
Abstract
Objectives:
The purpose of this study is to report the efficacy of endovascular treatment for patients with sub-acute (14-day to 2-month) deterioration of chronic lower extremity ischaemia.
Materials and Methods:
Between June 2013 and May 2015, 26 consecutive patients (22 men, 4 women; mean age, 68.6 years; range, 50–86 years) were treated for sub-acute deterioration of chronic lower extremity ischaemia in our hospital. All patients were treated with catheter-directed thrombolysis initially and then adjunctive percutaneous transluminal angioplasty and/or stenting was performed to correct underlying lesions.
Results:
The 26 intra-arterial thrombolysis procedures were all performed in native lower arteries including 8 iliac, 13 femoropopliteal and 5 diffuse occlusions involving the iliac and femoropopliteal segments. Lesion length decreased from 194 mm (70–350 mm) to 92 mm (20–270 mm) after the thrombolytic procedures, and the residual lesions were corrected with percutaneous transluminal angioplasty alone in 4 (15.4%) limbs and stenting in 22 (84.6%) patients. No cross-joint stenting was seen in the 22 affected limbs that used stents. Throughout the treatment process, nine patients with intermittent claudication achieved an unrestricted walking distance, and 17 patients with rest pain or foot ulcers showed significant symptom improvement. The mean ankle-brachial index increased from 0.42 ± 0.16 preoperatively to 0.81 ± 0.25 postoperatively (p < 0.01).
Conclusion:
Endovascular therapy with catheter-directed thrombolysis and percutaneous transluminal angioplasty/stenting is feasible for sub-acute deterioration of chronic lower extremity ischaemia patients with favourable midterm results.
Introduction
Sub-acute (14-day to 2-month) deterioration of chronic lower extremity ischaemia (DCLEI) in patients with peripheral artery disease (PAD) is often associated with relatively fresh thrombotic components within the primary occlusion.1–3 The patients may be characterized by severe claudication, rest pain or foot ulcers that often require surgical intervention.
Surgical reconstruction has been considered as the standard therapy for these sub-acute DCLEI patients. Compared to surgical bypass, endovascular therapy has been considered the initial choice for chronic lower extremity ischaemia based on its minimally invasive alternative nature, particularly in elderly high-risk patients. However, directing endovascular treatment such as balloon angioplasty and/or stent placement may result in the downwards movement of the clot to the distal artery. 4
Catheter-directed thrombolysis (CDT) has been accepted as an effective method to dissolve acute 5 and sub-acute6,7 clots by increasing the surface area available for enzymatic action. CDT therapy may eliminate the thrombotic or embolic material and then adjunctive endovascular intervention restores perfusion of lower extremity. 8 Considering the relative fresh thrombi of these sub-acute DCLEI patients, we could unmask the much less severe underlying lesions using CDT.
The aim of this study was to assess the efficacy of thrombolytic treatment combined with adjunctive percutaneous transluminal angioplasty (PTA) and/or stenting for 26 sub-acute DCLEI patients over the past 2 years.
Methods
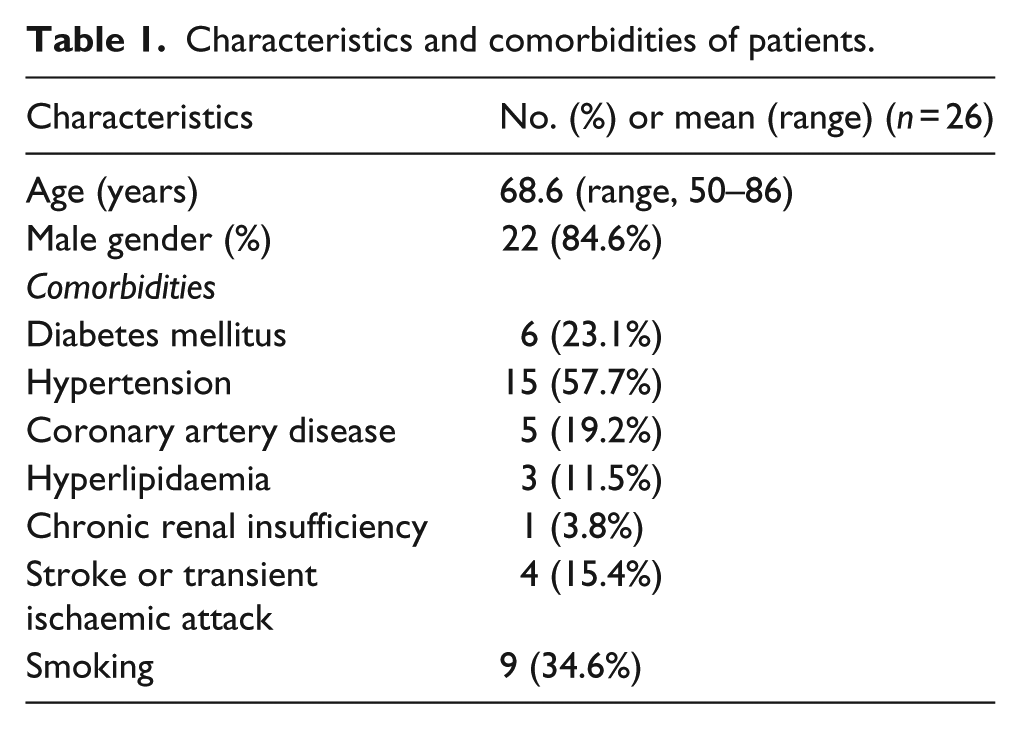
Between June 2013 and May 2015, of a total of 263 de novo lower extremity ischaemia cases enrolled, 26 consecutive patients (22 men, 4 women; mean age, 68.6 years; range, 50–86 years) were treated for sub-acute DCLEI in our hospital. Patients were included if they had chronic lower extremity ischaemia with intermittent claudication (R2 or R3) and developing sub-acute deterioration with the time window from 14 days to 2 months. They were excluded if they had one or more of the following: (1) receiving surgery previously for low extremity artery disease (open or endovascular treatments), (2) thromboangitis obliterans, (3) lesions involving the aorta, (4) acute lower extremity ischaemia (<14 days’ duration), (5) nephrotic syndrome, (6) digestive tract haemorrhage, (7) active bleeding during the past 3 months (such as major surgical operation, severe injuries), (8) stroke history within 6 months and (9) serious or unmanageable hypertension. Patient comorbidities included diabetes mellitus, hypertension, coronary artery disease, hyperlipidaemia, chronic renal insufficiency, stroke and smoking (Table 1). Cessation of tobacco use, walking exercises and conservative medication regimens including aspirin, cilostazol and statins were tried prior to the sub-acute deterioration, but without significant clinical improvement.
Characteristics and comorbidities of patients.
A pre-procedural assessment was performed in all the patients using computed tomography angiography, magnetic resonance angiography or colour Doppler ultrasonography. Lesion location, lesion length, proximal occlusion level and distal runoff vessels were evaluated. The protocol of this study was carried out according to the principles of the Declaration of Helsinki and approved by the Medical Ethics Committee in Shanghai Changhai Hospital. Written informed consent was obtained from each patient after a detailed explanation of the risks and benefits of the thrombolytic therapy and adjunctive treatments.
Under local anaesthesia, arterial access was obtained using a percutaneous retrograde femoral approach in all patients with a 6-F cross sheath (Cook Medical, Bloomington, IN, USA). Initial digital subtraction angiography was performed to determine the affected limb inflow, lesions and outflow. A hydrophilic guide wire (Terumo, Tokyo, Japan) was then crossed through the occluded thrombus intraluminally, and a selected multi-side-hole thrombolytic catheter (AngioDynamics, NY, USA) was navigated over the guide wire into the thrombus according to occlusion length. The thrombus was then reconfirmed via angiography through the thrombolytic catheter (Figure 1).
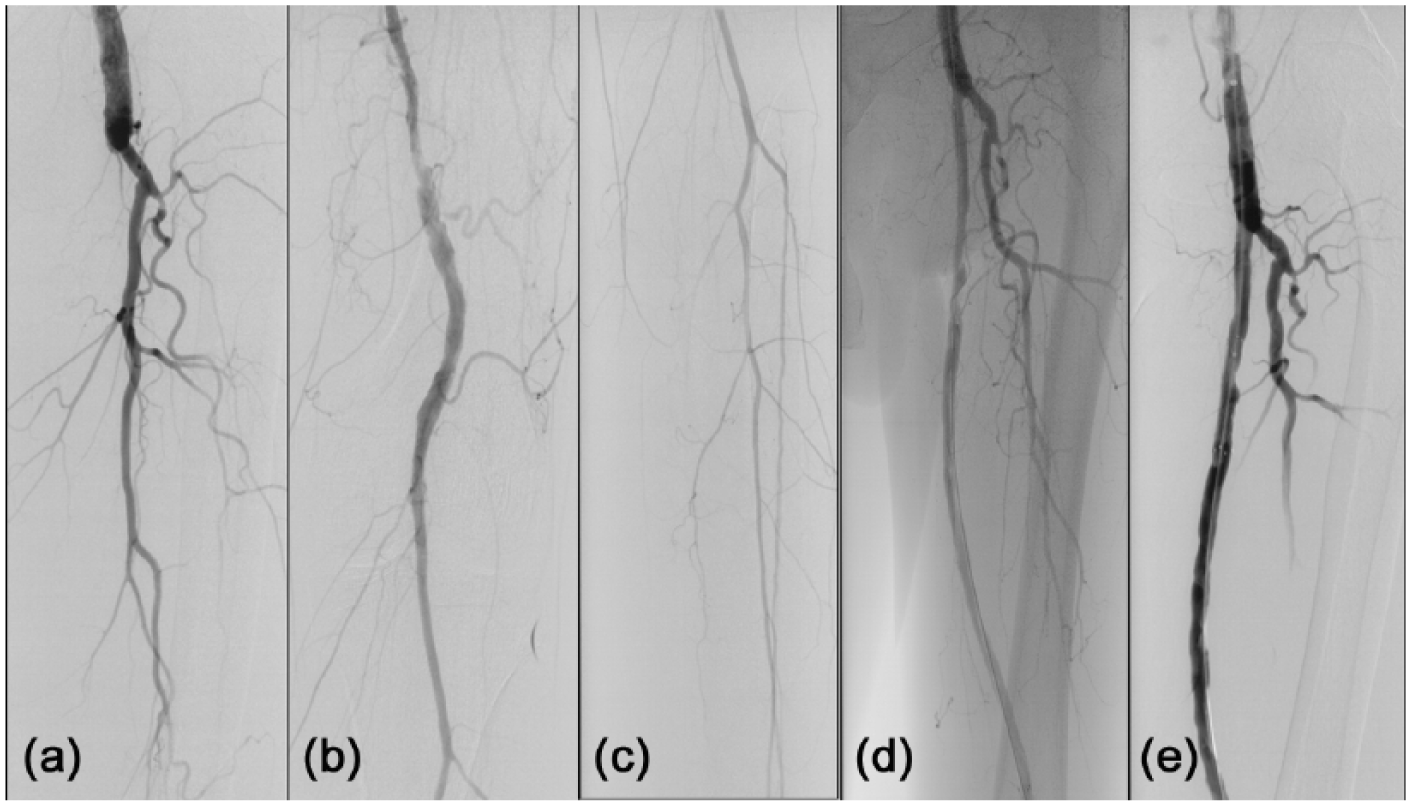
A 63-year-old male patient presented with severe claudication of the left leg that worsened over the 26 days prior to presentation. (a, b) Digital subtraction angiography demonstrated occlusion of proximal superficial femoral artery (SFA) and stenosis of the distal SFA. (c) Infrapopliteal angiography showed anterior tibial artery and peroneal artery. (d) Proximal occlusion was treated with catheter-directed thrombolysis for 24 h and higher grade stenosis was revealed. (e) Bare stent (6 mm × 40 mm) was deployed to correct the proximal stenosis and completion angiography showed patient SFA.
Urokinase was infused through the thrombolytic catheter via microinfusion, and the thrombolysis was accelerated using pulse-spray infusion. Complete details of the urokinase and unfractionated heparin infusion and laboratory monitoring used in this series have been previously described. 9 The thrombolytic procedure was temporarily stopped when the fibrinogen level dropped to <1.0 g/L.
Adjunctive endovascular treatments including PTA and/or stenting were performed to correct underlying lesions after the thrombolytic procedure. Balloons (4–7 mm in diameter, 60–200 mm long; Admiral Xtreme, Invatec, Italy) and/or extended self-expandable bare stents (5–8 mm in diameter, 60–200 mm long; EV3, Plymouth, MN, USA; Complete SE, Meditronic, MN, USA; or Smart, Cordis, NJ, USA) were used to correct underlying lesions with post-dilation. Stenting was performed only when residual stenosis was >30% or there was a flow-limiting dissection. A completion angiography was performed to observe the result and screen the distal runoff embolization.
Technical success was defined as restored vessel patency with a residual stenosis of <30%. No embolization was seen in the distal runoff. Immediate hemodynamic success was determined by a postoperative ankle-brachial index (ABI) increase of >0.10. Clinical success was defined as a subjective perception of improved walking distance, absence of resting pain and healing of trophic changes.
Complications included major bleeding (intracranial bleeding, bleeding that resulted in death or bleeding that required transfusion, surgery or cessation of thrombolytic therapy), minor bleeding (defined as less severe bleeding managed by local compression, increasing vascular sheath size or decreasing dose of thrombolysis, anticoagulation or antiplatelet drug) and distal runoff embolization.
Patients were discharged on an oral regimen of aspirin (100 mg/day), clopidogrel (75 mg/day) and atorvastatin (20 mg/day). Clinical examinations and duplex ultrasonography were performed before discharge; at 1, 3, and 6 months after discharge; and every 6 months thereafter. A hemodynamic evaluation was done by measuring the ABI and performing duplex ultrasonography in all patients. Restenosis was defined as a decrease in ABI by 0.15, loss of palpable pulses, a peak systolic velocity ratio of ⩾2.510–12 on an ultrasonography scan, or the development of ischaemic symptoms. Computed tomography angiography was performed only in cases where recurrent stenosis was >50% as measured on ultrasonography scans. Secondary reintervention may be necessary to maintain the patency rate in patients with severe claudication or critical limb ischaemia.
Statistical analysis was performed with SPSS software version 18 (SPSS Inc., Chicago, IL, USA). The pre- and postoperative difference in ABI and Rutherford category was analysed using the paired Student’s t-test, and values of p < 0.05 were considered statistically significant.
Results
A total of 26 consecutive patients (26 lower limbs) were enrolled in the study. All the 26 limbs had shown occlusive disease in the lower limb arteries on primary angiography. The mean chronic ischaemia time was 13 months (range, 2–36 months), while the mean duration of deteriorated ischaemia was 29.4 days (range, 14–60 days) accompanied by an upgraded Rutherford category (Table 2). The primary Rutherford category before intervention was category II in 12 patients and III in 14 patients; after ischaemia, the values were category III in 9 patients, IV in 16 patients and V in 1 patient. The infrapopliteal distal runoff was one vessel in seven patients, two vessels in 15 patients and three vessels in four patients.
Characteristics of limb occlusions undergoing CDT.
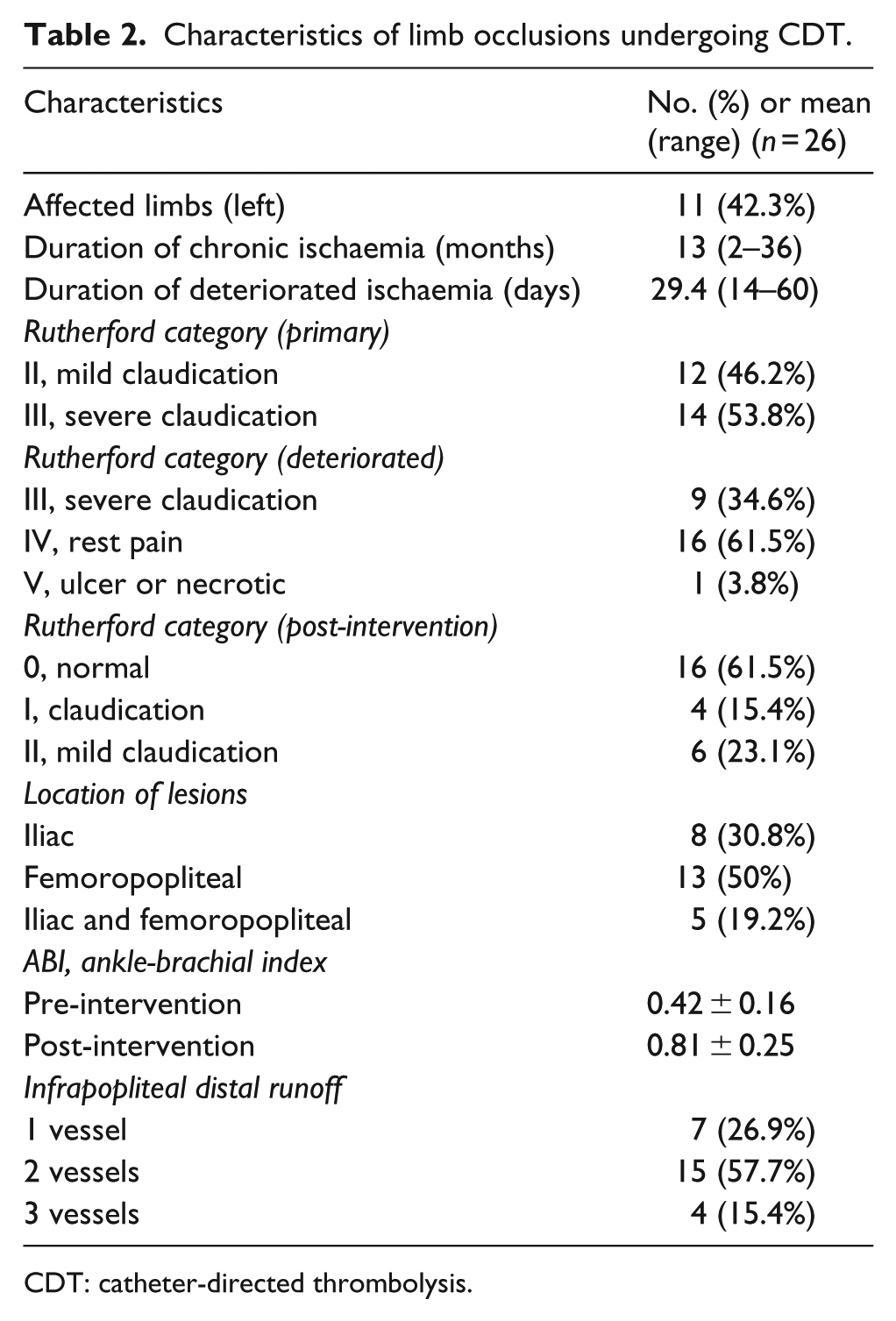
CDT: catheter-directed thrombolysis.
The 26 intra-arterial thrombolysis procedures were all performed in native lower arteries including 8 iliac, 13 femoropopliteal, and 5 diffuse occlusions involving the iliac and femoropopliteal segments. The multi-side-hole thrombolytic catheter was successfully embedded in the occluded segment intraluminally in all the affected limbs. The thrombolytic procedure lasted an average of 45.8 h (range, 42–60 h) with a mean urokinase dose of 1,516,000 IU (range, 1,263,000–1,896,000 IU).
All of the 26 patients achieved a reduction in lesion length by CDT, and lesion length decreased from 194 mm (70–350 mm) to 92 mm (20–270 mm) (p < 0.001). Among them, 24 patients (92.3%) had a TransAtlantic Inter-Society Consensus (TASC) classification downgrade (Table 3). The numbers of patients belonging to B, C and D grades according to preoperative TASC classification were 4 (15.4%), 5 (19.2%) and 17 (65.4%), respectively; and the numbers of cases at the levels A, B, C and D were nine (34.6%), 10 (38.5%), six (23.1%) and one (3.8%), respectively, after surgery. The residual lesions were all corrected with PTA in 4 (15.4%) limbs and stenting in 22 (84.6%) patients without cross-joint stent deployed. Among them, 19 lesions (84.2%) were implanted with only one stent, one lesion (10.5%) was implanted with two stents and two lesions (5.3%) were implanted with three stents (Table 3). The patency rates were 91.6% and 81.5% at 12 and 24 months, respectively (Figure 2).
Characteristics of lesions and thrombolytic procedures.
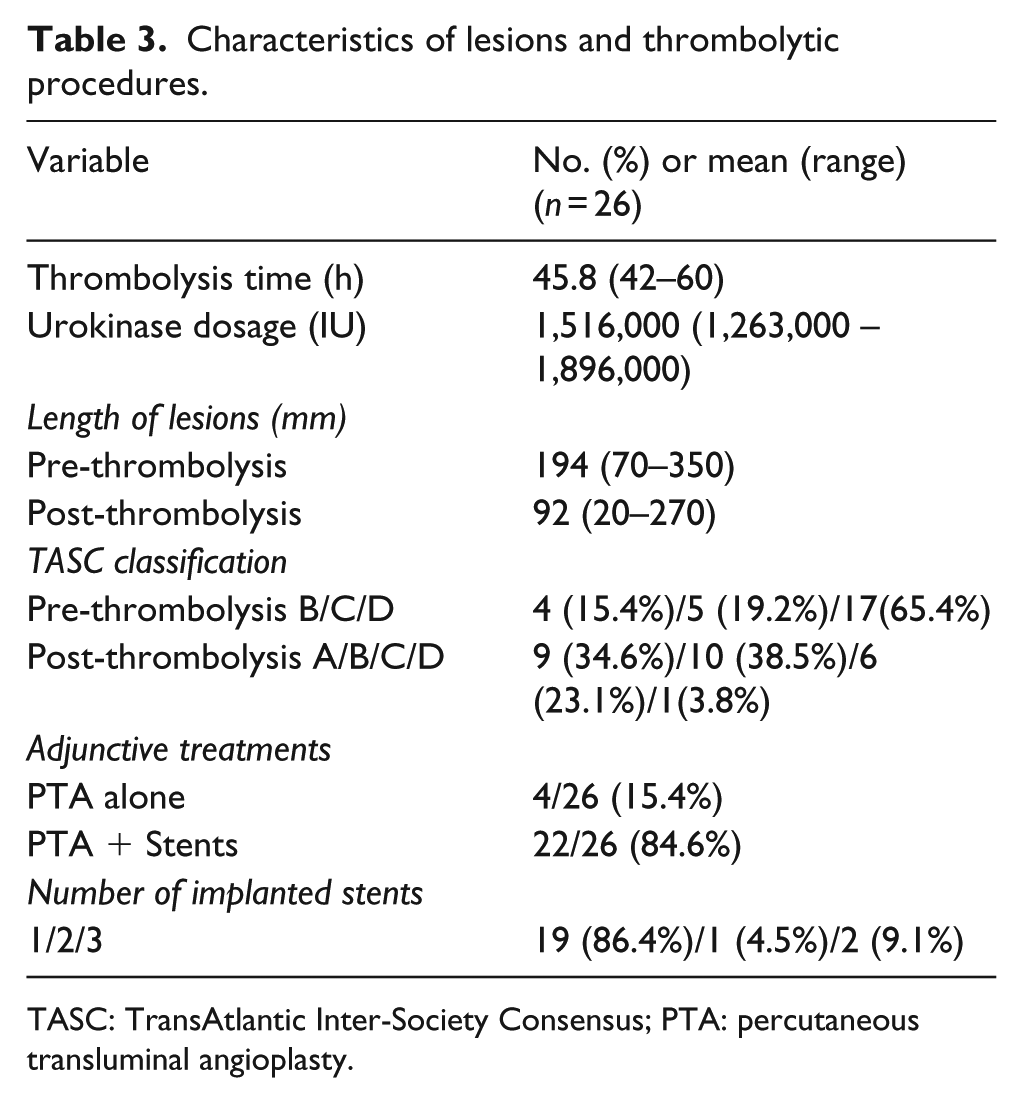
TASC: TransAtlantic Inter-Society Consensus; PTA: percutaneous transluminal angioplasty.
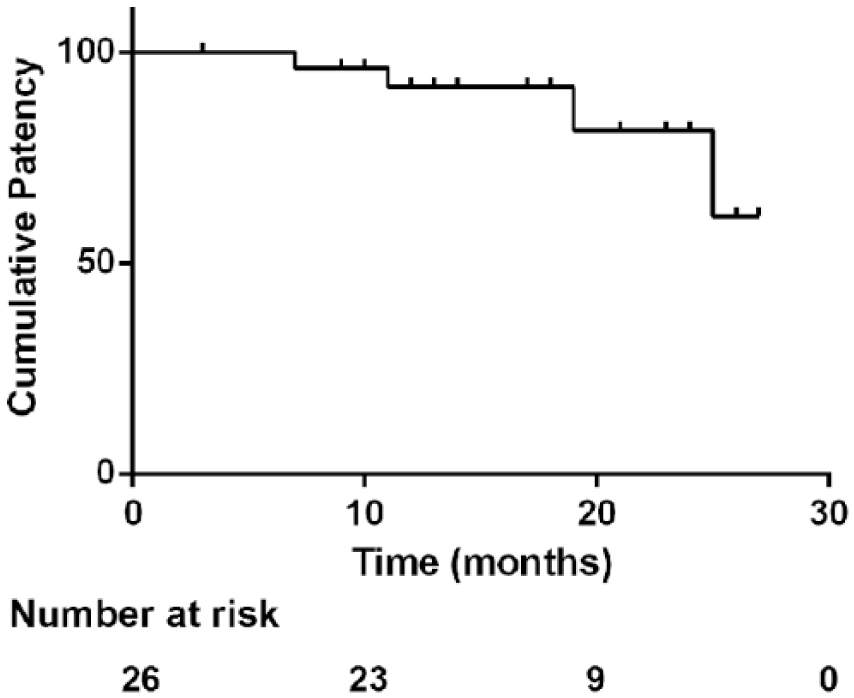
Kaplan–Meier estimates of patency rates.
Complications were observed during the thrombolytic treatment in two patients (morbidity rate, 7.7%). There were no episodes of major bleeding. A perisheath haematoma resulted in premature termination of the thrombolytic procedure in one patient (3.8%) without further treatment. Distal embolization occurred in one patient (3.8%) and it was resolved with thrombolysis and catheter aspiration.
Throughout the treatment process including CDT with adjunctive interventions, 9 patients with intermittent claudication achieved an unrestricted walking distance and 17 patients with rest pain or foot ulcers showed significant symptom improvement. The difference in the distributions of Rutherford category between baseline and discharge was statistically significant (p < 0.001). The mean ABI increased from 0.42 ± 0.16 preoperatively to 0.81 ± 0.25 postoperatively (p < 0.01).
After a mean 16.2 months of follow-up (range, 3–27 months), in-stent restenosis was observed on ultrasonography in four (15.4%) patients. Two (7.7%) patients underwent repeat endovascular treatment, while another two (7.7%) patients had no lifestyle-limiting symptoms and refused reintervention. One (3.8%) patient underwent endovascular treatment for the previously untreated limbs. Two patients died during follow-up because of myocardial infarction in one patient and malignancy in one patient.
Discussion
Sub-acute DCLEI patients may develop a relative fresh thrombus that occludes the main artery or its major collateral branches 4 and they may have aggravating ischaemic manifestations such as severe claudication, rest pain or ischaemic ulcers. Surgical procedures have substantial overall systemic or major morbidity rates in high-risk patients with sub-acute DCLEI and endovascular interventions have revolutionized the mainstay treatment of peripheral arterial disease, even for TASC C or D lesions. These sub-acute DCLEI lesions may be masked by the overlying thrombus, and dissolving the thrombus remains the ideal treatment approach. Because directed endovascular stenting may release embolic particles, 13 CDT therapy and adjunctive PTA or/and stenting was adopted in our study.
CDT therapy has been accepted as a minimally invasive accelerated thrombolysis method that involves increasing the surface area available for enzymatic action, which is useful in clot dissolution, exposing underlying lesions and simplifying subsequent treatment. CDT has been proven effective for the treatment of more acute thrombus. The interaction between urokinase and thrombus was strengthened by the use of a multi-side-hole thrombolytic catheter, and thrombolysis was accelerated using pulse-spray infusion. CDT was also useful for chronic thrombus in patients with a 4-month aggravation history in previous studies by our group and others.2,9 Wholey et al. 2 achieved complete or partial thrombolysis in 85% of sub-acute and 88% of chronic occlusions using urokinase. In our previous report, 9 CDT was effective for proximal relative fresh thrombus dissolution in patients with flush infrarenal aortic occlusion and a 4-month history of aggravating ischaemia, and it transformed flush renal occlusions to focal infrarenal occlusions.
In our study, CDT was also effective for all DCLEI patients with an aggravating ischaemia history of 14 days to 2 months. According to our previous studies, 9 2 months is a relatively critical point and thrombolytic effects may be poor in cases with aggravated symptoms of more than 2 months. In the Surgery versus Thrombolysis for Ischemia of the Lower Extremity (STILE) 14 study, 26% of patients who had aggravating symptoms over 2 months duration experienced poor thrombolytic effects. The key to successful thrombolysis also lies in directing thrombolysis catheter into the true lumen. In the STILE study, failure of catheter placement occurred in 28% of patients who were randomized to lysis, and that were considered treatment failures. Some researchers applied single-curved catheters or sheath catheters rather than a multi-hole thrombolytic catheter, which attenuated the thrombolytic effects. However, apart from continuous thrombolytic drugs, we also adopted pulse-spray infusion at intervals to enhance the thrombolytic effects.
The initial success rate may increase by converting long-segment occlusion to short lesions and downgrading the TASC level. 15 More stents would be deployed if direct stenting was achieved without CDT. In our study, stents (mean, 1.23) were deployed in 22 limbs (84.6%) without cross-joint stenting, and the possibility of stent fracture also decreased. Previous studies reported that the occurrence of stent fractures and in-stent restenosis were related to stented segment length and implanted stent quantity.11,16 We shortened the length of lesions by thrombolytic procedures and reduced the length of stent to improved patency rates. In our study, after removal of the non-acute clot component from the occlusions with thrombolytic procedures, lesion length decreased from 194 to 92 mm. The patency rates were 91.6% and 81.5% at 12 and 24 months, respectively.
It is important to judge whether the lesions coexist with relatively new fresh thrombus, which were comprehensively judged by the following four factors. First, patients with sub-acute DCLEI often have worsening symptoms prior to seeking treatment. Second, the lesions were often crossed rapidly by the wire, usually without the possibility of re-entry, which was almost like going through patient arteries. Third, a spray-like phenomenon from the multi-side-hole thrombolytic catheter could often be observed on angiography. Fourth, the contralateral limb arterial lesions are relatively less extensively involved as evidenced on angiography.
Periprocedural distal embolization during angioplasty is commonly blamed for the obstruction of distal vessels which results in severe distal ischaemia.17,18 It is important to avoid potential distal embolization by a relatively unstable thrombus. In the Siablis study, 19 filter-type emboli protection devices were used in the recanalization of 11 cases of sub-acute arterial occlusion, and rheolytic thrombectomy was performed in acute thrombosis in order to safeguard the distal capillary bed. The captured debris consisted of a fresh thrombus in the acute cases, and calcification with fibrin and cholesterol crystals in the chronic cases. However, König et al. 17 reported on their experience of using the AngioGuard emboli capture device in femoropopliteal angioplasty procedures in which blood flow decreased markedly in patients with concentric lesions rather than those with calcified lesions. They suggested perifilter clot formation as the cause and therefore do not recommend filter use in these cases. In our study, distal embolization was avoided by the use of CDT to remove relatively fresh thrombi. Although it occurred in one patient (3.8%) in the same limbs, it was resolved by thrombolysis and catheter aspiration.
This study had a few limitations. Specifically, it was a retrospective, nonrandomized analysis with a small patient group and a short follow-up period. Thus, a further study is required to evaluate the long-term results of endovascular therapy for more sub-acute DCLEI patients.
Conclusion
Endovascular therapy with CDT and PTA/stenting is feasible for sub-acute DCLEI patients and has lower complication rates and favourable midterm results.
Footnotes
Acknowledgements
L.Y., S.G. and J.D. contributed equally to the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This work was supported by the National Natural Science Foundation of China (grant no. 81500390).