
Abstract
Purpose:
To compare time to a composite endpoint of non-fatal acute myocardial infarction, non-fatal stroke or all-cause mortality in patients with type 2 diabetes mellitus who had their treatment intensified with a dipeptidylpeptidase-4 inhibitor or insulin following dual-therapy (metformin plus sulfonylurea) failure.
Methods:
A retrospective cohort study was conducted on 5238 patients newly treated with either a dipeptidylpeptidase-4 inhibitor or insulin following dual-therapy failure (2007–2014). Data were sourced from UK General Practices. The risk of the composite outcome was compared between two treatment groups: metformin + sulfonylurea + insulin (n = 1584) and metformin + sulfonylurea + dipeptidylpeptidase-4 inhibitor (n = 3654), while adjusting for baseline covariates. Follow-up was for up to 5 years. Propensity score matching analysis and Cox proportional hazard models were employed.
Results:
Overall, 123 and 171 composite outcome events occurred among patients who added insulin versus dipeptidylpeptidase-4 inhibitor, respectively (44.5 vs 14.6 events per 1000 person-years). Addition of insulin was associated with a significantly higher hazard ratio versus the addition of a dipeptidylpeptidase-4 inhibitor (adjusted hazard ratio = 2.6, 95% confidence interval: 1.9–3.4; p < 0.01), an effect that was more pronounced in obese (body mass index: 30–34.9 kg/m2) patients (corresponding adjusted hazard ratio 3.6, 95% confidence interval: 2.3–5.6; p < 0.01).
Conclusion:
In routine clinical practice, intensification of metformin + sulfonylurea therapy by adding insulin is associated with increased risk of cardiovascular events and death compared with adding a dipeptidylpeptidase-4 inhibitor. These findings are in line with suggestions from previous studies regarding the cardiovascular safety of insulin in type 2 diabetes mellitus, but should be interpreted with caution.
Introduction
There is evidence that tight glucose control, especially in the early years after diagnosis, reduces the risk of long-term cardiovascular (CV) complications in patients with type 2 diabetes mellitus (T2DM).1,2 International guidelines therefore recommend an individualized treatment strategy to achieve and maintain target levels of glycaemic control. 3 Metformin (MET) is the usual first-line drug therapy when diet and exercise alone are insufficient.3,4 It used to be the case during the period of this retrospective analysis that the recommended second-line therapy after MET was sulfonylurea (SU), 4 and because of the progressive decline in beta cell function, many patients failed to maintain adequate levels of HbA1c despite up-titration to maximum tolerated doses of dual therapy (MET + SU). However, recent guidelines give more flexibility in prescribing choices. 5
Several treatment options are available when MET and SU dual therapy is insufficient, 3 but there is very limited data on CV and diabetes-related outcomes in this group of patients to inform decision-making about third-line treatments. For many patients, the choice includes adding basal insulin (INS) or a dipeptidylpeptidase-4 (DPP-4) inhibitor as a third oral agent. There are concerns about the CV safety of INS in T2DM,6–10 but these studies have mainly investigated the use of INS per se as monotherapy or in combination with MET.6–10 However, the UK Prospective Diabetes Study (UKPDS) 11 and Outcome Reduction with Initial Glargine Intervention (ORIGIN) 12 trials have demonstrated the safety of INS, while recent prospective randomized clinical trials (RCTs) have shown that the CV outcomes of DPP-4 inhibitors are non-inferior to placebo.13,14 However, no RCT has compared INS with DPP-4 inhibitors either in terms of their CV safety or effectiveness as a third option after MET plus SU fails. Further work is needed to explore the CV safety of INS when used as a third-line therapy, often in patients with longer duration disease and higher CV risk. INS is known to exert antiatherogenic effects, 15 and many patients prefer to delay INS treatment because of fear of injections, weight gain and the risk of hypoglycaemia. Therefore, adding a DPP-4 inhibitor to MET + SU is an effective alternative to lower HbA1c. Prior to recent RCTs which have demonstrated the safety of DPP-4 inhibitor, there has been some uncertainty about CV outcomes with DPP-4 inhibitors,13,16 and till date, there are no comparative outcome studies available on DPP-4 inhibitor versus INS in patients with dual-therapy failure. Therefore, the aim of this study is to compare CV outcomes and mortality among patients with T2DM who, in routine clinical practice, intensified their treatment with the addition of INS or a DPP-4 inhibitor following dual-therapy (MET + SU) failure.
Methods
Study design and data source
We conducted retrospective cohort analyses of data from The Health Improvement Network (THIN) database, which contains anonymous patient data from more than 400 General Practices throughout England and Wales. THIN has been used previously to evaluate diabetes-related outcomes in routine clinical practice. 17
Study population
The study population comprised a cohort of patients identified to have T2DM and registered to a practice for more than 12 months before the index date (1 January 2007 to 30 May 2014). The cohort included patients ⩾18 years old who were newly treated with a DPP-4 inhibitor or INS following MET + SU therapy failure. Patients who were administered other glucose-lowering therapies (GLTs) such as pioglitazone, glucagon-like peptide 1 (GLP-1) receptor agonists, sodium–glucose co-transporter 2 (SGLT2) inhibitors, glinides and acarbose were excluded from the study. Also excluded were patients with a baseline diagnosis of a CV condition. Standardized computerized routines were used to identify and extract information on patients’ prescriptions for GLTs using British National Formulary (BNF) codes and patients’ diagnosis of disease conditions using Read codes. Read codes used in defining the outcome of events are summarized as electronic supplementary material (ESM).
Exposure
The exposures were incident intensification prescription of INS (long-acting, short or fast-acting, or biphasic) or a DPP-4 inhibitor (sitagliptin, vildagliptin, saxagliptin and linagliptin) as third-line GLT following dual (MET + SU) treatment failure. The follow-up period commenced from the index date (the date of incident intensification prescription) to the date of a censoring outcome event until a switch to, or addition of, another anti-diabetic drug, up to 5 years after the index date. The study end date was 30 May 2014. Patients were segregated into two treatment groups based on the GLTs they received at baseline: MET + SU + INS versus MET + SU + DPP-4 inhibitor (reference/control group).
Outcome
The primary composite outcome was time to diagnosis of predefined events. These included non-fatal acute myocardial infarction (AMI), non-fatal stroke and all-cause mortality. Secondary outcomes included CV events (non-fatal AMI, non-fatal stroke and CV-related deaths combined), all-cause deaths and CV-related deaths. Read codes used for identifying AMI and strokes are included in Supplementary Table 1 (available online). CV-related deaths were included where the cause of death was documented. Subjects whose cause of death could not be verified were ignored in the CV death analysis. The risks of events in the study population were compared between the two treatment groups. In addition, descriptive analysis of the glycaemic and body weight responses of patients in each treatment group was conducted.
Covariates
Covariates were selected a priori on the basis of clinical significance. These are baseline demographic and medical parameters, and they include the following: age, gender, social deprivation (measured using Townsend’s index scores), body weight, body mass index (BMI), HbA1c, total cholesterol levels, low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglycerides, systolic and diastolic blood pressure (BP), smoking status, duration of diabetes, glomerular filtration rate (GFR), albumin levels and urinary albumin–creatinine ratio (ACR). Others included the use of lipid-lowering drugs, antihypertensive drugs, aspirin and the following comorbidities at baseline: coronary heart diseases (CHD) other than AMI, peripheral arterial disease (PAD), hypoglycaemia and heart failure.
Statistical analyses
Descriptive analysis of baseline characteristics was conducted for all patients and compared between the INS and DPP-4 inhibitor treated groups using t-test for continuous variables and chi-squared test for categorical variables. Primary analysis estimated the time to the composite outcome of non-fatal AMI, non-fatal stroke or all-cause death in the entire cohort as well as propensity score (PS)-matched cohort. A PS model was estimated using a logistic regression model in which the treatment status was regressed on the baseline covariates. 18 We assessed the balance in baseline covariates between the treated (INS) and reference (DPP-4 inhibitor) subjects using standardized differences before and after matching. 19 An absolute standardized difference >10% indicated serious imbalance. The mean and frequency distribution of measured baseline covariates between treatment groups with the same estimated PS were examined and summarized. Pairs of treated group and reference subjects were matched based on their estimated treatment probabilities using logistic regression. The average treatment effect on the treated (ATT) was estimated by finding at least one match for each of the treated subjects from the reference group. PS was considered as a prognostic covariate and included in a Cox proportional hazards regression model.
Crude and adjusted Kaplan–Meier (KM) estimates of survival functions were obtained for the treatment groups in the full cohort and PS-matched cohort. From these survival functions, we computed the absolute reduction in the probability of an event occurring within a 5-year follow-up. The marginal hazard ratios were also estimated to enable us to quantify the adjusted hazard of an event occurring in the INS-treated group compared to the DPP-4 inhibitor group. Proportional hazard assumptions were confirmed through Schoenfeld residuals test. 20 Point estimates with 95% confidence interval (CI) at the conventional statistical significance level of 0.05 were used in the regression models. Missing data among covariates were accounted for with multiple imputations using the chained equation (MICE) model. 21 All analyses were conducted using Stata Software, version 13. 22
Subgroup and sensitivity analyses
We examined the hazard ratio of an event occurring in subgroups of patients with BMI between 30 and 34.9 kg/m2 and those with BMI ⩾ 35 kg/m2. BMI categories were broken down into BMI < 30, 30–34.9 and >35 kg/m2 distinguishing overweight, obese and morbidly obese because National Institute for Health and Care Excellence (NICE) refer to BMI > 35 as arbitrary cut-off for certain prescribing choices rather than patient numbers in each group. Sensitivity analysis was aimed at examining the assumption of no unmeasured binary confounding variable.23,24 Assumption was made for an unmeasured covariate that would increase the odds of assigned treatment. 18 Sensitivity analysis was applied to KM survival functions in the PS-matched cohort. In addition, a sensitivity analysis was carried out to compare results of covariates with missing data with those having multiple-imputed data to assess the reliability of the outcomes and the impact of missing data.
Biases
Our analysis employed the ‘new user’ design to minimize biases associated with prevalent use of intensification regimens. 23 In an approach similar to that used in as-treated analyses, we used the intensification regimen to define drug exposure; post index date exposure to any GLT other than a DPP-4 inhibitor or INS was not permitted in our study to reduce confounding by indication.
Immortal-time bias was also addressed by ensuring subjects diagnosed with outcome events on or before the index date were excluded. In addition, to eliminate bias that may occur from KM estimates of survival functions due to an unbalanced distribution of covariates, we used the stratified log-rank test to compare the equality of the survival curves in the matched sets (KM survival curves were estimated separately for INS treated and compared with DPP-4 inhibitor–treated participants in the PS-matched sample). 25
Results
General patient characteristics
After screening 8654 patients who intensified MET + SU treatment with a third-line drug, 5238 patients made the criteria for cohort entry and were assigned to one of the two treatment groups as outlined in Figure 1. The number (proportion) of patients assigned to each treatment group included n = 1584 (30%) for MET + SU + INS and n = 3654 (70%) for MET + SU + DPP-4 inhibitor.
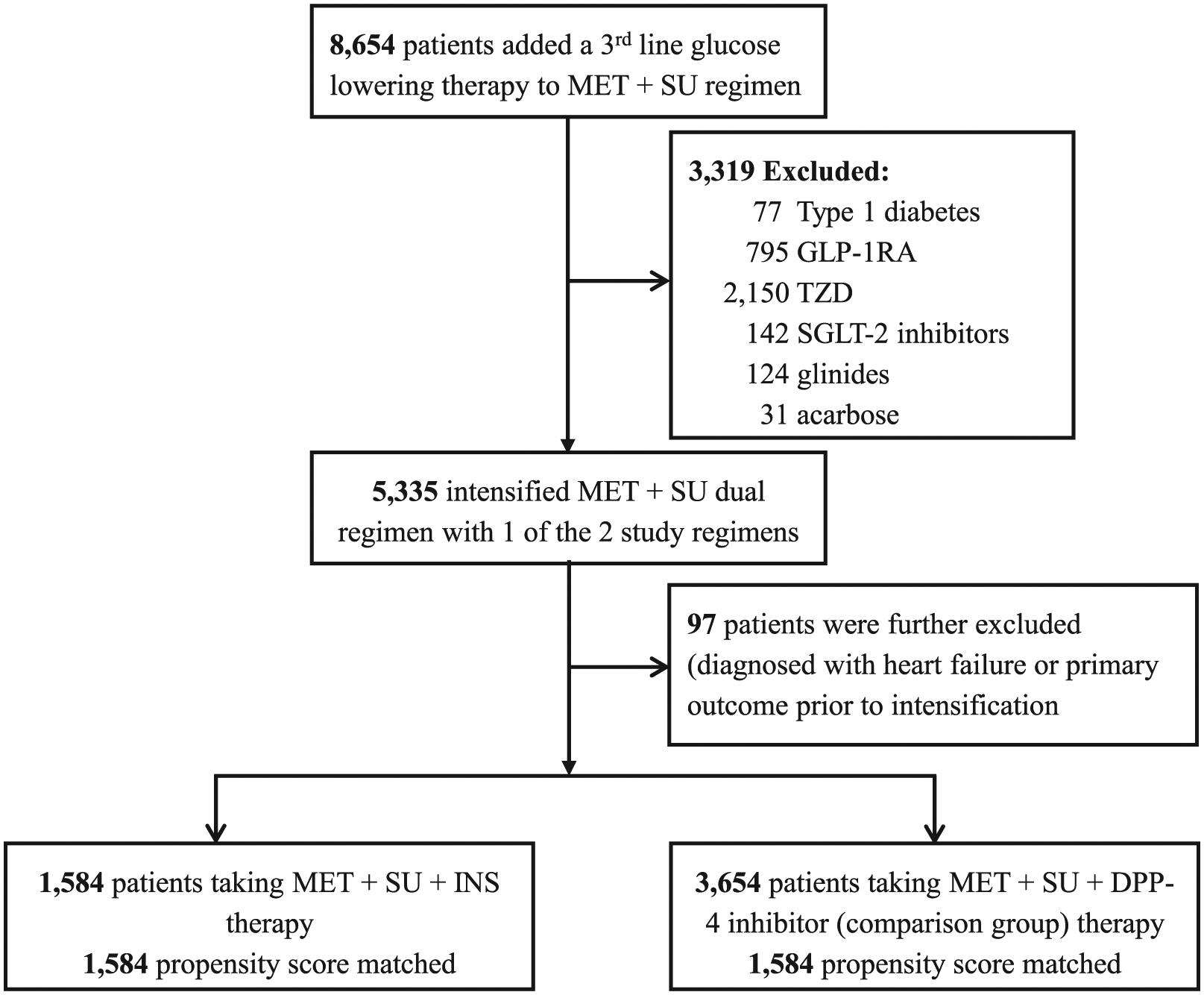
Study population screening and selection process.
Graph shows the addition of INS appearing to have a lower HbA1c reduction; however, this was not statistically different to the addition of a DPP-4i, with the exception of changes at 1 year (−3% vs −1%, respectively).
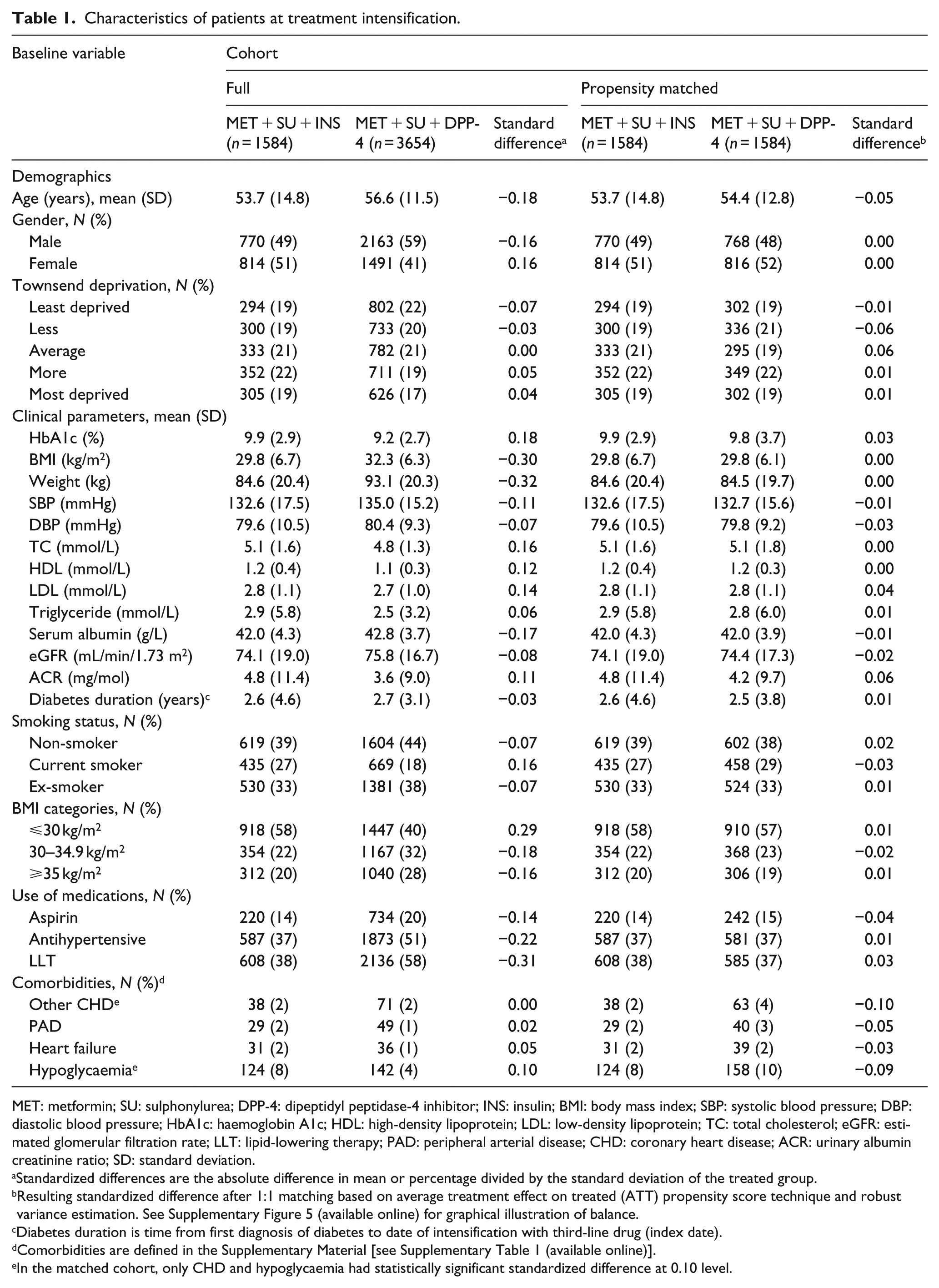
Patients had a mean age of 56 years and constituted 56% male. Compared with patients who added a DPP-4 inhibitor, those who added INS to MET + SU before PS matching had higher mean HbA1c levels of 9.9% (85 mmol/mol) versus 9.2% (77 mmol/mol), respectively, and many of the measured covariates had a standardized difference above the 0.10 level (Table 1). The application of PS matching resulted in the inclusion of 3168 patients (1584 MET + SU + INS matched 1:1 with MET + SU + DPP-4 inhibitor) and brought into balance the distributions of the measured covariates. Apart from previous hypoglycaemia and a diagnosis of other CHD, the baseline characteristics of the matched sample were not statistically different; as a result, the systematic differences between INS and DPP-4 inhibitor subjects in the original sample have been substantially reduced or eliminated in the matched sample (Table 1). This shows that the differences between the treatment groups have been reduced by PS matching and adequate balance on baseline covariates has been induced by the specification of the PS model used.
Characteristics of patients at treatment intensification.
MET: metformin; SU: sulphonylurea; DPP-4: dipeptidyl peptidase-4 inhibitor; INS: insulin; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; HbA1c: haemoglobin A1c; HDL: high-density lipoprotein; LDL: low-density lipoprotein; TC: total cholesterol; eGFR: estimated glomerular filtration rate; LLT: lipid-lowering therapy; PAD: peripheral arterial disease; CHD: coronary heart disease; ACR: urinary albumin creatinine ratio; SD: standard deviation.
Standardized differences are the absolute difference in mean or percentage divided by the standard deviation of the treated group.
Resulting standardized difference after 1:1 matching based on average treatment effect on treated (ATT) propensity score technique and robust variance estimation. See Supplementary Figure 5 (available online) for graphical illustration of balance.
Diabetes duration is time from first diagnosis of diabetes to date of intensification with third-line drug (index date).
Comorbidities are defined in the Supplementary Material [see Supplementary Table 1 (available online)].
In the matched cohort, only CHD and hypoglycaemia had statistically significant standardized difference at 0.10 level.
Time to composite outcome
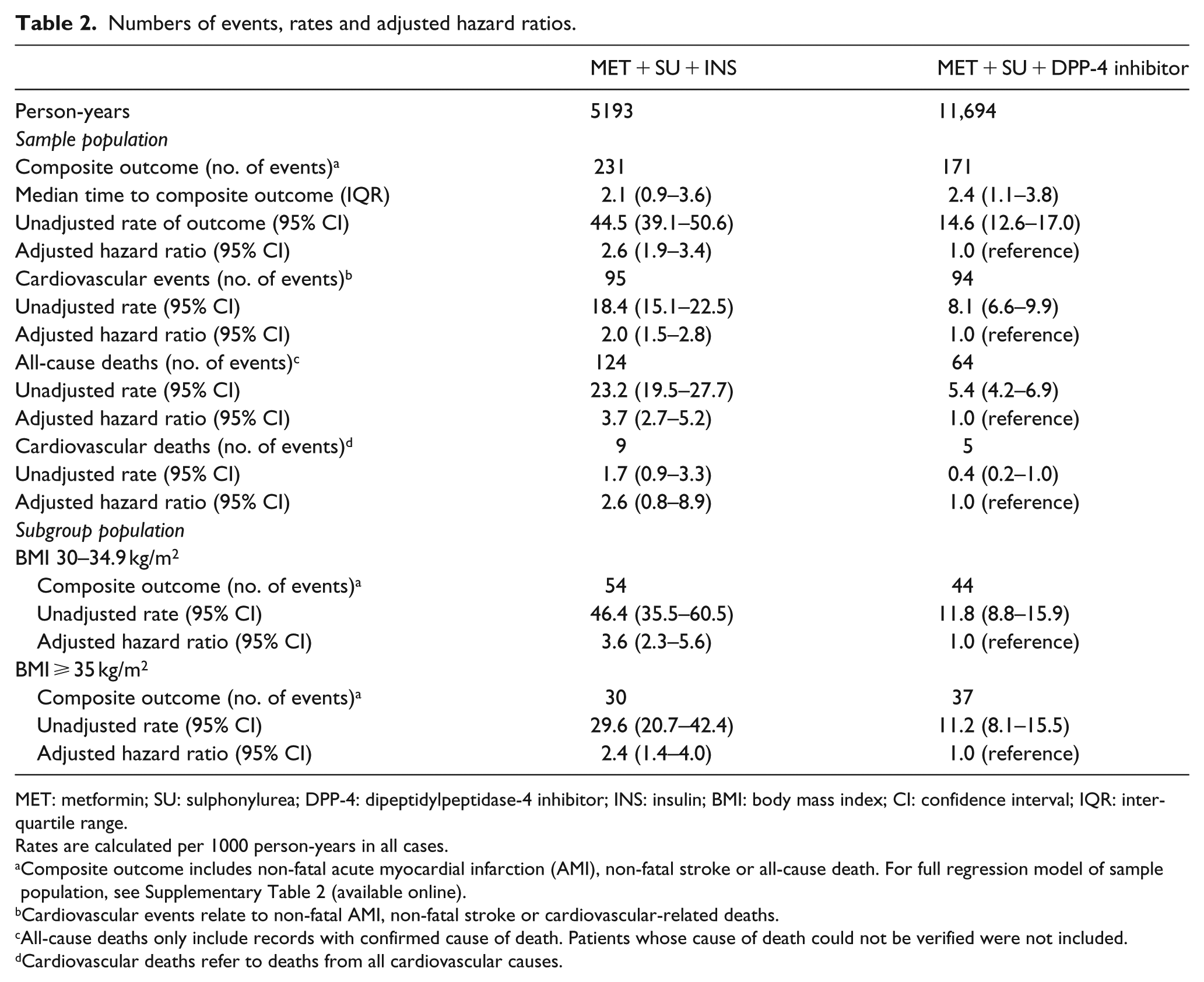
The time to a composite outcome in the cohort of patients is summarized in Table 2. The median time before the composite outcome among the DPP-4 inhibitor users was longer at 2.4 years (interquartile range (IQR): 1.1–3.8) compared to INS users (2.1 years, IQR: 0.9–3.6). The survival analysis showed that the 5-year cumulative incidence of composite outcome was 9% with DPP-4 inhibitor and 23% with INS.
Numbers of events, rates and adjusted hazard ratios.
MET: metformin; SU: sulphonylurea; DPP-4: dipeptidylpeptidase-4 inhibitor; INS: insulin; BMI: body mass index; CI: confidence interval; IQR: interquartile range.
Rates are calculated per 1000 person-years in all cases.
Composite outcome includes non-fatal acute myocardial infarction (AMI), non-fatal stroke or all-cause death. For full regression model of sample population, see Supplementary Table 2 (available online).
Cardiovascular events relate to non-fatal AMI, non-fatal stroke or cardiovascular-related deaths.
All-cause deaths only include records with confirmed cause of death. Patients whose cause of death could not be verified were not included.
Cardiovascular deaths refer to deaths from all cardiovascular causes.
Estimating survival curves and survival effects
Crude KM survival curves for INS subjects and the reference DPP-4 inhibitor subjects in the full original sample are reported in Figure 2(a). The result showed there was a significant difference between the two curves; log-rank test p < 0.001. The KM survival curves obtained from the PS-matched sample are summarized (stratified log-rank test p < 0.001; Figure 2(b)). From the estimated survival curves, our data showed that patients who intensified treatment with INS were significantly more likely to experience a composite outcome than those who added a DPP-4 inhibitor. For example, from the matched sample, the probability of dying or experiencing a CV event at 3 years was 0.11 (95% CI: 0.10–1.03) with INS and 0.03 (95% CI: 0.02–0.04) with a DPP-4 inhibitor.
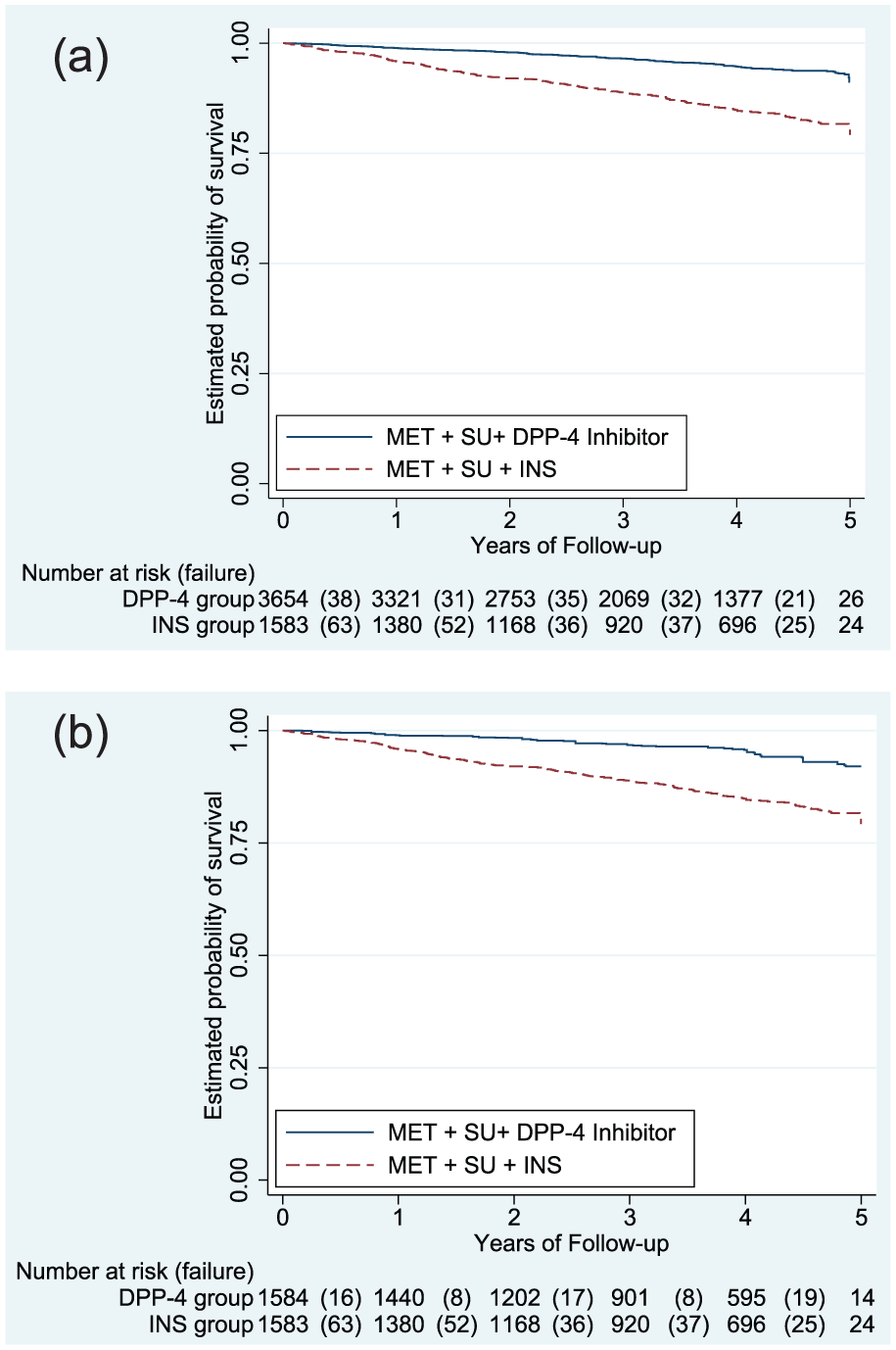
Kaplan-Meier survival curves for INS-treated vs reference DPP-4 inhibitor-treated groups in (a) the original cohort and (b) the propensity score matched cohort.
Overall, there were 123 and 171 composite outcome events among patients who added INS versus a DPP-4 inhibitor, respectively (44.5 vs 14.6 events per 1000 person-years). The rate of occurrence remained the same after matching. The adjusted hazard ratio (aHR) from the PS-matched model was 2.6 (95% CI: 1.9–3.4; p < 0.01; Table 2). A breakdown of the number of component outcome events showed the following: the number of CV events (non-fatal AMI, non-fatal stroke or CV-related deaths) was 95 and 94 among patients who added INS versus a DPP-4 inhibitor, respectively (18 vs 8 events per 1000 person-years; p < 0.01); all-cause deaths were 124 versus 64 events, respectively (23 vs 5 events per 1000 person-years; Table 2).
Subgroup and other analyses
In a subgroup of patients with BMI 30–34.9 kg/m2, the composite outcomes were 54 and 44 among patients who added INS versus a DPP-4 inhibitor, respectively [46 vs 12 events per 1000 person-years; aHR 3.6 (2.3–5.6); p < 0.01]. The subgroup with BMI ⩾ 35 kg/m2 had 30 and 37 composite events from intensification with INS versus a DPP-4 inhibitor [30 vs 11 events per 1000 person-years; aHR 2.4 (1.4–4.0); p < 0.01; Table 2].
Stratification analysis across baseline BMI categories showed the risk of composite outcome among obese (BMI: 30–34.9 kg/m2) patients was not significantly different to normal BMI status (BMI ⩽ 30 kg/m2) patients.
In terms of glycaemic response, INS versus DPP-4 inhibitor users showed absolute mean reduction in HbA1c of −1.3% (14 mmol/mol) versus −1.0% (11 mmol/mol), respectively (p < 0.001). With the exception of the period between 48 weeks and 1 year, the mean reduction in HbA1c was not significantly different between INS and DPP-4 inhibitor over time (Supplementary Figure 1, available online).
An absolute significant body weight increase was observed with INS (1.2 kg; p < 0.001), whereas DPP-4 inhibitor showed a non-significant weight loss (−0.1 kg; p = 0.5). From our data, INS users appeared to have consistently gained weight after the first year of treatment intensification (Supplementary Figure 2, available online).
Sensitivity analyses
One of the analyses was to assess how strongly an unmeasured confounder would have to be associated with treatment selection in order for a previously statistically significant treatment effect to become statistically non-significant if the unmeasured confounder had been accounted for. However, a large majority of estimated effects of covariates in our study were not statistically significant. Therefore, we did not employ this sensitivity analysis. Moreover, the p value for the stratified log-rank test in the matched cohort was p < 0.001. Hence, the small p value obtained in the primary analysis cannot be taken as an indication that the study is insensitive to unmeasured confounders. The sensitivity analysis on missing data yielded comparable results to complete case models [aHR 2.3 (1.7–3.0); p < 0.001], which reflects results that are unlikely to be attributable to bias from missing information. The probability density functions of the PS matching of the treatment groups show there was no violation of the overlap assumption 26 (Supplementary Figure 4, available online).
Discussion
This study has shown that in people who may need to have more therapy to lower their glycaemia, those who are selected by their general practitioner (GP) to have DPP-4 inhibitor were less likely to experience the composite outcome of non-fatal AMI, non-fatal stroke or death. Furthermore, the increased risk with INS was even higher among the subgroup of patients who were obese (BMI > 30). In the absence of a consensus on which third-line treatment is most appropriate when maximum tolerated doses of MET + SU fail to maintain adequate glycaemic control, this study identifies important differences in CV and mortality outcomes between two treatment options that are frequently used in patients with dual-therapy failure.
The risk-benefit balance and overall safety of a more intensive treatment strategy in T2DM have recently been questioned, 27 and in particular, the use of INS has been associated with an increase in life-threatening hypoglycaemia risk and mortality. 6 Other observational studies have also raised concerns about INS use in T2DM. For example, a dose-response relationship between INS exposure and all-cause deaths was reported in a large Canadian population, 7 and worse survival was reported among INS-treated patients (relative to those on MET + SU) in a study exploring the relationship between HbA1c and CV diseases. 8 More recently, adverse CV events and increases in all-cause mortality were reported in a cohort of patients who received INS compared with other agents, 9 and among those whose treatment was intensified to INS (compared with adding a SU) following failure of MET monotherapy. 10 However, an important limitation of these observational studies was their inability to control for differences in HbA1c, 7 hidden confounders or allocation bias8–10 because they compared INS therapy with either MET or SU, both of which are often used much earlier in the course of the disease. This study overcomes many of these limitations and specifically compared outcomes in a cohort of dual-therapy failure patients without prior evidence of CV disease.
The observation of an even higher hazard ratio for the composite of non-fatal AMI, non-fatal stroke and all-cause death among the obese subgroup is clinically important. INS therapy is associated with weight gain, thereby increasing the amount of INS required to control hyperglycaemia,28,29 at the expense of further weight gain, increased INS resistance and potentially increased risk of CHD. 30 Our study population still had suboptimal glucose control (HbA1c > 8% or 64 mmol/mol) despite treatment intensification with INS. Our data show that patients in our study population have poor response to diabetes management, although this may not apply to most other populations. Therefore, patient factors associated with persistently high HbA1c might be an important determinant of increased mortality risks and may need to be further investigated. We would speculate that patients in our study may have required high-dose INS treatment in order to achieve glycaemic targets. We have previously shown that the effectiveness of INS therapy to lower HbA1c levels among overweight patients with diabetes is reduced. 31
Our analyses were subject to a number of limitations that are inherent to observational studies. First, we cannot be certain that the patients were fully compliant with their medication. Other factors apart from HbA1c may also influence the decision to intensify treatment in everyday practice. These may include tolerability, cost and patient’s preference. In addition, covariates were mainly included as baseline parameters and their effects were not assessed during the follow-up period, some of these variables are relevant during the entire observation period for monitoring outcomes. Although we could not account for potential residual confounders such as compliance, indications for intensification treatments, markers of β-cell deterioration and differences in dosages, we were able to account for differences in the observed covariates and used robust analytical techniques to control confounding that may bias the results of the estimated treatment effects. Our use of PS matching to estimate average treatment effect in the dataset contributed to the balancing of treatment and comparison groups on the available covariates. However, this technique only accounts for observed covariates. Although we ensured a thoughtful and thorough specification of the selection model was employed to successfully apply the PS matching technique and minimize bias, our study findings must be interpreted with caution in light of the above limitations. Furthermore, there are other newer agents which will most likely be used in place of INS after MET + SU combination therapy such as GLP-1 agonist and SGLT2 inhibitors given their benefit in weight and hypoglycaemia risk. The changing landscape of diabetes management could undermine the relevance of the clinical implications of findings from this study.
Conclusion
Patients with T2DM fail to maintain adequate levels of HbA1c despite up-titration to maximum tolerated doses of dual therapy (MET + SU). Comparative effectiveness studies and RCTs which examine the risks of CV events or deaths from the co-administration of INS or DPP-4 inhibitor as third-line regimens are not reported. Conducting RCTs at this level of treatment is not without its numerous challenges. We observed that among patients with diabetes who are receiving MET and SU therapy, the addition of INS compared with DPP-4 inhibitor was associated with an increased risk of a composite of non-fatal CV outcomes and all-cause mortality. The observed excess risk of adverse CV events was increased in patients who are obese. INS is a still a very important treatment option in the management of T2DM, and our data are not clinically applicable until RCTs comparing INS with DPP-4 inhibitors have been conducted. These findings require further investigation to clarify the risk associated with INS, especially among obese patients with T2DM, in view of the increasing availability of other therapies.
Footnotes
Declaration of conflicting interests
I.I. and D.R. have both received speaker fees from MSD, Astra Zeneca, Eli Lilly and Novo Nordisk. M.J. and M.R. have no relevant financial or other relationships to disclose.
Ethical approval
This article is based on anonymous patient data and does not involve any new studies of human or animal subjects performed by any of the authors. Ethical approval was obtained as part of the Specialist Research Committee approval by The Health Improvement Network, provided by the National Research Ethics Committee and South East Research Ethics Committee.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.