
Abstract
Background:
UK cardiac rehabilitation has reached for the first time 50% uptake in 2016; however, this still leaves 50% of the eligible group not starting cardiac rehabilitation. The characteristics of patients missing cardiac rehabilitation are relatively unknown with some studies in America suggesting that patients with diabetes have a reduced likelihood of joining cardiac rehabilitation.
Methods:
This study used routinely collected data from the National Audit of Cardiac Rehabilitation to investigate proportional differences in patients with cardiovascular disease with, and without, diabetes taking up the offer of cardiac rehabilitation.
Results:
The proportion of patients with diabetes entering cardiac rehabilitation dropped by between 7% and 15% depending on the age group (<40 years, 7% reduction; 61–80 years, 15%). The study’s results showed that in all demographic and diagnostic groups, the proportion of patients with diabetes was significantly less than that of the eligible group (p < 0.001). There was no difference in the proportion of loss, from eligible to starting cardiac rehabilitation, between males and females, which was 13% for both groups.
Conclusion:
This study confirms, in a new UK population with over 121,002 eligible patients, that there is a statistically significant drop in patients with diabetes taking up cardiac rehabilitation. This study is unique in looking at all four key diagnosis and treatment groups and comparing them to those taking up cardiac rehabilitation. To achieve the target of 65% uptake set by NHS England, improvements in identifying and targeting complex patients, such as those with diabetes, need to be adopted.
Introduction
Cardiac rehabilitation (CR) is a widely recognised and effective intervention post-cardiovascular disease (CVD) that has been evidenced to reduce cardiovascular mortality [risk ratio (RR) = 0.74, 95% confidence interval (CI) = 0.64–0.86], overall mortality [hazard ratio (HR) = 0.37, 95% CI = 0.20–0.69] and hospital readmission (RR = 0.82, 95% CI = 0.70–0.96).1,2 Patients benefit from CR in a variety of areas from a reduction in lifestyle risk factors, improved mental well-being and overall physical health.
Nationally in the United Kingdom, uptake to CR has gradually improved from ~40% over the past 4 years to achieve 50%, which puts UK CR within the top 2% of countries in Europe.3,4 The new uptake figures signify a real success in the UK CR programmes, bringing the uptake closer to the 65% target set by NHS England 5 in 2014. Although CR uptake is increasing, evidence suggests that some demographics of patients are not taking up the offer; these include unemployed patients, older and female patients.6–8
The population who are taking up CR have a variety of different comorbidities including angina, hypertension and diabetes. 3 Patients with CVD often have type 2 diabetes as well; the two conditions within the literature are closely associated.9,10 Patients with diabetes (PWD) have an increased risk of CVD, patients post-myocardial infarction (MI) have higher long-term mortality risk than the patients without (PW) and 80% of all deaths in diabetes are from cardiovascular events.11,12 Alongside the evidenced link between diabetes and CVD, there are also 30% of PWD in CR programmes with a multi-morbid profile. 3
CR in the United Kingdom is defined by the BACPR core components, which states that patients broader than typical patients with CVD should be attending rehabilitation, specifically mentioning PWD. 13 The risk factor management involved in CR is shared with those in diabetes, such as blood pressure management, weight control, physical activity/capacity and healthy diets.
Dunlay et al.’s 7 2009 study looked at patients with MI who were taken up to CR in the United States; they also considered whether patient’s comorbidities affected their uptake. The study population had 23.5% PWD, who were less likely to take part in CR than PW [odds ratio (OR) = 2.50]. This study is supported in their conclusions by additional work by Motivala et al. 14 This study concluded that high-risk patients, which included diabetes as a demographic, were less likely to receive a variety of CVD interventions/treatments such as aspirin, beta-blockers and CR. 14 These studies were in the United States, and either contained a relatively small sample or were looking at overall risk rather than patient’s diabetes status specifically.
The aim of this study is to, using routinely collected audit and Hospital Episode Statistic (HES) data, identify differences in uptake of patients with and without diabetes. Additionally, the study will consider sub-groups of the eligible population to identify whether there are differing uptake levels of PWD across age groups, cardiovascular diagnosis/treatment and gender.
Methods
This study was reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 15
Data
The analyses used routinely collected patient-level data from the UK National Audit of Cardiac Rehabilitation (NACR) and the eligible CR population in Hospital Episode Statistics (HES) database from 1 April 2014 to 31 March 2015. The two datasets are routinely used each year to help produce the NACR annual report.
The HES data are processed annually to calculate the eligible population for CR, and thus uptake across four main diagnosis/treatment groups, which for the first time, has reached 50% in total. 3 The data also record patient’s comorbidities and other conditions, such as diabetes. The data were coded to identify PWD and PW within the eligible population. Patients were identified as eligible if they had one of the included diagnosis/treatment codes and were discharged from hospital alive.
The NACR data contain information on patient’s initiating event, treatment, individual risk factors, medication use, characteristics and outcomes post rehabilitation. Data are collected under 251 approval, which is reviewed annually by NHS Digital. Within the NACR dataset, there are records of patient’s comorbidities. Due to the coding of the NACR, the diabetes status was binary, based on whether the patients had a comorbidity of diabetes or not, it was not possible to split out type 1 or 2. Patients were coded according to their initiating event/treatment from the HES data, along with whether or not they had diabetes. Patients were classified as being taken up to CR, if they were entered in the NACR data and had a valid start date of CR within 1 April 2014 to 31 March 2015.
The two datasets will be used to compare demographics across the two groups, which will identify whether there are barriers to entry for PWD in CR. The demographics will include patient’s diagnosis/treatment along with age groups and gender, known to be themselves barriers to entry for patients.
Statistical analysis
The analyses were conducted using Stata 14. The probability of a patient being taken up to CR was assessed using one sample test of proportion. The z-score was set at −1.96 to 1.96 as the parameter for accepting differences between our test population and eligible proportion; statistical significance is set at p < 0.05. The proportion of PWD to PW in each dataset would remain constant if there were no barriers to entry for either groups. The four main diagnosis/treatment groups reported in the uptake calculation annually along with gender and age groups were used to split the eligible population for the analysis. The age groups were generated from the age at which the patient’s event occurred. The age groups were chosen to split younger (<40 years) and older patients (80+ years), along with the large middle-aged group (41–60 and 61–80 years) as defined in the Cochrane Review of CR which is 49–70 years. 8
Results
This study population, shown in Table 1, included 121,002 patients identified as eligible from the HES data; within this population, 26% were PWD. The number of patients who started CR and were entered into the NACR was 32,663 total patients, of which 14% had a comorbidity of diabetes. In the four diagnosis/treatment groups, the proportion of PWD is similar, with coronary artery bypass grafting (CABG) having the highest percentage in both eligible and receiving populations. The lowest proportion of PWD was in the eligible MI/percutaneous coronary intervention (PCI) group, which transferred to the receiving population also. Across the four age groups, the proportion of PWD increases from <40 to 41–60 years by 13% and then to 61–80 years by 4%; however, in the 80+ years group, there was less eligible PWD than either 41–60 or 61–80 years.
Proportions of PW/PWD in the eligible and starting CR groups, split by diagnosis/treatment, gender and age.
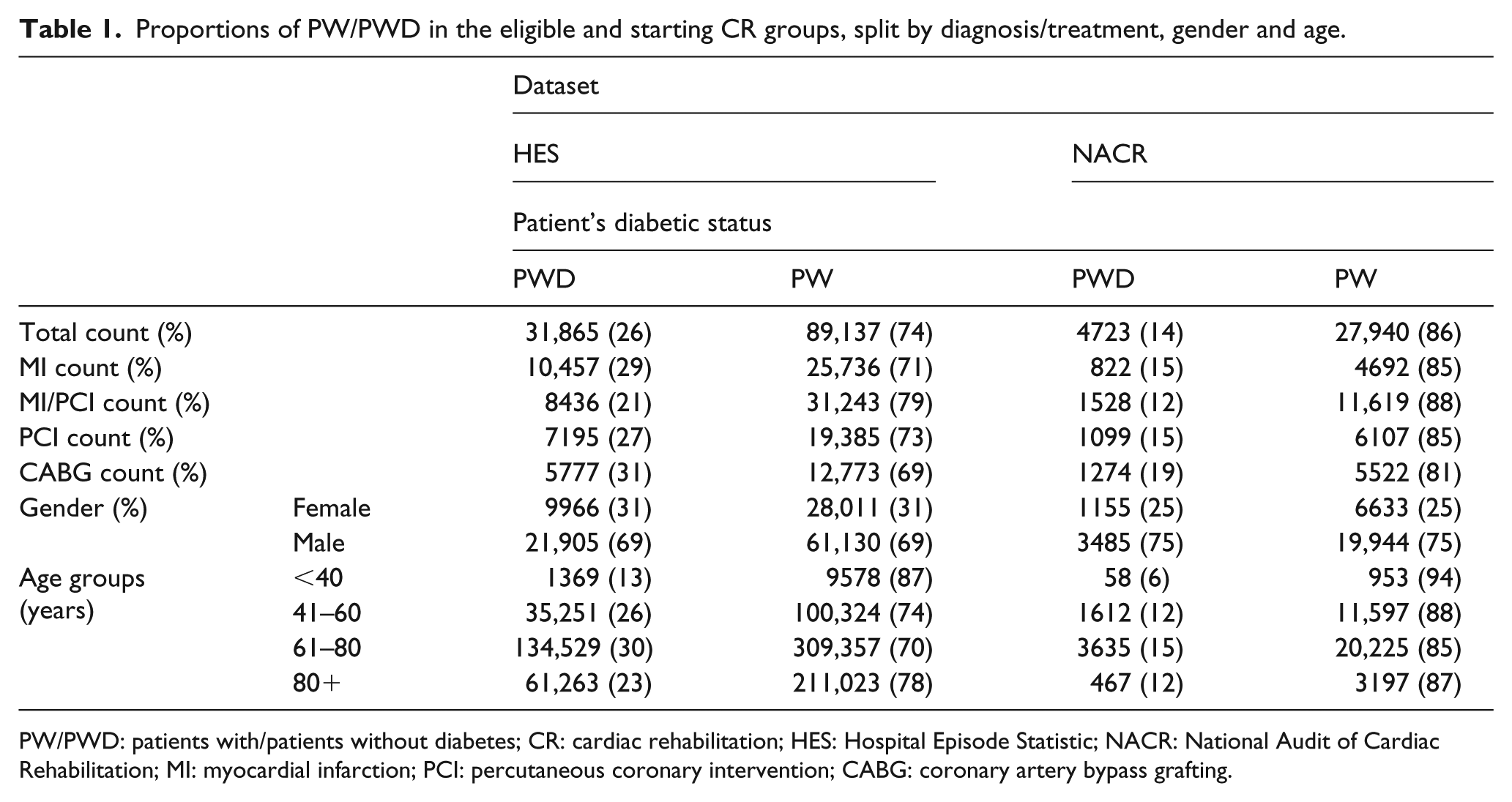
PW/PWD: patients with/patients without diabetes; CR: cardiac rehabilitation; HES: Hospital Episode Statistic; NACR: National Audit of Cardiac Rehabilitation; MI: myocardial infarction; PCI: percutaneous coronary intervention; CABG: coronary artery bypass grafting.
The proportion of PWD in the male and female eligible groups was 31%; this proportion dropped by 6% by the time patients reached CR which was similar in PWD and PW. This suggests that across PWD and PW, there seems to be no difference in gender uptake for diabetes. The proportion of PWD across the eligible age groups varied between 12% and 30%, with the 61–80 years group having the largest percentage. Across all age groups, there is a significant drop in the proportion of PWD of 7%–15%; this is strongest in <40 years group which has greater than 50% of the eligible PWD not taking up CR, followed closely by 61–80 years with 50% reduction.
The statistical tests included in this study were comparing the proportion starting rehabilitation to the constant deemed as the eligible proportion of PWD. Table 2 shows that in every grouping tested, PWD have a statistically different population to that of the eligible group. The z-scores in Table 2 are all smaller than 1.96, ranging from −6.5 to −49.4. The p-values are all <0.001, likely due to the sample size, however, the extent of the drop in each group, shown by the results in Table 1, signifies a high level of clinical significance.
Z-scores of PWD and PW across the two populations.
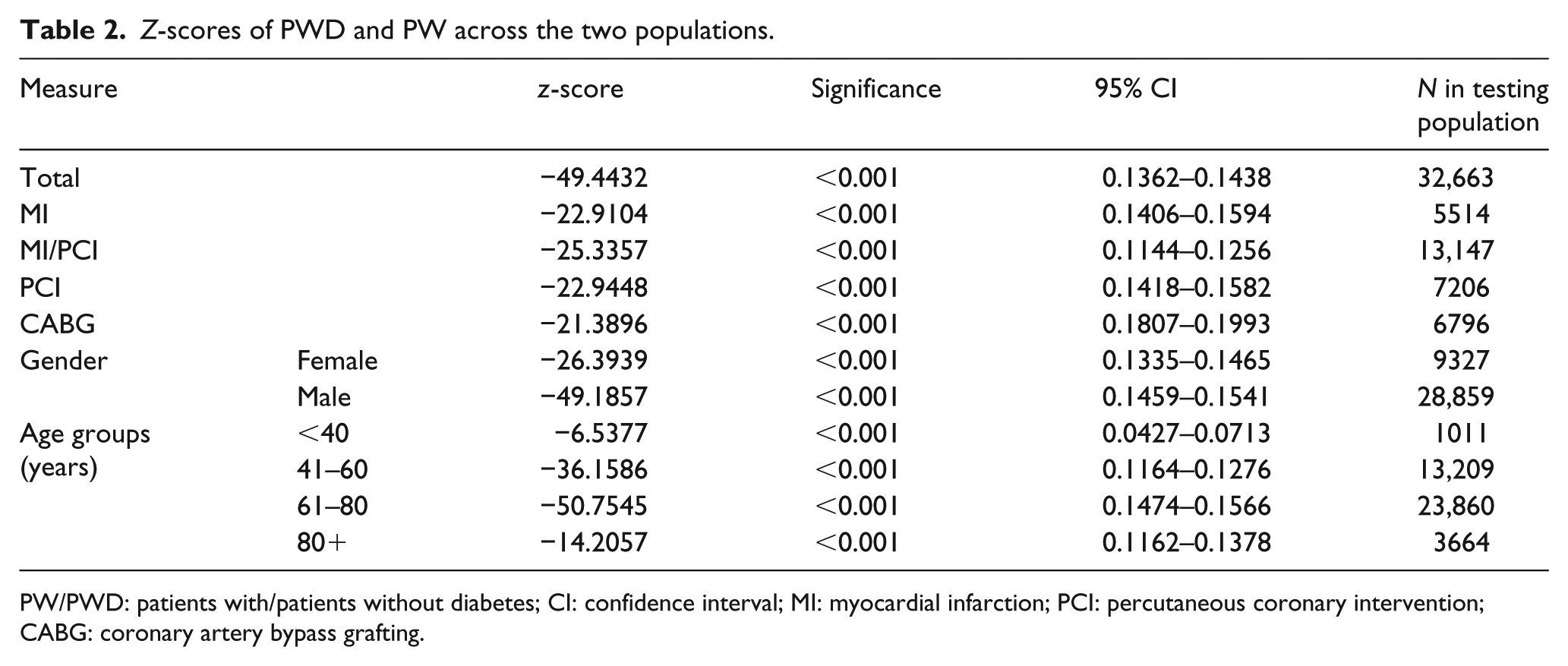
PW/PWD: patients with/patients without diabetes; CI: confidence interval; MI: myocardial infarction; PCI: percutaneous coronary intervention; CABG: coronary artery bypass grafting.
Discussion
The aim of this study was to consider the uptake of patients into CR, specifically whether patient’s comorbidity of diabetes is a factor. Based on the evidence, a patient having diabetes is a strong factor that affects uptake to CR. Regardless of the patient’s diagnosis/treatment, age or gender, there seems to be a strong relationship between patients having diabetes and not taking up the offer of CR. The results of this study support other work in the area, such as Dunlay et al. 7 and Motivala et al.; 14 however, this is the first study considering UK CR and diabetes uptake, and also is utilising more patients than these studies.
The drop in total PWD from the eligible group is 12%, in some sub-groups as high as 15% reduction. If there were no barriers to entry, then this proportion of the population would stay the same. The statistical analysis showed that this proportional change was statistically significant. The study showed that the reduction in the proportion of PWD was the same for both genders; this might suggest that across genders, there are equal barriers to entry for PWD.
In the age groups, there was a similar reduction in uptake with the eligible PWD proportion halving by the time they reached rehabilitation, suggesting that in all age groups, diabetes is a barrier for entry. It was worth noting that there was less PWD in the eldest age group, which may be done to the reduced survival chances in older patients when they have diabetes as a comorbidity.
This study is of considerable importance to CR providers and commissioners. Evidence shows that PWD who have an MI event are at higher risk of a further event than those PW; however, control of risk factors in PWD can reduce the risk of events such as MI, blood pressure control showed a reduction of risk by a fifth. 16 This provides a strong incentive for PWD to attend CR to reduce their risk and their burden on the NHS. The prevalence of diabetes is increasing each year, with the cost to health services to follow suit.17,18 This evidence suggests that more work needs to be done, in making CR more attractive for PWD, which in turn can reduce the financial burden.
The benefits from attending CR are extensively shared across CVD and diabetes, from reducing blood pressure, improvements in physical activity and education about diet. This study did not set out to assess the effectiveness of CR in PWD, moreover, to address whether there is evidence that in the United Kingdom, there are barriers for PWD.
Limitations
The main limitation of this study is the level of analysis. Due to the nature of access to this data, it was not possible to link between the eligible and starting populations. This resulted in analysis of proportions in groups and sub-groups being used. Future work will aim to, through linking of the two groups, assess whether there is an interaction of likelihood of taking part in CR and age, gender, diagnosis/treatment and other known barriers such as employment state, deprivation and education level.7,8,19,20 One factor that is evidenced to affect uptake to health-care services is other comorbidities in PWD. Although the analysis was a limitation for the more complex question of uptake in CR, we feel that it provided sufficient evidence to address whether there are barriers to entry for PWD.
Another piece of work will build on the results here by comparing in more detail whether the PWD population who take up the offer are different to wider PW population. If there is a difference between the two groups, it may be important to tailor CR for PWD if they are more multi-morbid or older.
Conclusion
This is the first study in the United Kingdom, using routinely collected data, to investigate the relationship between patients having diabetes and their participation in CR. This study has evidenced that there are barriers to PWD taking part in CR, with a reduction of 12% of eligible patients by the time CR starts. With CR in the United Kingdom reaching world leading levels of uptake, the hard-to-reach patients may need more tailoring to reach the 65% target set by NHS England. This article concludes that as well as older and female patients, another group who is missing out on beneficial CR is those with diabetes. Innovation to make CR more appealing to PWD needs to be investigated.
Footnotes
Acknowledgements
The authors acknowledge the support of the NACR team.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was carried out by the British Heart Foundation (BHF) Cardiovascular Care and Education Research Group, which is supported by a grant from the BHF (R1680901).