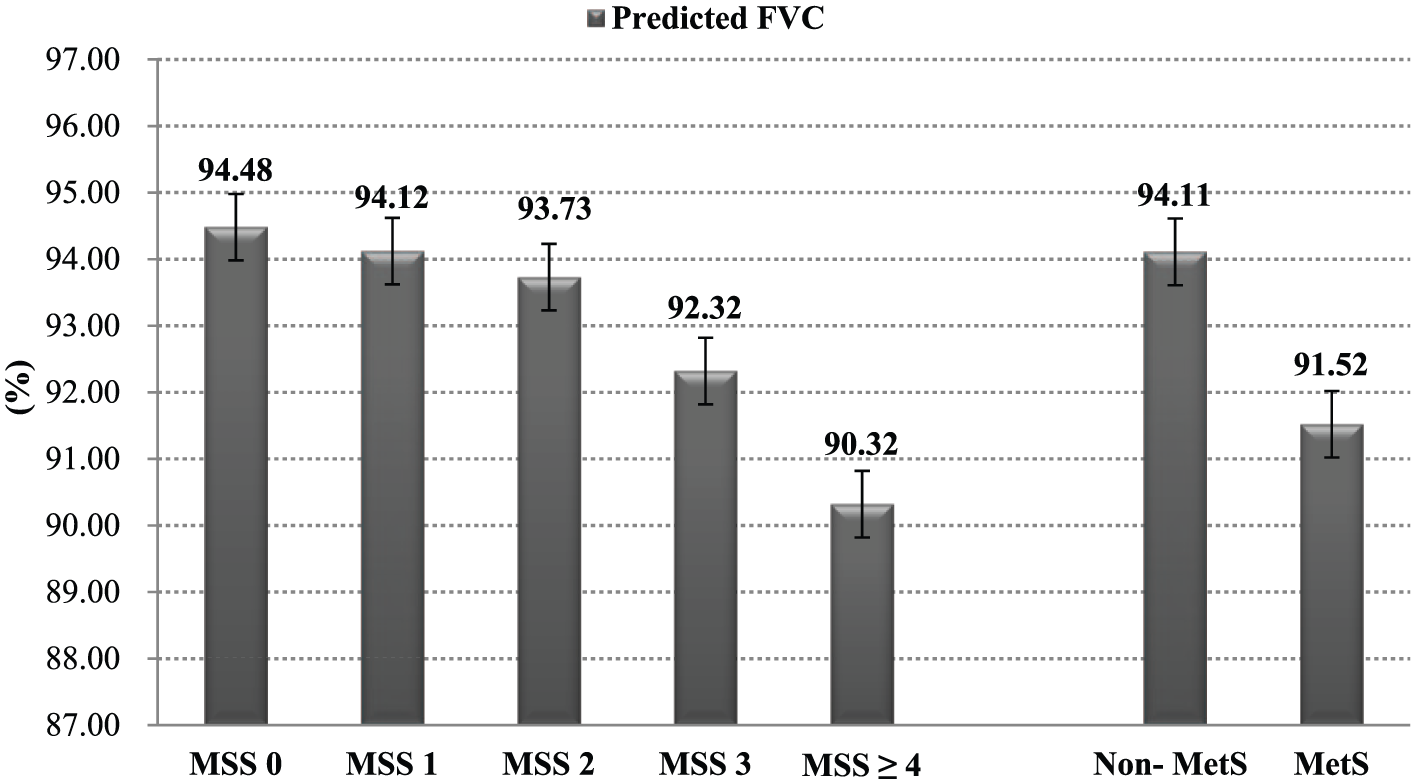
Comparisons of the predicted FVC according to MetS and MSS. Predicted FVC: predicted forced vital capacity; MetS: metabolic syndrome; MSS: metabolic syndrome score. After adjustment for related variables (age, gender, alcohol drinking, regular exercise and BMI), MetS (p < 0.001) and MSS (p < 0.001) were inversely associated with the predicted FVC.
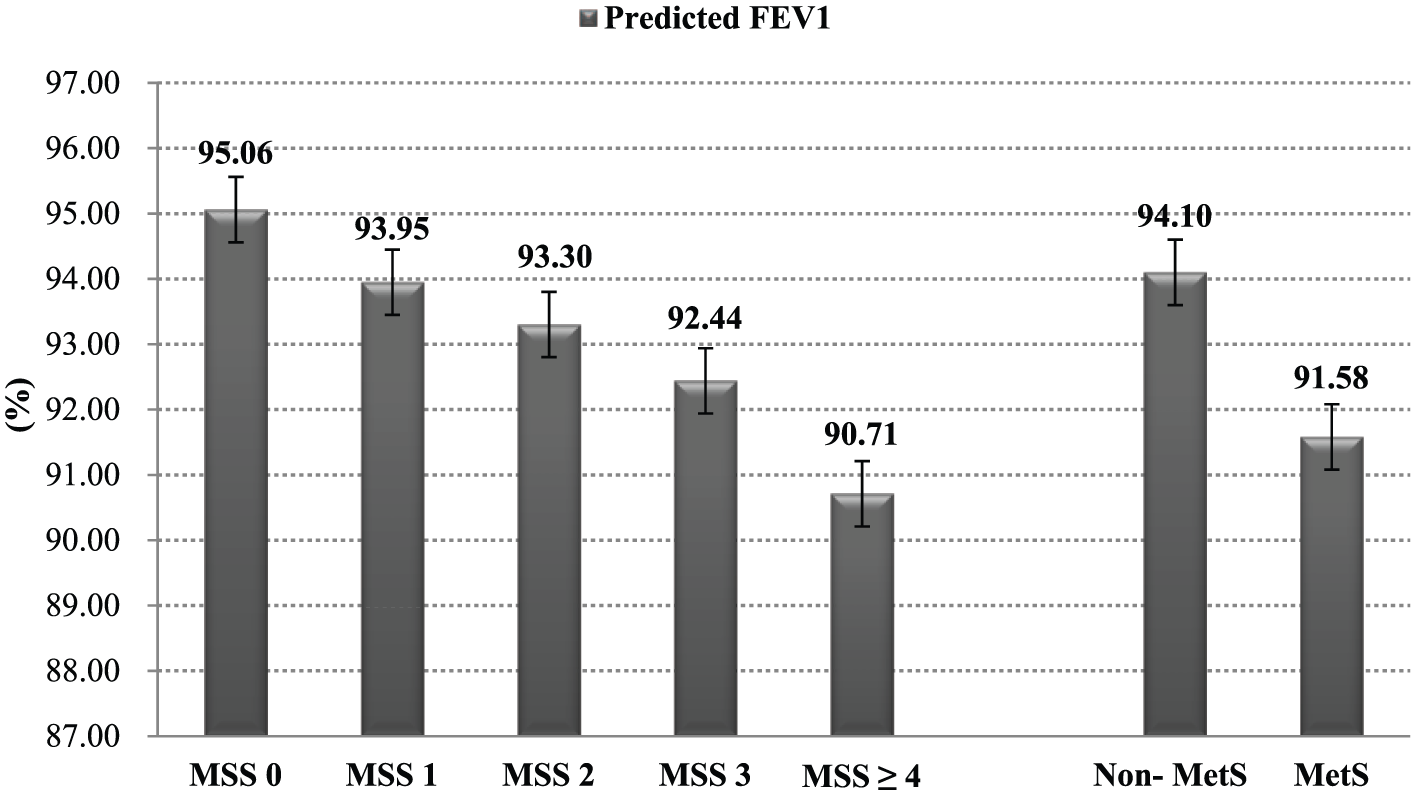
Comparisons of the predicted FEV1 according to MetS and MSS. Predicted FEV1: predicted forced expiratory volume in 1 s; MetS: metabolic syndrome; MSS: metabolic syndrome score. After adjustment for related variables (age, gender, alcohol drinking, regular exercise and BMI), MetS (p < 0.001) and MSS (p < 0.001) were inversely associated with the predicted FEV1.
Comparisons of the odds ratio of obstructive pulmonary diseases according to metabolic syndrome and metabolic syndrome score.
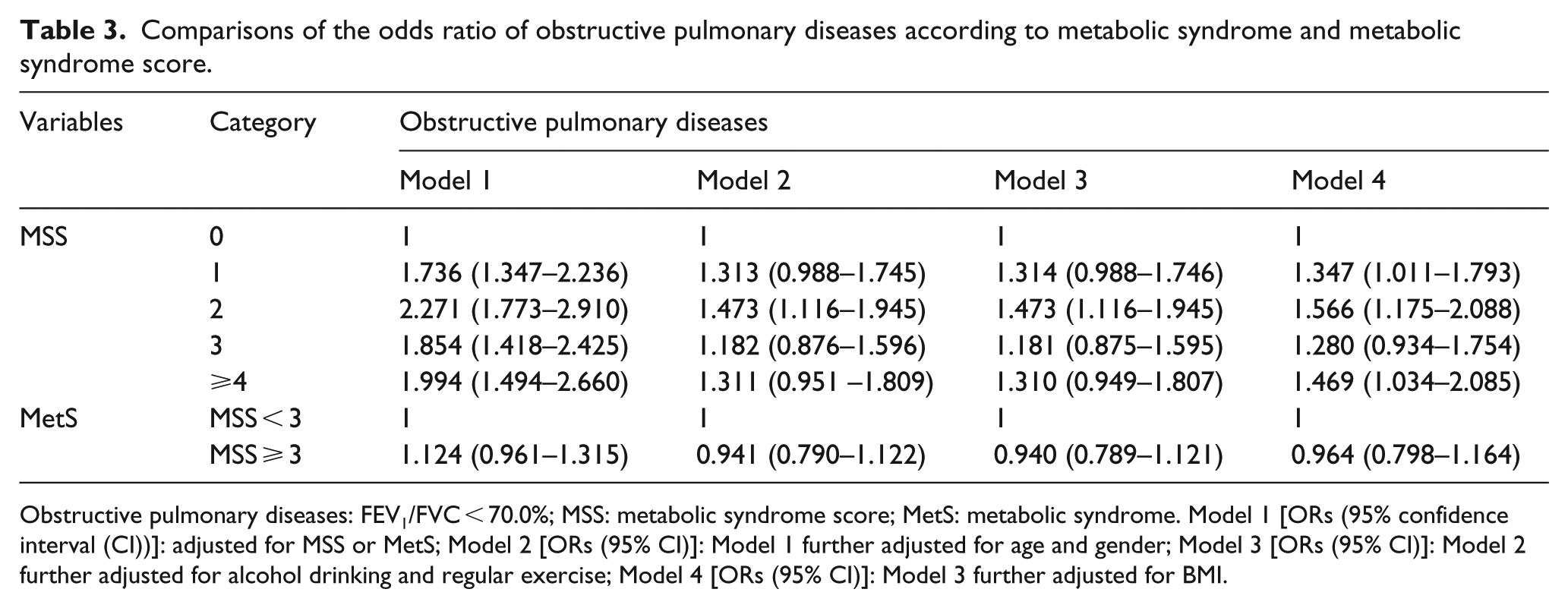
Obstructive pulmonary diseases: FEV1/FVC < 70.0%; MSS: metabolic syndrome score; MetS: metabolic syndrome. Model 1 [ORs (95% confidence interval (CI))]: adjusted for MSS or MetS; Model 2 [ORs (95% CI)]: Model 1 further adjusted for age and gender; Model 3 [ORs (95% CI)]: Model 2 further adjusted for alcohol drinking and regular exercise; Model 4 [ORs (95% CI)]: Model 3 further adjusted for BMI.
Comparisons of the odds ratio of restrictive pulmonary diseases according to metabolic syndrome and metabolic syndrome score.
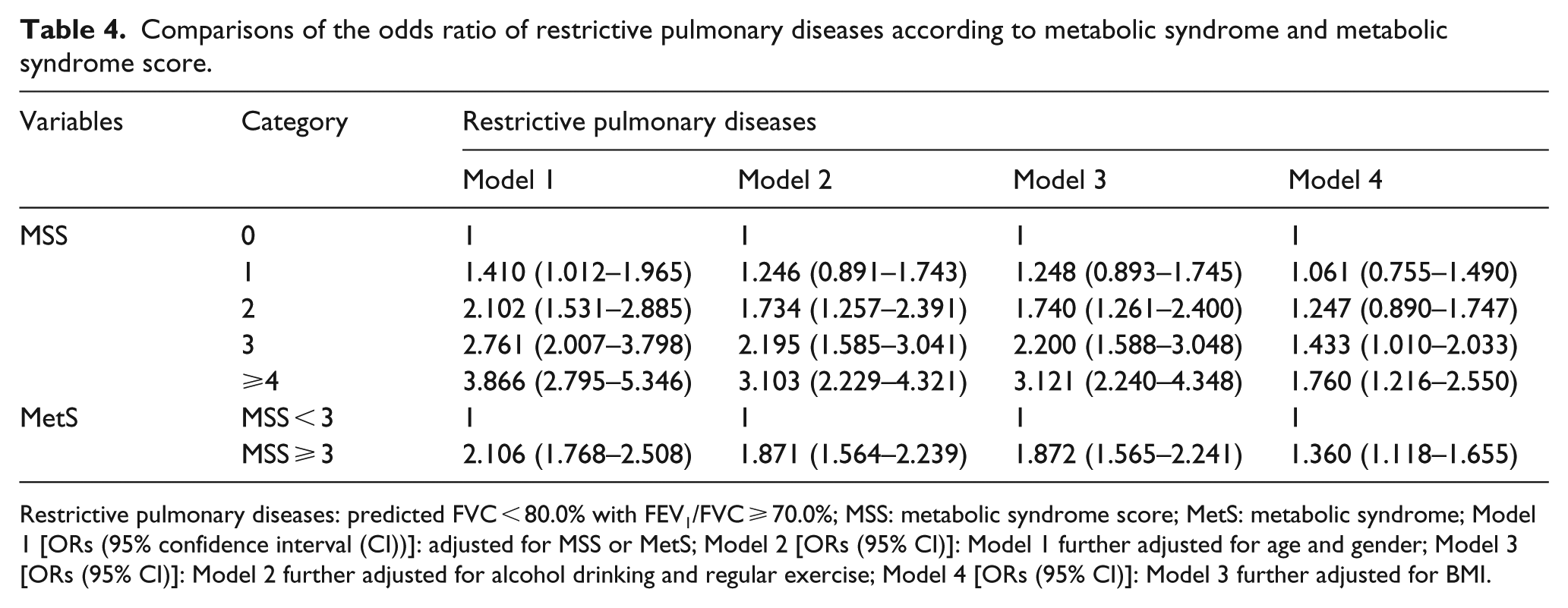
Restrictive pulmonary diseases: predicted FVC < 80.0% with FEV1/FVC ⩾ 70.0%; MSS: metabolic syndrome score; MetS: metabolic syndrome; Model 1 [ORs (95% confidence interval (CI))]: adjusted for MSS or MetS; Model 2 [ORs (95% CI)]: Model 1 further adjusted for age and gender; Model 3 [ORs (95% CI)]: Model 2 further adjusted for alcohol drinking and regular exercise; Model 4 [ORs (95% CI)]: Model 3 further adjusted for BMI.
Discussion
This study investigated the association of MetS and MSS with pulmonary function in Korean non-smoking adults using data from KNHANES-VI conducted in 2013–2015. After adjustment for related variables, MetS and MSS were positively associated with the RPD and negatively with the predicted FVC and FEV1 values. No significant association was found with OPD.
Among the studies conducted in non-smoking populations, the prevalence of MetS (31.7%) in our study was higher than in those of Takeuchi et al. 23 and Yu et al. 24 and lower than in those of Calo et al. 25 MetS is a chronic disease wherein abdominal obesity, hypertension, DM and dyslipidemia occur simultaneously, and each MetS component compromises pulmonary function. Regarding the association between MetS components and pulmonary function, Ochs-Balcom et al. 26 reported that abdominal obesity is the independent risk factor of pulmonary function decreases. In addition, they suggested that abdominal obesity is a better predictor of compromised pulmonary function than BMI. Regarding the association between dyslipidemia and pulmonary function, some studies reported that dyslipidemia is a strong independent risk factor of pulmonary function decreases.27–29 Esteve et al. 29 reported that dyslipidemia is associated with activation of the inflammatory cascade, and they suggested that activation of the inflammatory cascade could explain the effect of dyslipidemia in the development of pulmonary diseases. DM affects lungs causing restrictive type of ventilatory changes probably because of glycosylation of connective tissues, reduced pulmonary elastic recoil and inflammatory changes in lungs. 30 In particular, the restrictive pattern becomes more prominent with DM progression. 31 Finally, regarding the association between hypertension and pulmonary function, some studies have reported an association;6,32 however, the direct link between these remains unclear.
Currently, there is little research on the association between MetS components and pulmonary function in non-smokers. The association between each MetS component and pulmonary function decreases in non-smokers may vary. However, in this study, if a MetS component was present, compromised pulmonary function was observed. Rogliani et al. 33 reported that FVC and FEV1 were not associated with WM, TGs and FBG in Italian non-smokers but were inversely associated with MetS. In addition, Lim et al. 34 reported that FVC and FEV1 were not associated with SBP, DBP, TGs and HDL-C in Korean non-smoking males but MetS was inversely associated with pulmonary function. In this study, the predicted FVC values (all reduced or elevated groups) and predicted FEV1 (all elevated groups except the reduced HDL-C group) were significantly lower in all abnormal groups than in the normal group. Furthermore, the predicted FVC and FEV1 values were lower in non-MetS than in MetS.
Among research on the association between MetS and pulmonary diseases, most previous studies reported an association between MetS and RPD; however, the results of the association between MetS and OPD varied by country. Ford et al. 35 reported that RPD [OR, 1.47 (95% CI, 1.27−1.70)] was associated with MetS in the United States, whereas OPD was not. Marquis et al. 36 reported that RPD [OR, 1.221 (95% CI, 1.086−1.327)] was significantly associated with MetS in Taiwanese, whereas OPD was not. However, some studies have reported an association between MetS and OPD. Leone et al. 37 reported that MetS was associated with both RPD and OPD. Ghatas 38 reported that MetS was associated with the OPD, particularly in early stages (GOLD stages I−II). In addition, Park et al. 39 reported that the association between MetS and OPD differed by the sex: men, 2.03 (95% CI, 1.08−3.80)]; women, 1.44 (95% CI, 0.62−3.34).
In this study conducted in non-smokers, RPD was significantly associated with all MetS components. In addition, the ORs of the RPD were significantly increased in only MSS 3 and MSS ⩾ 4. However, OPD was associated with elevated BP and FBG among the MetS components, and ORs of OPD were significantly increased in MSS 1, MSS 2 and MSS ⩾4. Therefore, because MetS was identified as exhibiting more than three out of the five MetS components, MetS was associated with RPD but not with OPD.
RPD can have various aetiologies, including diseases such as congestive heart failure, interstitial lung disease, systemic inflammation, as well as DM and obesity, which are the risk factors of MetS. 40 In addition, MetS is characterized by insulin resistance, and some studies have reported that insulin resistance is a key association between RPD and MetS.41,42 In this study that included non-smokers, MetS was positively associated with RPD, and one of these reasons is that RPD increases as MSS increases.
However, there are several limitations of our study. First, C-reactive protein (CRP) and homeostatic model assessment of insulin resistance (HOMA-IR) are important determinants of the association between MetS and pulmonary function; however, these were not measured in KNHANES-VI study and thus could not be included as factors in our study. Therefore, we could not determine the relationship of pulmonary function with HOMA-IR and C-reactive protein, and these could not be used as adjustment variables. Second, because this was a cross-sectional study, the scope of establishing a causal relationship of MetS and MSS with pulmonary function was limited. Although this study has these limitations, this is, to our knowledge, the first reported study to determine the association of MetS and MSS with pulmonary function in Korean non-smoking adults. Therefore, more accurate results may be obtained by performing a cohort study that also includes CRP and HOMA-IR as variables.
In conclusion, this study investigated the association of MetS and MSS with pulmonary function in Korean non-smoking adults using data from KNHANES-VI conducted in 2013–2015. MetS and MSS were inversely associated with the predicted FVC and FEV1 values in Korean non-smoking adults. In addition, MetS and MSS were positively associated with RPD.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.