
Abstract
Background:
Endothelial dysfunction contributes to the development of vascular complication in diabetes. Arginase has emerged as a key mechanism behind endothelial dysfunction by its reciprocal regulation of nitric oxide production by substrate competition. We hypothesized that increased arginase activity in patients with type 2 diabetes shifts the metabolism of
Methods:
Forearm endothelium-dependent vasodilatation and endothelium-independent vasodilatation were determined in 15 patients with type 2 diabetes and 10 healthy controls and related to amino acids reflecting arginase and nitric oxide synthase activity.
Results:
Compared to healthy controls, patients with diabetes had impaired endothelium-dependent vasodilatation and endothelium-independent vasodilatation. The ratios of ornithine/citrulline and proline/citrulline were 60% and 95% higher, respectively, in patients with diabetes than in controls (p < 0.001). The plasma ornithine/arginine ratio was 36% higher in patients with diabetes, indicating increased arginase activity. These ratios were inversely correlated to endothelium-dependent vasodilatation and endothelium-independent vasodilatation.
Conclusion:
Patients with diabetes and macrovascular complications have increased amino acid ratios reflecting a shift in arginine metabolism due to arginase activation. These changes are inversely related to endothelial function supporting that arginase activity contributes to endothelial dysfunction.
Introduction
Endothelial dysfunction is a central mediator for the development of cardiovascular diseases including atherosclerosis and vascular complications associated with diabetes.1,2 Reduced bioavailability of nitric oxide (NO) is a key factor behind endothelial dysfunction and the progression of cardiovascular disease due to its importance for normal vascular homeostasis.
3
NO is produced together with citrulline from the amino acid
The activity of arginase has been shown to be increased in animal models of atherosclerosis7,8 and diabetes9–11 which leads to reduced NO formation and increased production of reactive oxygen species. Accordingly, arginase blockade results in improved endothelial function.7,11–13 This mechanism also seems to be highly relevant for patients with cardiovascular disease. We have shown that arginase blockade markedly improves endothelium-dependent vasodilatation in patient with coronary artery disease. Importantly, this effect is particularly pronounced among patients with type 2 diabetes, whereas no effect is observed in healthy subjects. 14 The improvement in endothelial function induced by arginase blockade was mediated by increased production of NO from eNOS. These observations suggest that patients with type 2 diabetes have increased activity of arginase resulting in a shift in the balance of arginase/NOS driving endothelial dysfunction. This shift in enzyme activities is likely to result in changed ratios of the amino acids substrate (arginine) and products of arginase (ornithine) and NOS (citrulline). Ornithine is further metabolized to form proline by ornithine aminotransferase. 5 Quantification of these amino acids and their ratios may be useful for determination of the relative activity of arginase and NOS in the clinical setting.
We therefore hypothesized that patients with type 2 diabetes have increased ratios of plasma ornithine/citrulline and proline/citrulline as a result of increased arginase activity and that this change is associated with endothelial dysfunction. To test this hypothesis, we determined the amino acid substrate and products of arginase and NOS and correlated them with endothelium-dependent vasodilatation (EDV) and endothelium-independent vasodilatation (EIDV) in patients with type 2 diabetes and age-matched healthy control subjects.
Method
Subjects
The study was performed on two groups of male subjects. Patient characteristics are summarized in Table 1. One group (n = 15) consisted of patients with type 2 diabetes and macrovascular complications and the other group (n = 10) consisted of healthy controls. Patients were classified as having type 2 diabetes if fasting blood glucose exceeded 7 mmol/L on two different occasions, if blood glucose exceeded 11 mmol/L 2 h after oral administration of 75 g of glucose or medical history of type 2 diabetes. Macrovascular complication was defined as coronary artery disease diagnosed as history of previous myocardial infarction or treatment with percutaneous coronary intervention or coronary artery by-pass grafting due to significant coronary artery stenosis. Healthy control subjects had no history of cardiovascular disease, and diabetes was excluded by an oral glucose tolerance test. The study was conducted according to the principles outlined by the Declaration of Helsinki and was approved by the regional ethical committee. All patients were informed of the purpose and possible risks of the study and gave their oral and written informed consent.
Basal characteristics.
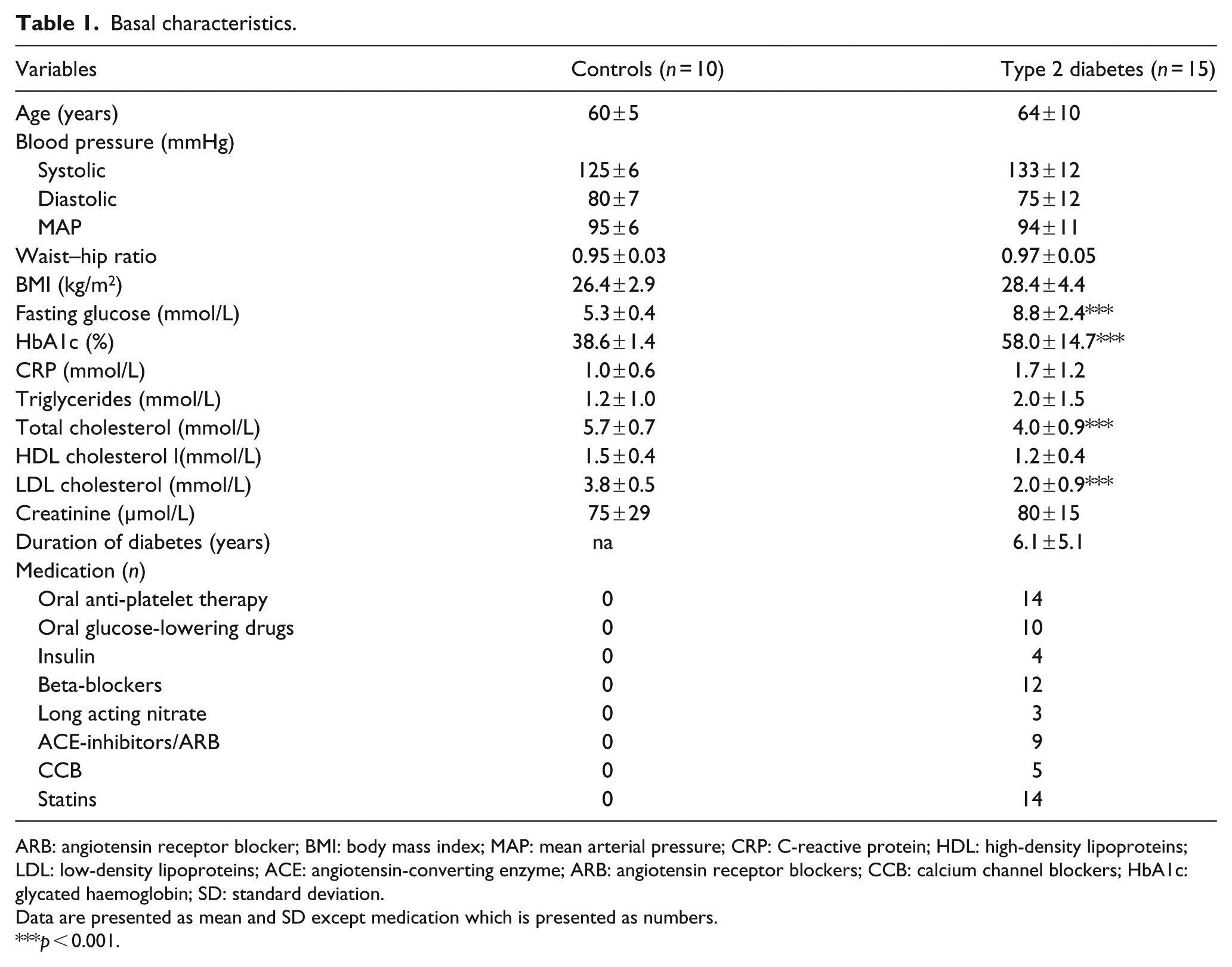
ARB: angiotensin receptor blocker; BMI: body mass index; MAP: mean arterial pressure; CRP: C-reactive protein; HDL: high-density lipoproteins; LDL: low-density lipoproteins; ACE: angiotensin-converting enzyme; ARB: angiotensin receptor blockers; CCB: calcium channel blockers; HbA1c: glycated haemoglobin; SD: standard deviation.
Data are presented as mean and SD except medication which is presented as numbers.
p < 0.001.
EDV and EIDV
All patients arrived in the laboratory at 8 a.m. after an overnight fasting period. After collection of a basal venous blood sample, the patients were given a light breakfast. Blood flow in both forearms was measured using venous occlusion plethysmography14,15 using mercury-in-silastic strain gauge applied around the widest part of the forearm. Two cuffs are placed on each arm: one above the wrist and one around the upper part of the arm. The proximal cuff was inflated to 40 mmHg in 10-s periods to occlude the venous outflow without affecting the arterial inflow. Simultaneously the wrist cuffs were inflated to 200 mmHg to exclude the circulation of the hands. A catheter was introduced in the brachial artery under local anaesthesia (Carbocain 2 mL, 5 mg/mL) of the non-dominant arm for administration drugs. Baseline forearm blood flow was determined by intra-arterial (i.a.) infusion of saline (2.5 mL/min) for 2 min. This was followed by i.a. infusion of the endothelium-dependent vasodilator serotonin (21, 70 and 210 ng/min) and the endothelium-independent vasodilator sodium nitroprusside (SNP 1, 3 and 10 µg/min). Each dose was given for 2 min at a rate of 2.5 mL/min with a 2-min washout period between each dose. Serotonin has previously been demonstrated to evoke NO-dependent vasodilatation in the human forearm of patients with type 2 diabetes and coronary artery disease. 14
Amino acid quantification
Blood samples were drawn in ethylenediaminetetraacetic acid (EDTA) tubes and centrifuged immediately at 1750g and +4°C for 15 min. The supernatant was removed and frozen at −80°C. At analysis, plasma was thawed and centrifuged for 10 min for 1600g. Proteins were removed by mixing 300 µL plasma with 300 µL 10% sulpha salicylic acid containing norleucine. Samples were left to rest for 1 h at +4°C after which they were centrifuged at 13,600g and +4°C for 10 min. The supernatant was filtered through a 0.22-µm filter. Samples were analysed directly with ion chromatography on a Biochrom 30 amino acid analyser. A 20-µL filtrate was injected into a cation-switcher cylinder. The amino acids were eluted with five citrate-based buffers, with rising pH and molarity (added one after the other through the system). The eluate was mixed with ninhydrin which passed through the reaction unit (coil, 135 C) where the reaction of the amino acids and the ninhydrin took place. The absorbance was measured at 570 and 440 nm. The results were analysed with the program EZCHrom Elite (Agilent Technologies, Santa Clara, CA, USA).
Calculations and statistics
Baseline forearm blood flow was calculated as the mean of four inflow curves during infusion of saline and expressed as mL/min/1000 mL tissue. EDV and EIDV were calculated as the increase in flow from baseline during the infusions of serotonin and SNP, respectively, using the four highest inflow curves for each dose. In addition, the total EDV and EIDV were determined by calculating the area under the curve (AUC) for all three doses of serotonin and SNP in each subject. Amino acid levels are presented both as absolute values and as ratios. Global arginine bioavailability ratio was calculated as arginine/(citrulline + ornithine). All data are presented as mean and standard deviation (SD) unless otherwise stated. Differences in EDV and EIDV between patients and controls were determined using two-way analysis of variance (ANOVA). Student’s t test was used to determine differences in basal characteristics, amino acid concentrations and ratios of amino acids between the two groups. The ratios of the amino acids were correlated to EDV and EIDV using Pearson’s regression. All analyses were performed using Graph Pad Prism (GraphPad Software, Inc., La Jolla, CA, USA) A p value of <0.05 was considered significant.
Results
Subjects
Patient characteristics are presented in Table 1. The groups were well matched for age and blood pressure. As expected, the patient group with type 2 diabetes had significantly higher fasting glucose and HbA1c but lower low-density lipoprotein (LDL) cholesterol levels than the control group. The mean duration of diabetes among the patients was 6.0 ± 5.1 years.
EDV and EIDV
EDV and EIDV in patients with diabetes and controls are shown in Figure 1. Patients with diabetes had significantly lower EDV than the control group. Also, EIDV was impaired in patients with diabetes The AUC of EDV was 48.3 ± 36.3 mL/min/1000 mL in the patient group with diabetes and 130 ± 54.6 mL/min/1000 mL in the control group (p < 0.001). AUC for EIDV was 282 ± 96.9 in patients with diabetes and 406 ± 106 mL/min/1000 mL in healthy controls (p < 0.01).
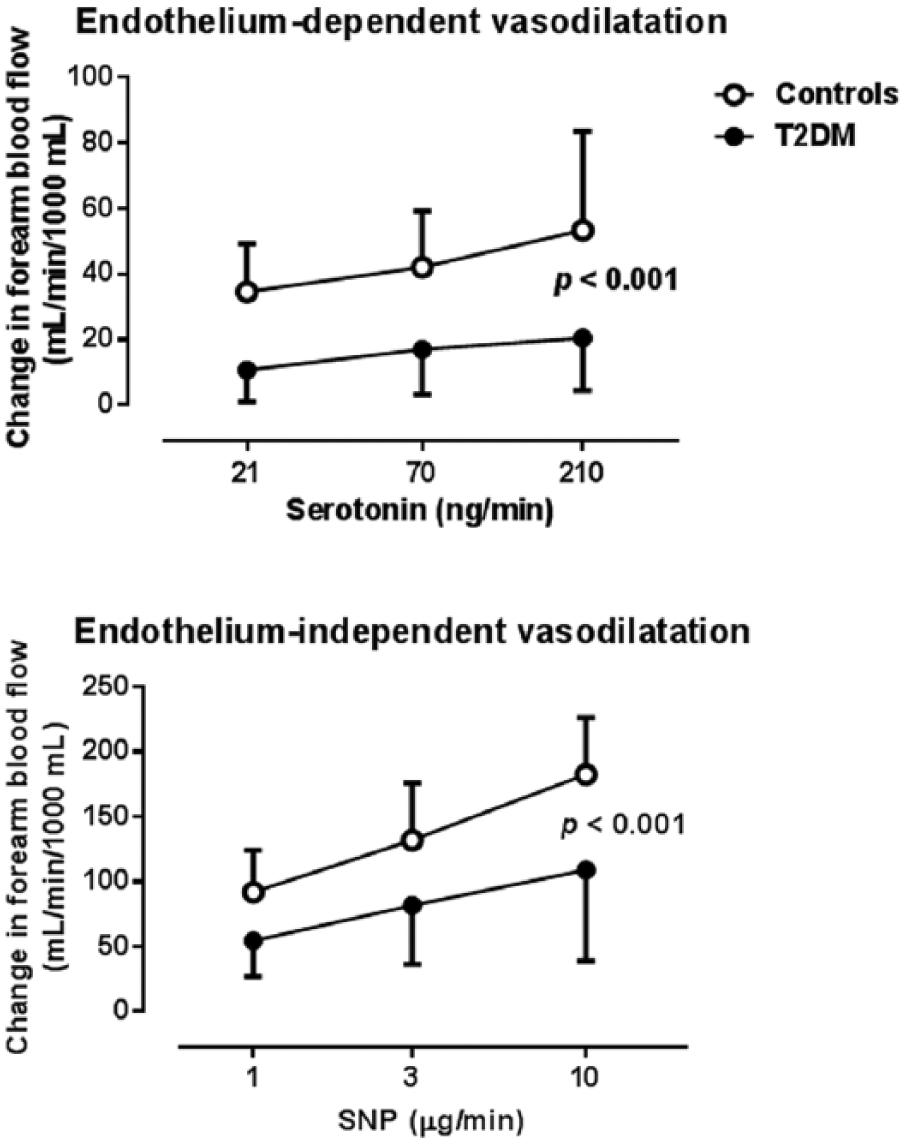
Endothelium-dependent and endothelium-independent vasodilatation expressed as change in forearm blood flow from baseline induced by serotonin and nitroprusside (SNP) in healthy controls and patients with type 2 diabetes (T2DM).
Amino acid levels and ratios
The absolute values of the amino acids are presented in Table 2. Citrulline and arginine levels were significantly lower in patients with type 2 diabetes than in controls. The levels of proline were higher in patients with diabetes than in the control group. The ratios between amino acid substrate and products for arginase and NOS were calculated as a measurement for the relative activities of the two enzymes. Patients with type 2 diabetes had significantly higher ratios of ornithine/citrulline, proline/citrulline and ornithine/arginine (Figure 2). The citrulline/arginine ratio did not differ between the two groups (0.33 ± 0.11 in the diabetes group vs 0.38 ± 0.07 in the control group). The ratio ornithine/arginine, reflecting arginase activity, was negatively related to EDV (r = −0.62, p < 0.001). The ratios of ornithine/citrulline and proline/citrulline were also negatively correlated to EDV (r = −0.52, p < 0.001 and r = −0.41, p < 0.05, respectively) and to EIDV (r = −0.63, p < 0.001 and r = −0.46, p < 0.01, respectively) (Figures 3 and 4). Global arginine availability ratio (i.e. arginine/(citrulline + ornithine)) did not differ between healthy controls (1.08 ± 0.14) and patients with type 2 diabetes (0.95 ± 0.19).
Amino acid levels.
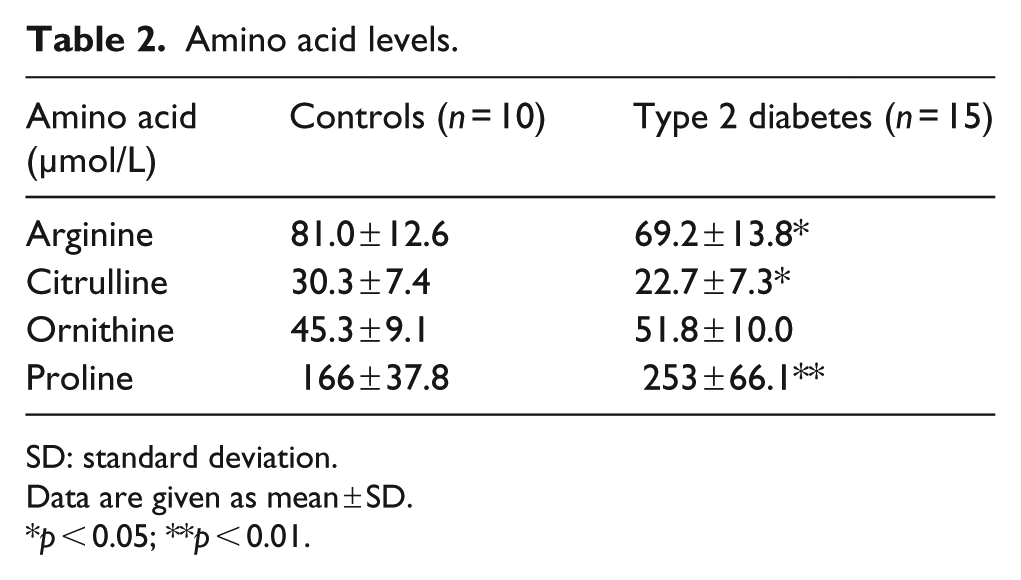
SD: standard deviation.
Data are given as mean ± SD.
p < 0.05; **p < 0.01.
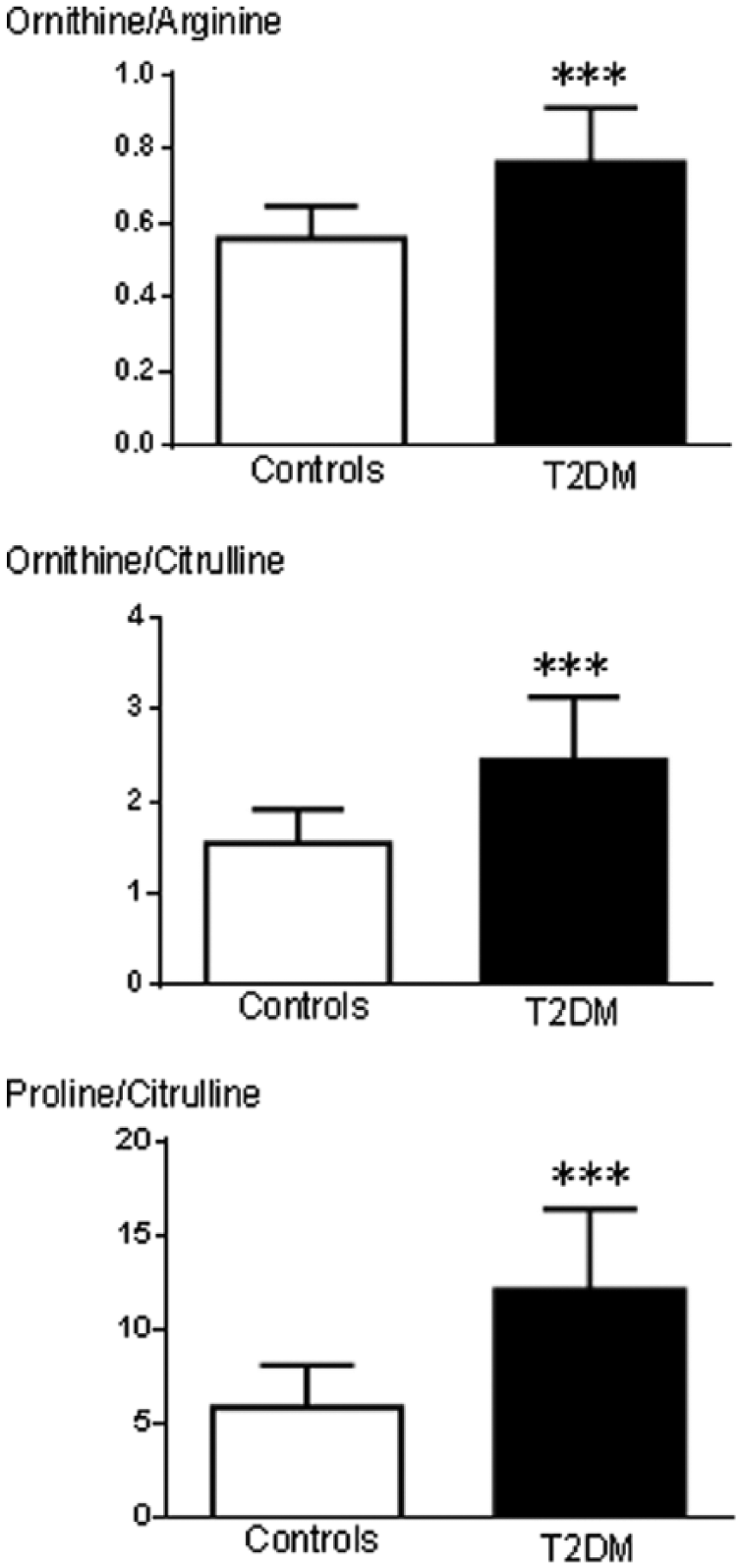
The ratios of amino acids in healthy controls and in patients with type 2 diabetes (T2DM).
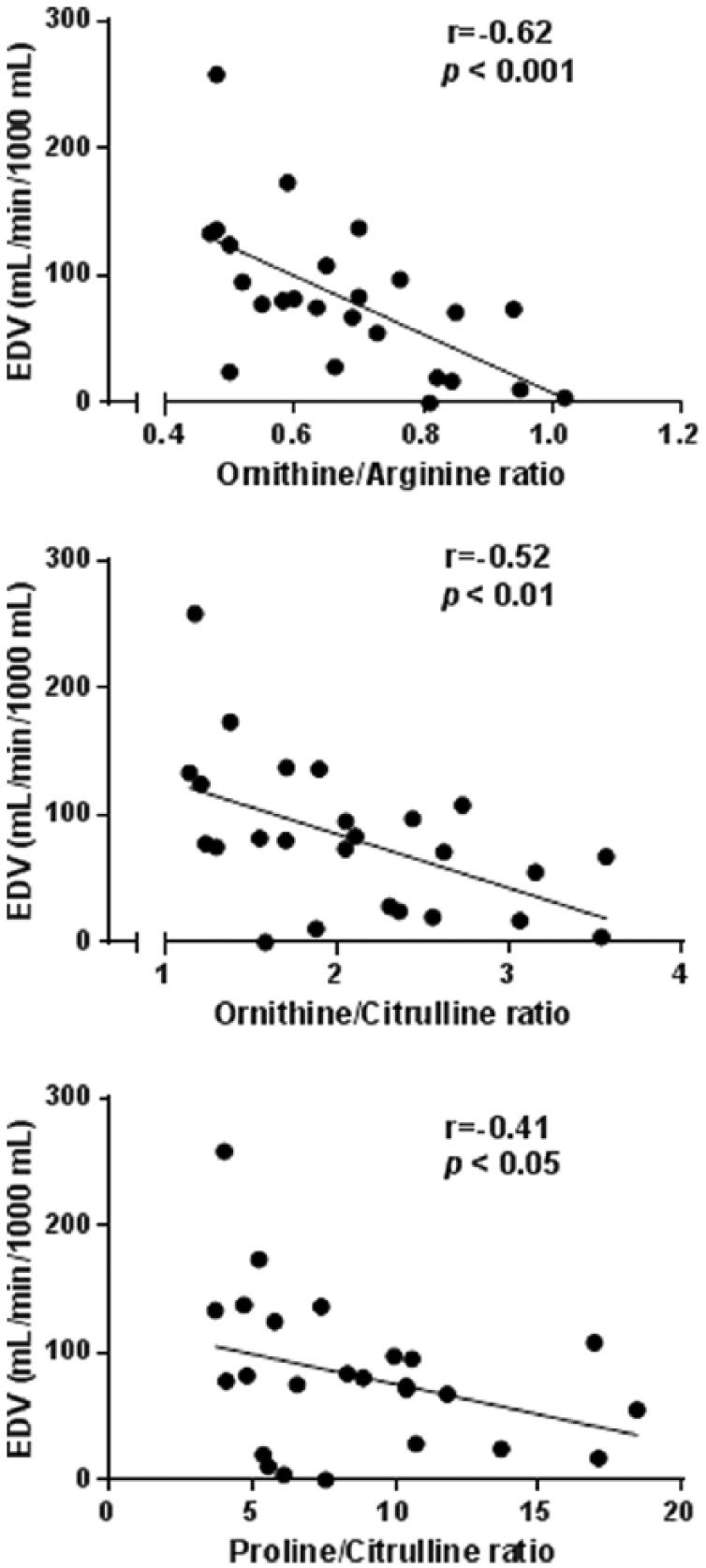
Correlations between ratios of amino acids and endothelium-dependent vasodilatation.
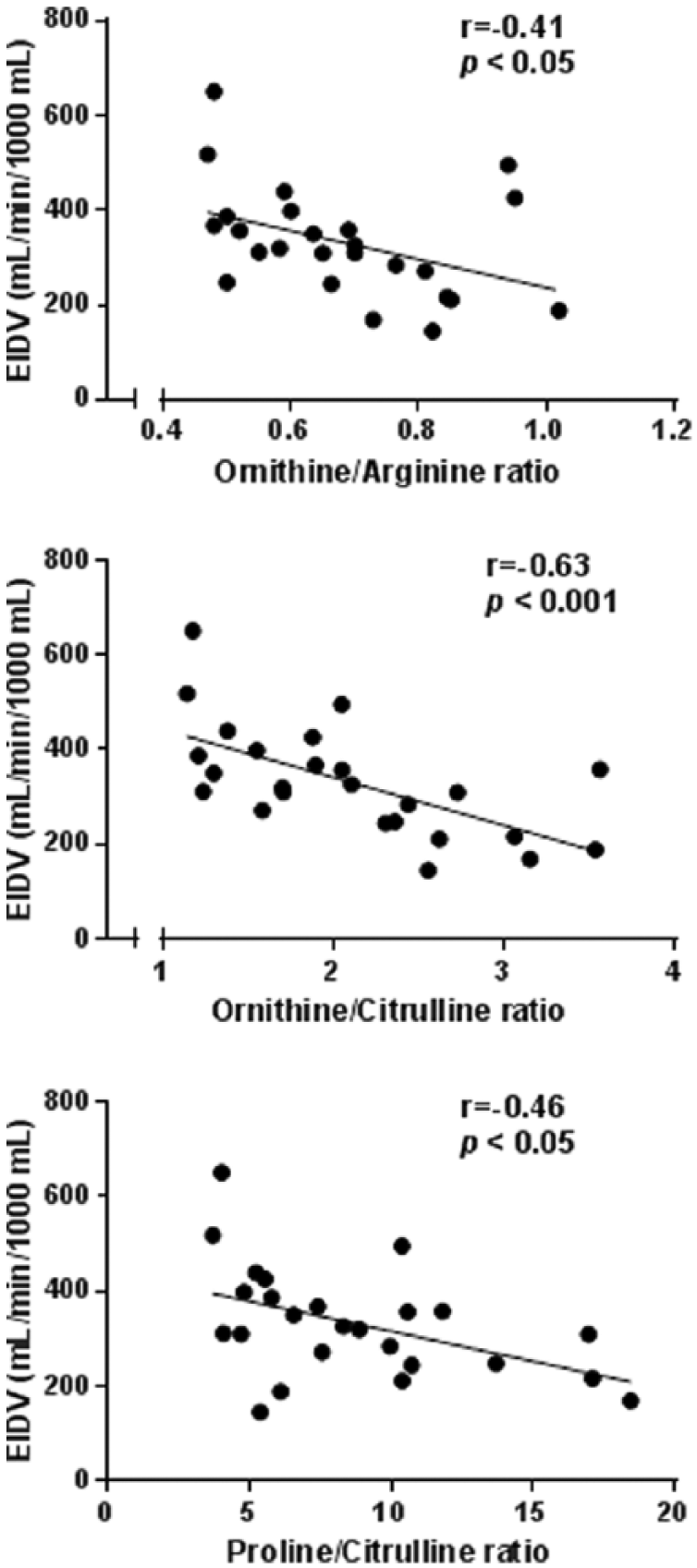
Correlations between ratios of amino acids and endothelium-independent vasodilatation.
Discussion
The main findings of this study are that patients with type 2 diabetes and macrovascular complications have increased ratios of ornithine/arginine, ornithine/citrulline and proline/citrulline in comparison with age-matched healthy controls. Furthermore, these amino acid ratios correlate inversely to EDV and EIDV measured with venous occlusion plethysmography. These observations suggest that patients with type 2 diabetes have increased activity of arginase in relation to NOS and that these changes in enzyme activities are associated with vascular dysfunction. The results also indicate that these amino acid ratios may be useful biomarkers of vascular dysfunction among patients with type 2 diabetes and macrovascular complications.
Although the mechanism behind vascular complications in diabetes is multifactorial, endothelial dysfunction is considered to be a central factor. Endothelial function is a complex process in which NO is a key mediator by regulating vascular tone, inflammation and coagulation.2,3 Thus, reduced bioavailability of NO is a crucial factor contributing to vascular dysfunction in diabetes.
2
The enzyme arginase has emerged as an important regulator of NO bioavailability by competing with NOS for their common substrate
We next investigated whether the changes in arginase-related amino acid ratios reflect vascular function. It was found that the increased ratios of ornithine/arginine, ornithine/citrulline and proline/citrulline all are inversely related to EDV. This observation supports the notion not only that arginase activity is a key mediator of endothelial dysfunction but also that these amino acid ratios could be used as biomarkers of endothelial function. It should be emphasized, however, that our findings might not be specific for the pathology of diabetes. There are several other patient groups with endothelial dysfunction that has been linked to increased arginase activity. These include patients with obstructive sleep apnoea, coronary artery disease, familiar hypercholesterolaemia and sickle cell disease.14,17,18 Interestingly, the amino acid ratios in this study were also inversely related to EIDV induced by SNP. It was further found that EIDV was impaired in patients with diabetes. The latter observation is in line with previous findings 19 and suggests that also the response to exogenous NO is impaired in patients with diabetes. The exact mechanism for this reason is unclear but might be explained by excess of reactive oxygen species that scavenges NO resulting in a decreased response from exogenous NO. Since arginase blockade does not affect EIDV in patients with diabetes, 14 it is unlikely that alterations in arginase activity contribute to changes in EIDV.
Previous studies have investigated metabolism of amino acids related to NOS activity in different patient groups and their significance for disease progression and outcome. However, none of them have related them to vascular function in vivo as in this study. Tang et al. 20 showed a decreased global arginine bioavailability among patients undergoing elective angiography and a correlation to increased incidence of major adverse cardiac events (myocardial infarction, stroke or death). The reduction was driven by increased ornithine and citrulline levels, which is in contrast to the reduced citrulline levels in patients with diabetes and vascular complications in this study. By analysing global arginine bioavailability and arginine/ornithine rations in patients admitted for coronary angiography, Sourij et al. 21 found an inverse relation between global arginine bioavailability ratio and cardiovascular mortality. They also showed that patients with type 2 diabetes had reduced global arginine bioavailability ratio which correlated with the circulating markers vascular cell adhesion molecule-1 (VCAM-1) and intercellular adhesion molecule 1 (ICAM-1). Our results extend these observations by demonstrating that amino acid ratios reflecting increased arginase activity correlates significantly to vascular dysfunction. We did not observe any differences in global arginine bioavailability between healthy volunteers and patients with diabetes or a correlation to EDV. This may not be surprising since the global arginine bioavailability ratio includes the sum of citrulline and ornithine. As citrulline was decreased and ornithine numerically increased in patients with diabetes, this ratio may be unaltered. Our data suggest that the ratio ornithine/citrulline better reflects the arginine/NOS activities and thereby also endothelial function.
There are certain limitations to this study. The study includes a limited number of subjects. However, the sample size was sufficient to detect clear differences in amino acid ratios and in EDV. The patients were not followed over time and it would be of great interest to study whether temporal changes in amino acid ratios also reflect changes in endothelial function. Since the amino acid metabolism is complex several factors including hepatic arginase activity may affect the levels of amino acids in the systemic circulation. However, based on our result there is a clear negative correlation between amino acid ratios (arginase activity) and vascular function suggesting that these are of vascular origin.
Conclusion
Patients with diabetes and macrovascular complications have increased ornithine/arginine and ornithine/citrulline ratios reflecting a shift in metabolism of arginine from NOS to arginase due to increased arginase activity. These changes are inversely related to endothelial function supporting the notion that increased arginase activity contributes to endothelial dysfunction among these patients. These amino acid ratios may be a useful biomarker of vascular function.
Footnotes
Acknowledgements
The expert technical assistance of Ann Lindström is gratefully acknowledged.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by the Swedish Research Council Medicine (10857), the Swedish Heart and Lung Foundation, the Stockholm County Council (ALF), Torsten Söderberg Foundation, Diabetes Research & Wellness Foundation, Karolinska Institutet/Stockholm County Council Strategic Cardiovascular Programme and the Novo Nordisk Foundation.