
Abstract
Purpose:
Cardiovascular disease is the most common cause of mortality in type 1 diabetes; patients with albuminuria are at greatest risk. We investigated myocardial function and premature myocardial impairment in type 1 diabetes patients with and without albuminuria compared to controls.
Methods:
This study included a cross-sectional survey of 1093 type 1 diabetes patients from Steno Diabetes Center and 200 healthy controls. Conventional and tissue Doppler echocardiographic measurements were analysed in multivariable models in normoalbuminuria (n = 760), microalbuminuria (n = 227) and macroalbuminuria (n = 106). Investigators were blinded to degree of albuminuria.
Results:
For the type 1 diabetes patients, mean age was 49.6 years, 53% were men and mean diabetes duration was 25.5 years. In multivariable models systolic velocity s′ did not differ between type 1 diabetes patients with normoalbuminuria and controls (β-coefficient [95% confidence interval]: −0.17 [−0.41; 0.08], p = 0.19), but was impaired between controls and microalbuminuria (−0.53 [−0.84; −0.23], p = 0.001) and macroalbuminuria (−0.59 [−0.96; −0.22], p = 0.002). Diastolic measurements (e′, a′, e′/a′, and E/e′) were all significantly impaired in type 1 diabetes, for example, e′/a′: normoalbuminuria, microalbuminuria and macroalbuminuria versus controls: −0.38 [−0.52; −0.23], p < 0.001; −0.49 [−0.67; −0.32], p < 0.001; and −0.81 [−1.03; −0.59], p < 0.001. In age-related analyses, myocardial impairment occurred prematurely in type 1 diabetes compared to controls (e.g. E/e′ = 8; 9.2 years [normoalbuminuria], 17.3 years [microalbuminuria] and 41.4 years [macroalbuminuria] prematurely, respectively).
Conclusion:
In type 1 diabetes patients with albuminuria, both systolic and diastolic functions are impaired, whereas in patients without albuminuria only diastolic function is affected. Myocardial impairment is detectable many years prematurely in type 1 diabetes, especially in patients with albuminuria.
Introduction
Cardiovascular disease (CVD) is the most common cause of mortality and morbidity in diabetes.1,2 It has been shown that the most common risk factor for CVD in type 1 diabetes (T1DM) is the presence of albuminuria.3–5 Overall, T1DM patients without albuminuria have a mortality rate which is almost similar to the background population, while mortality rates are more than doubled in T1DM patients with albuminuria compared to T1DM patients without nephropathy. 5
Heart disease in diabetes is often characterized by premature coronary atherosclerosis, although a diabetes-specific myopathy without concomitant coronary artery disease (CAD) has been proposed, 6 diabetic cardiomyopathy,7,8 which may lead to heart failure.9–11 Heart failure is a common manifestation of CVD in diabetes patients12–14 and can occur without macrovascular disease.15–17 In a recent register-based study, it was shown that the incidence of heart failure in T1DM patients aged between 41 and 45 years was the same as in individuals from the general population aged 55–64 years. 18
Whereas late changes in myocardial function can be detected by conventional echocardiography, early subclinical changes may be detectable only by advanced echocardiography. It has previously been shown that T1DM patients without known heart disease but with albuminuria have discrete systolic impairment assessed with speckle-tracking echocardiography compared to healthy subjects, whereas patients without albuminuria had a myocardial systolic function similar to healthy controls. 17 It is generally believed that changes in diastole precede changes in systole. Diastolic changes may therefore be the first marker of future myocardial disease and impaired systolic function. Tissue Doppler imaging echocardiography is especially suited for detecting early diastolic changes and has been shown to predict events occurring several years later. 19
Tissue Doppler Imaging echocardiography could therefore be used to potentially detect early myocardial changes associated with T1DM with and without albuminuria and, in particular, diastolic myocardial impairment.
In this study, we therefore studied myocardial function and time-related changes in myocardial function using Tissue Doppler echocardiography in relation to albuminuria in T1DM patients without known heart disease compared to healthy controls.
Research design and methods
Study population
The Thousand & 1 study is a cross-sectional cohort study of T1DM patients without known heart disease. Invitation, screening and inclusion of patients started on 1 April 2010 and inclusion was completed on 1 April 2012. Patients were eligible if they were aged 18 years or older, attending the outpatient clinic at Steno Diabetes Center, diagnosed with T1DM, without known heart disease and willing to participate. The study population and study visit have previously been described in detail. 20 The power calculation for this study was based on previous research from our group 19 indicating that the present number of patients would allow for relevant subanalyses without the risk of type 2 errors. As previously shown, the included study population was representative of T1DM patients without known heart disease followed at Steno Diabetes Center without any major selection bias.
The study was performed in accordance with the second Helsinki declaration and approved by the regional ethics committee (H-3-2009-139) and the Danish Data Protection Agency (00934-Geh-2010-003). All subjects gave written informed consent.
Study visit
Prior to the echocardiographic examination, all patients received study information, signed the consent form and filled out a questionnaire with information about lifestyle factors, including smoking, exercise, alcohol consumption, cardiorespiratory symptoms and the use of medication. Blood pressure and electrocardiogram (ECG) at rest were recorded in the supine position.
Control population
A healthy, non-diabetic control population was sampled from the fifth cross-sectional survey of the Copenhagen City Heart Study (CCHS), which is currently in the inclusion phase. The CCHS is a prospective cardiovascular study of the general population. 21 In the present fifth survey, subjects are invited if they have previously been invited to earlier cross-sectional surveys of the CCHS; also, subjects are randomly selected through the Civil Registration System and invited to participate in order to include up to 5000 subjects for the present survey. So far, around 2500 patients have been included since 2011.
After relevant approval from the Steering Committee of the CCHS was obtained, a total of 200 subjects with similar age and sex distribution were included as controls if they had no history of CVD in the National Patient Registry (LPR), answered ‘No’ to previous CVD on the questionnaire, did not take any cardiovascular medication, did not have diabetes, did not have known kidney disease, did not have known hypertension and had an echocardiography performed with the examination stored in the EchoPac BT11 format, a format which was replaced by EchoPac BT12 in 2012. Subjects who met these criteria were stratified consecutively by inclusion date in 5-year age and gender strata and sampled to reflect age and gender distributions similar to the T1DM patients. Characteristics are shown in Table 1. Echocardiograms were analysed off-line by Dr MTJ using the same methodology as for the Thousand & 1 population described below.
Demographics, type 1 diabetes patients versus controls.
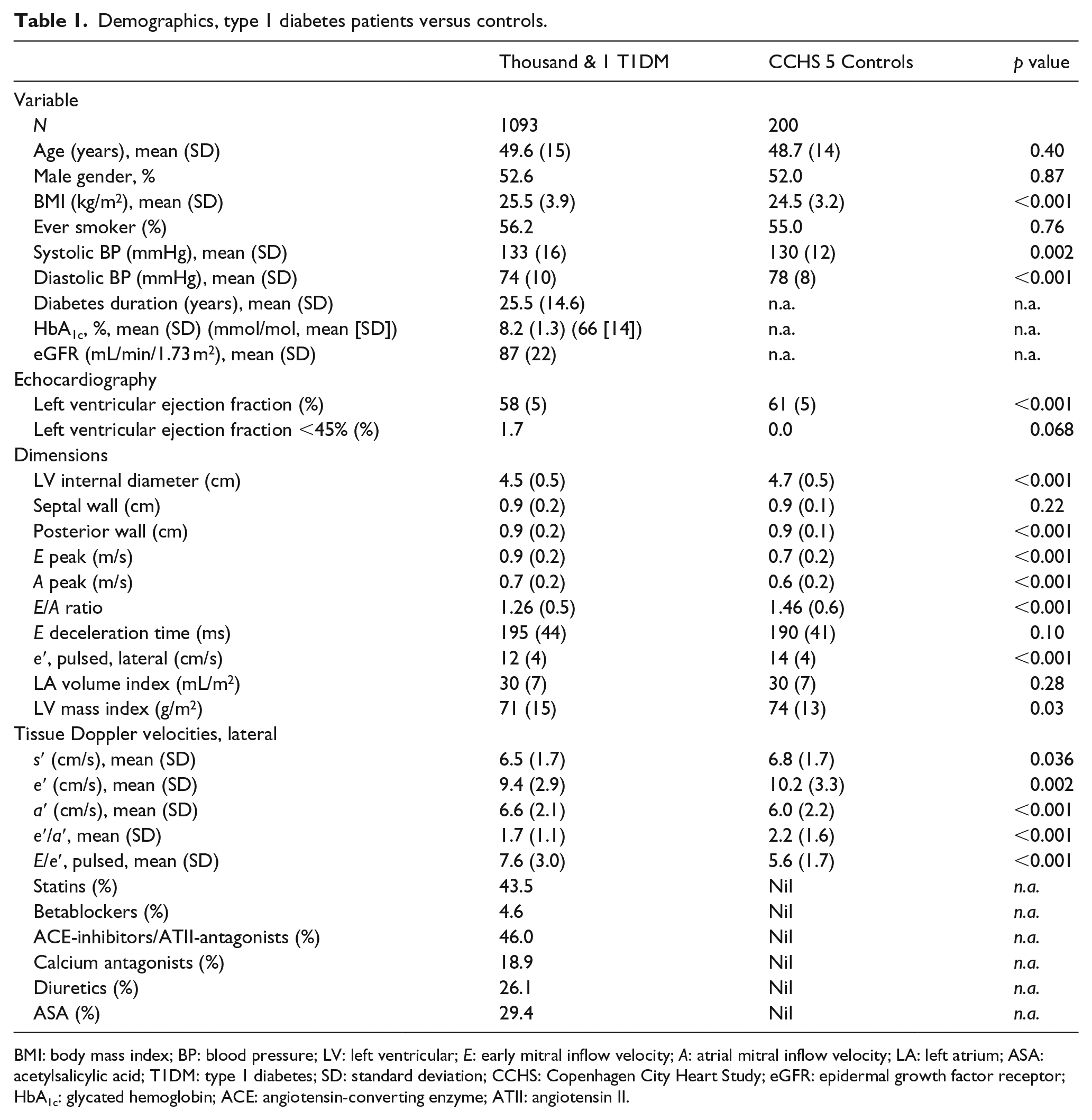
BMI: body mass index; BP: blood pressure; LV: left ventricular; E: early mitral inflow velocity; A: atrial mitral inflow velocity; LA: left atrium; ASA: acetylsalicylic acid; T1DM: type 1 diabetes; SD: standard deviation; CCHS: Copenhagen City Heart Study; eGFR: epidermal growth factor receptor; HbA1c: glycated hemoglobin; ACE: angiotensin-converting enzyme; ATII: angiotensin II.
Echocardiography
Echocardiography was performed with a General Electric, Vivid 7 Dimension imaging system device (GE Vingmed Ultrasound AS, Horten, Norway) with a 3.5-MHz transducer in accordance with the recommendations from the European Association of Echocardiography/American Society of Echocardiography. 22 Echocardiographic examinations were read and analysed using General Electric EchoPAC software (BT11). Three consecutive heart cycles were recorded. Left ventricular ejection fraction was determined by Simpson’s biplane method. Left atrial volume was determined by the recommended biplane area-length method and indexed for body surface area. Left ventricular mass was determined by the linear method and indexed for body surface area. Pulsed-wave Doppler was performed in the apical four-chamber view with the sample volume placed between the mitral leaflet tips to obtain diastolic mitral early (E) and atrial (A) inflow velocities and deceleration time of the E velocity wave. Pulsed-wave early diastolic tissue Doppler velocities (e′) were determined from the apical four-chamber view at the lateral region of the mitral annulus. 23
Tissue Doppler imaging
Pulsed-wave early diastolic tissue Doppler velocities (e′) were determined from the apical four-chamber view at the lateral region of the mitral annulus 23 and used to calculate the E/e′ ratio. Colour Tissue Doppler Imaging velocities were obtained with the highest possible frame rate and analysed off-line. Tissue velocities were sampled from the lateral mitral annulus, since this site has been proven to most accurately correlate with invasive measures of diastolic function. 24 The parameter s′ represents the highest longitudinal myocardial tissue contraction velocity during systole, and e′ and a′ represent the maximal LV early and atrial (late) myocardial tissue relaxation velocities during diastole. Tissue velocity e′ usually decreases and a′ increases with increasing myocardial stiffness and diastolic dysfunction. E/e′ is known to correlate well with left ventricular filling pressure and usually increases with the degree of diastolic dysfunction. The ratio e′/a′ is considered an echocardiographic sign of diastolic dysfunction when the e′/a′ ratio is <1, indicating the aforementioned atrial compensation (a′ increase) as the ventricle stiffens and early relaxation is impaired (e′ decrease). Systolic tissue s′ is a measure of systolic function and is expected to decrease when early systolic impairment is present.
Biochemistry
Information about biochemistry such as HbA1c, p-creatinine and albuminuric status was collected from electronic patient files at Steno Diabetes Center from the ambulatory visit closest to study inclusion, which was maximally ±4 months from inclusion. This information was collected after analysing the echocardiography, ensuring that the investigators were blinded.
Urinary albumin excretion rate (UAER) was measured in 24-h sterile urine collections by enzyme immunoassay. Patients were categorized as normoalbuminuric if UAER, in two out of three consecutive measurements, was <30 mg/24 h, microalbuminuric if UAER was between 30 and 300 mg/24 h and macroalbuminuric if UAER >300 mg/24 h. HbA1c was measured by high-performance liquid chromatography (normal range: 21–46 mmol/mol [4.1%–6.4%]; Variant; Bio-Rad Laboratories, Munich, Germany) and serum creatinine concentration by an enzymatic method (Hitachi 912; Roche Diagnostics, Mannheim, Germany). Estimated growth factor receptor (GFR) was calculated by the Modification of Diet in Renal Disease (MDRD) method. 25
Statistical analysis
All analyses were performed with STATA 12.1 (STATACorp LP, TX, USA). Categorical variables were analysed with the χ2 test and continuous variables with Student’s t test or analysis of variance (ANOVA). Continuous variables were reported as mean (standard deviation [SD]). Multivariable regression models were performed to test the association between myocardial function and albuminuria. The relationship between myocardial function and age was examined more closely; from the regression models, the age and age-difference between controls and T1DM stratified by degree of albuminuria was estimated for specific values of myocardial tissue velocities and ratios in univariable and multivariable regression models including age, systolic and diastolic blood pressure, body mass index (BMI), left ventricular mass index (LVMI) and systolic dysfunction. In these analyses, the estimated age and age differences were predicted for T1DM population mean values of s′, e′, a′, e′/a′ (Table 1) and a value of E/e′ = 8. The analyses of s′, e′ and a′ were solved as linear predictions and e′/a′ and E/e′ as quadratic equations. In these analyses, p values represent tests for differences in β-coefficients, and the T1DM population’s mean values for the covariates were used for the multivariable age estimations (Table 1). A p value of <0.05 was considered statistically significant.
Results
Baseline characteristics
A total of 1093 T1DM patients and 200 controls were included. For the T1DM patients, mean age was 49.6 years, 53% of the population was men, mean HbA1c was 8.2%, mean BMI 25.5 kg/ m2 and mean diabetes duration was 25.5 years. For the controls, mean age was 48.7 years, 52% were men and BMI was 24.5. Clinical characteristics are shown in Table 1.
The population was stratified according to the degree of albuminuria into normoalbuminuria (n = 760), microalbuminuria (n = 227) and macroalbuminuria (n = 106) (Table 2). Patients with microalbuminuria tended to be older than both normoalbuminuria and macroalbuminuria patients, and macroalbuminuria patients tended to be older than patients with normoalbuminuria. BMI, HbA1c and systolic blood pressure increased with the increase in degree of albuminuria, whereas diastolic blood pressure was not associated with albuminuria in the baseline analysis.
Demographics, type 1 diabetes stratified by degree of albuminuria.
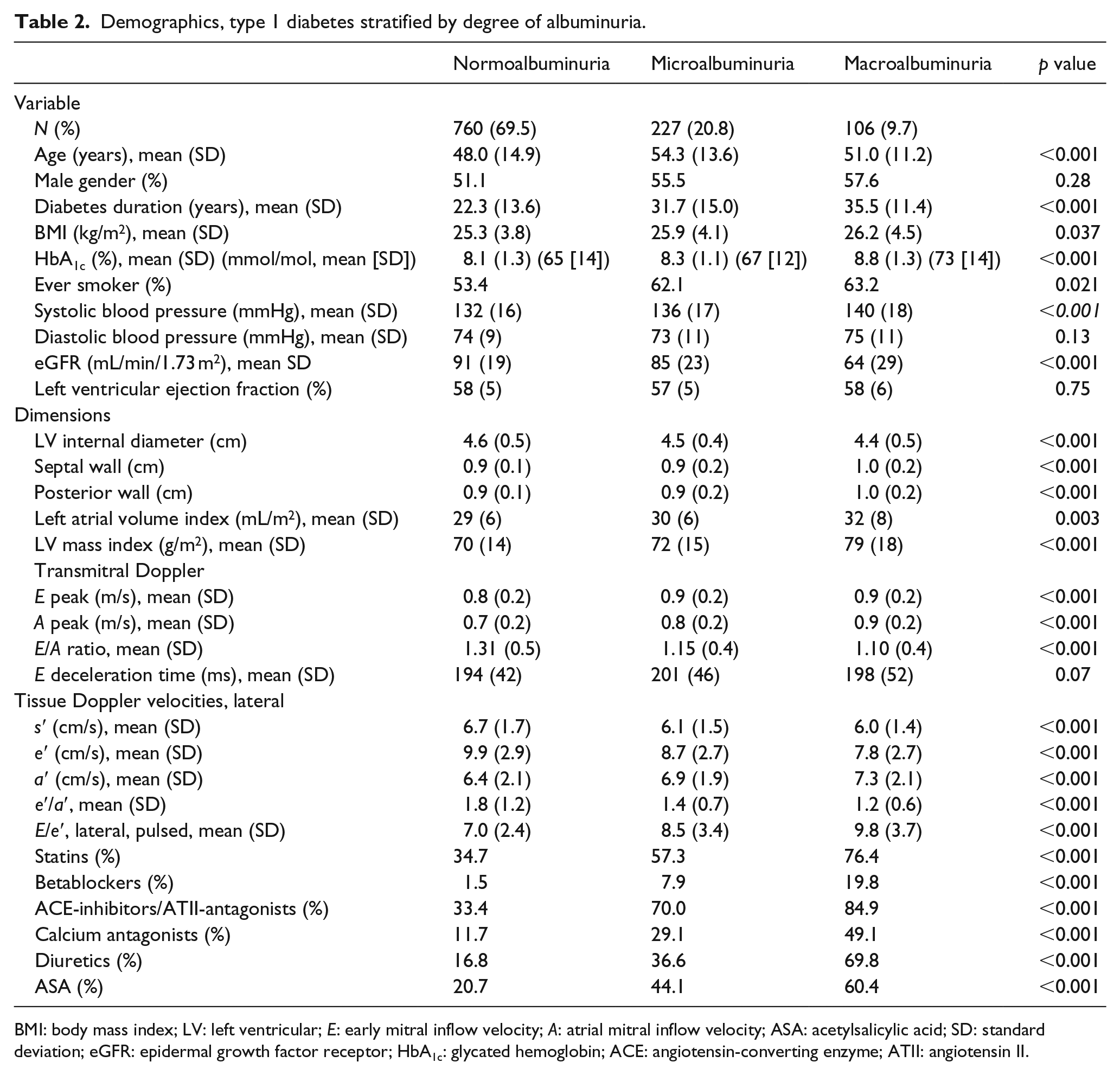
BMI: body mass index; LV: left ventricular; E: early mitral inflow velocity; A: atrial mitral inflow velocity; ASA: acetylsalicylic acid; SD: standard deviation; eGFR: epidermal growth factor receptor; HbA1c: glycated hemoglobin; ACE: angiotensin-converting enzyme; ATII: angiotensin II.
There were significant differences in echocardiographic characteristics between degrees of albuminuria (Table 2); however, although group differences were statistically significant, absolute differences between groups of albuminuria were relatively small.
Tissue Doppler velocities in T1DM versus controls
Differences in myocardial function between T1DM stratified by degree of albuminuria and controls were analysed in multivariable models. In the univariate analyses (Table 1), the age- and sex-matched controls had significantly different s′, e′, a′, e′/a′ and E/e′ compared to patients with T1DM. Table 3 shows differences between the controls and T1DM patients stratified by degree of albuminuria after multivariable adjustments. Interestingly, systolic tissue Doppler velocity s′ did not differ between controls and patients with normoalbuminuria. However, s′ was significantly lower in patients with microalbuminuria and macroalbuminuria. For the atrial diastolic velocity a′ and early diastolic velocity e′, there were significant differences in velocities between T1DM patients and controls irrespective of degree of albuminuria. Also, both the e′/a′ ratio and the E/e′ ratio were significantly different in patients with diabetes compared to controls independent of degree of albuminuria. As shown from the coefficients, increasing degree of albuminuria was associated with a greater decrease in myocardial function compared to the controls.
Myocardial function in T1DM versus controls, association with albuminuria: multivariable model.
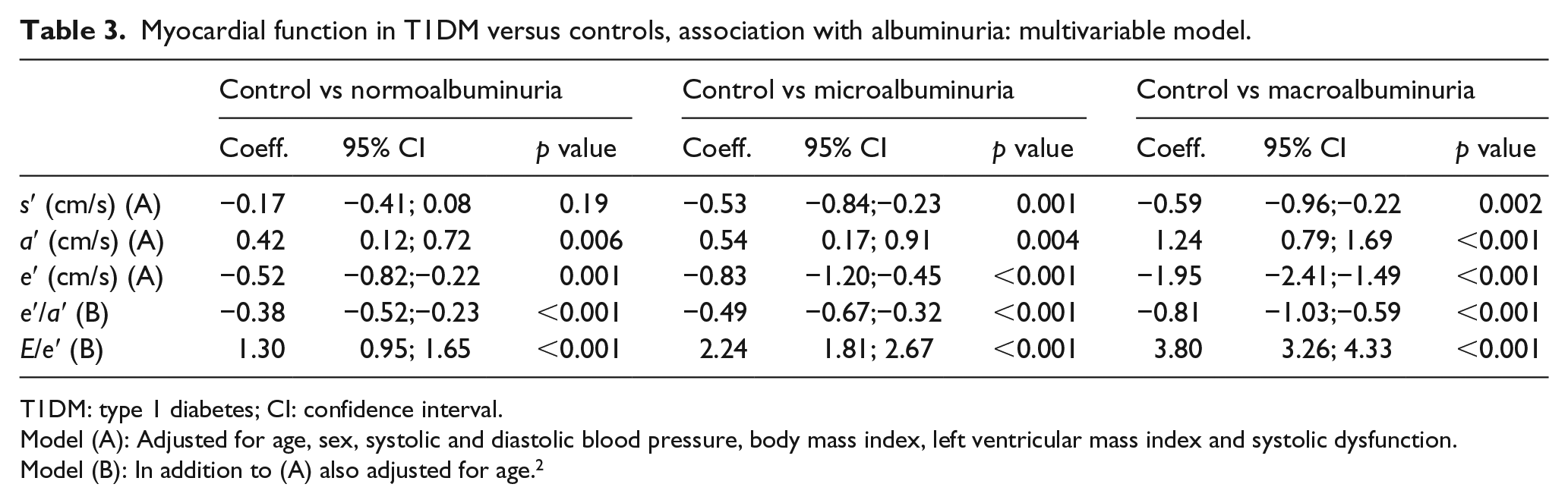
T1DM: type 1 diabetes; CI: confidence interval.
Model (A): Adjusted for age, sex, systolic and diastolic blood pressure, body mass index, left ventricular mass index and systolic dysfunction.
Model (B): In addition to (A) also adjusted for age. 2
The analyses were also performed with the inclusion of use of angiotensin-converting enzyme (ACE)-inhibitors/angiotensin II (ATII)-antagonists in the multivariable model; this, however, did not change the estimates (data not shown).
Tissue Doppler velocities and age
The association between age and tissue Doppler velocities and E/e′ in T1DM patients stratified by degree of albuminuria versus age- and sex-matched controls is shown in Figure S1(a) to (e) (Supplemental data). Tissue Doppler velocities decreased with age. As shown, patients with diabetes and especially patients with microalbuminuria and macroalbuminuria tended to have lower tissue Doppler velocities across the entire age-span (Figure S1(a) to (e)). The relationship between e′/a′ and age (Figure S1(d)) showed a decrease in ratio with age, and the association was graded with decreasing ratios with increase in degree of albuminuria. For E/e′, which is an estimate of left ventricular filling pressure, there was also a graded relationship with controls having the lowest values; values increased in patients with diabetes with increase in the degree of albuminuria (Figure S1(e)).
Estimating premature myocardial impairment
The relationship between myocardial tissue velocities, e′/a′ ratio, E/e′, and age was examined more closely and the age and age-difference between controls and T1DM stratified by degree of albuminuria was estimated for specific values of myocardial tissue velocities and ratios. Tissue Doppler velocities are highly age dependent, and these analyses demonstrate how many years prematurely a T1DM patient with or without albuminuria can expect to have a specific tissue Doppler velocity compared to controls. Mean values for the T1DM population were chosen for the covariates in the multivariable models, and the specific values for which predictions were made were also mean TDI velocities and e′/a′ ratios (Table 1). For E/e′, a value of 8 was chosen (population mean 7.6).
As shown in Figure S2(a) to (e) (Supplemental data), the age differences between controls and T1DM patients after multivariable adjustments were 3.2, 12.8 and 16.7 years for s′ (Figure S2(a)); 3.4, 5.4 and 13.1 years for e′ (Figure S2(b)); 7.2, 9.5 and 19.2 years for a′ (Figure S2(c)); 8.4, 10.8 and 16.0 years for e′/a′ (Figure S2(d)); and 9.2, 17.3 and 41.4 years for E/e′ (Figure S2(e)) for normoalbuminuria, microalbuminuria and macroalbuminuria, respectrively. All differences were statistically different, except for s′ between controls and T1DM patients with normoalbuminuria. Significance levels and values from the univariable analyses are shown in the Supplementary Material.
Discussion
In this study, we find that T1DM patients with albuminuria have impaired tissue Doppler parameters of myocardial systolic and diastolic performance. T1DM patients without albuminuria present with impaired diastolic function that occur several years prematurely when compared to healthy controls. Furthermore, changes in myocardial function can be measured many years prematurely in patients with T1DM compared to controls using tissue Doppler imaging echocardiography.
In the clinical setting, heart failure is a very common complication to diabetes. A specific myocardial disease in diabetes has been proposed, diabetic cardiomyopathy, which is defined as myocardial dysfunction in the absence of other contributing factors such as CAD and hypertension. The myocardial changes relate to myocardial fibrosis and microvascular disease which, in turn, lead to altered myocardial haemodynamics 26 and heart failure. 10 The myocardial tissue becomes ‘stiffer’ which will affect first diastole and later systole. 27 Whereas conventional echocardiography primarily measures systolic function, Doppler measurements can be used to measure changes in blood flow, tissue velocities and diastolic function. Clinical studies of a possible diabetic cardiomyopathy have been small and primarily in patients with type 2 diabetes.10,26,28 Two important reasons may potentially make T1DM a more appropriate model and patient population to study the characteristics of a possible diabetic cardiomyopathy: first, the myocardial changes associated with T1DM are less confounded by lifestyle factors than in T2DM. Second, whereas hypertension and kidney disease are often already present at the time of diagnosis in T2DM, T1DM is usually diagnosed at such an early stage in life, that kidney disease and gross myocardial impairments are usually absent. 29 Overall, the features of T1DM may better allow for studying physiology, pathophysiology and the ‘natural history’ of myocardial disease associated with diabetic kidney disease compared to T2DM.
The question is therefore whether myocardial dysfunction is caused by ‘lack of insulin’ in itself or the consequences thereof. In this study, we find that patients without albuminuria have a systolic function similar to healthy controls. This corresponds to our previous findings using speckle-tracking echocardiography. 17 On the other hand, discrete changes in diastolic function were measureable also in patients without albuminuria, indicating a myocardial involvement related specifically to diabetes.
There is a well-known association between myocardial velocities and age. 19 This was examined further in the present population stratified by degree of albuminuria compared to the controls. We found that across the entire age-span, T1DM and especially T1DM with albuminuria have decreased myocardial tissue velocities. In order to quantify the magnitude of this difference, the age-related differences were analysed for specific velocities of s′, e′, and a′, and the ratios e′/a′ and E/e′. As shown in Figure S1(a) to (e), patients with T1DM and especially T1DM with albuminuria displayed markedly premature decrease in myocardial velocities, the e′/a′ ratio and premature increase in E/e′. After multivariable adjustments, the differences between patients with macroalbuminuria and controls were up to 17 years for s′, 13 years for e′, 19 years for a′, 16 years of the e′/a′ ratio and more than 40 years for E/e′.
The advantage of investigating myocardial function using continuous measurements of TDI is the avoidance of arbitrary classifications of diastolic function. Unzek et al. 30 demonstrated how difficult the classification of diastolic function is even in the presence of the actual images and N-terminal of the prohormone brain natriuretic peptide (NT-proBNP) to help differentiate between grades of diastolic function. As this study demonstrates, the age-related decrease in myocardial function displayed by tissue Doppler velocities is a progressive development without a specific cut-off.
Potential strengths and limitations should be considered. First, the current population is the largest cohort of T1DM patients studied with advanced echocardiography to date; we are therefore able to detect changes in myocardial function not previously described. In addition, patients were included across the entire adult age-span (⩾18 years) and any potential biases from selective age-criteria have therefore been avoided. Furthermore, due to our large sample size spanning across all ages – and within the context of a cross-sectional setup – we are able to describe the ‘natural history’ or at least the age-dependency of different parameters of myocardial function. A limitation of this study may be that the presence of subclinical CAD was unknown. The Thousand & 1 population are followed lifelong every third month at the Steno Diabetes Center and clinical signs or a history of cardiac symptoms will prompt further investigation. A functional test or further studies of possible CAD would, therefore, have strengthened the findings further. Last, the presence of albuminuria in the controls was not assessed.
In conclusion, 1093 T1DM patients without known heart disease were compared to 200 controls using Tissue Doppler echocardiography. We found that tissue Doppler imaging could detect impairment in both systolic and diastolic myocardial functions in T1DM patients with albuminuria. T1DM patients without albuminuria have a systolic myocardial function similar to healthy controls; however, diastolic function was impaired. Across all T1DM patients impairments in myocardial function could be detected many years prematurely compared to healthy controls, and severity increased with the increase in degree of albuminuria.
Footnotes
Acknowledgements
We are indebted to the staff and patients of Steno Diabetes Center for their participation and contribution to The Thousand & 1 Study. M.T.J. is the guarantor of this work and takes full responsibility. M.T.J. researched data and wrote manuscript; P.S., P.R. and J.S.J. reviewed and edited the manuscript; and J.B., T.F.H., H.U.A., S.T., I.G. and T.A. contributed to the discussion and edited the manuscript.
Declaration of conflicting interests
P.R. has board memberships in Astra Zeneca/BMS, Eli Lilly, Janssen, Novo Nordisk, Astellas; has received grants and/or have grants pending from Novo Nordisk, Novartis and Abbott; has received payment for lectures by Astra Zeneca/BMS, Novartis and Sanofi Aventis; and has stocks in Novo Nordisk. H.U.A. is a member of an advisory board of Abbott and has stocks in Novo Nordisk.
Funding
This work was supported by The European Foundation for the Study of Diabetes/Pfizer European Programme 2010 for Research into Cardiovascular Risk Reduction in Patients with Diabetes, Düsseldorf, Germany, and The Danish Heart Foundation, Copenhagen, Denmark. (#: 12-04-R90-A3840-22725).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.