
Abstract
As one of the vascular complications of type 2 diabetes mellitus, the incidence of diabetes retinopathy is greatly increasing worldwide. Both genetic and environmental factors are involved in the pathologies. A meta-analysis was conducted to assess the association between transcription factor 7-like 2 polymorphism (rs7903146) and type 2 diabetic retinopathy. Published literature from PubMed, Web of Science and China National Knowledge Infrastructure were retrieved. Pooled odds ratios with 95% confidence intervals were calculated to estimate the strength of the association. Eight studies including 6422 participants were included in the final meta-analysis. Our analysis provides substantial evidence that the rs7903146 variant is significantly associated with the risk of diabetic retinopathy in Caucasian populations while not in East Asian populations. The variant of rs7903146 appeared more likely to be a promising genetic biomarker of diabetic retinopathy in Caucasians.
Keywords
Introduction
Diabetes has become a major cause of death in people younger than 60 years. 1 Type 2 diabetes mellitus (T2DM) is the most common form of diabetes, accounting for 90% of cases in the world. 2 As one of the most prevalent microvascular complications of T2DM, diabetic retinopathy (DR) remains as the leading cause of preventable blindness in working adults.3,4
DR is associated with both environmental and genetic factors, and its pathogenetic mechanisms are very complex. 5 Many hyperglycaemia-induced metabolic abnormalities are implicated in its pathogenesis, such as increased flux through the polyol pathway, increased advanced glycation endproduct formation, activation of protein kinase C isoforms, and increased hexosamine pathway activity.6,7 Alteration of retinal blood flow, haemostatic abnormalities, metabolic changes, increased oxidative stress, nonenzymatic glycosylation of collagen and neoangiogenesis are observed during long-term hyperglycaemia. 6 As is universally acknowledged, increased vascular permeability is the common pathomechanism in DR.
Transcription factor 7-like 2 (TCF7L2), also known as TCF4, is a protein coding gene. This gene encodes a high mobility group (HMG) box-containing transcription factor that is a key component in the Wnt signalling pathway. The protein has been reported to be associated with blood glucose homeostasis. 8 Several transcript variants encoding multiple different isoforms have been found for this gene. Genetic variants of this gene are implicated in relationship with type 2 diabetes, which also involves in vasculature disorders of the retina. 9 Among these genetic variants, rs7903146 on the chromosome 10q25 region has been the most frequently reported to be strongly associated with T2DM.8,10–29 It was also reported that TCF7L2 gene rs7903146 is linked with microvascular and macrovascular complications, such as coronary artery disease,30,31 nephropathy,20,32,33 retinopathy,32,34–40 and neuropathy. 37 However, some studies demonstrated that TCF7L2 rs7903146 is not consistently associated with DR,32,34,35,38,39 while others suggested TCF7L2 genetic variability contributes to the development of DR.36,37,40 Clarification of the actual role of TCF7L2 rs7903146 in DR process and identification of its function as a genetic risk marker will assist ophthalmologists to predict and debilitate diabetes complication. Thus, a meta-analysis of previous studies of the relationship between the rs7903146 single nucleotide polymorphism (SNP) in TCF7L2 gene and T2DM with DR susceptibility was conducted.
Materials and methods
Information sources and searching strategy
All relevant articles were retrieved by searching the PubMed, Web of Science and China National Knowledge Infrastructure (CNKI), using the following terms: (‘TCF7L2’ or ‘TCF4’ or ‘rs7903146’) and (‘diabetic’ or ‘diabetic retinopathy’ or ‘T2DM’). Final search was carried out on 14 July 2015. Only studies published in the English or Chinese language for which full text was available were included. After abstracts screening, the studies were read in their entirety to assess their appropriateness for the analysis. All references cited in the studies were also checked for additional relevant articles. Meetings abstracts, case reports, editorials, review articles and letters were excluded.
The articles that met the following criteria were included in our meta-analysis. (1) Studies that estimated the relationship between rs7903146 polymorphism and the T2DM with DR. (2) Study design was limited to case-control study, cohort study, or population-based epidemiologic survey. (3) Studies that provided sufficient data to estimate an odds ratio (OR) and its 95% confidence interval (CI). (4) For those repeated reports, the latest report or the report with maximum sample size was selected. Diabetes was diagnosed according to World Health Organization (WHO) or American Diabetes Association (ADA) criteria. 41 All patients underwent a thorough medical history and biochemical tests. DR was assessed by trained ophthalmologists.
Data extraction and quality assessment
In order to retrieve articles as completely and correctly as possible, two investigators independently conducted the search and extracted data based on the inclusion criteria. From each included study, the following information was extracted: first author, journal, year of publication, ethnicity of study population, average age, mean T2DM duration, mean HbA1C, gender, body mass index (BMI), number of cases and controls, frequency of risk allele T. When discrepancies were observed, they were settled by discussion and consensus among all the authors.
Statistical analysis
All statistical analyses were conducted using Stata V.11.0 (Stata Corp, College Station, TX, USA) and p < 0.05 was considered to be statistically significant. The pooled ORs of responders versus non-responders with 95% CIs were used to measure the strength of the association between the rs7903146 polymorphism and T2DM with DR. The following four comparisons were calculated: TT versus CC, TC versus CC, TT + TC versus CC and allele T versus C. Heterogeneity between studies was quantified using the Q statistic: if p < 0.05, heterogeneity was considered statistically significant and random effects models were selected for a more accurate calculation. Otherwise, the fixed-effects models were used. In this study, random effects models were preferential for simplicity. Visual inspection of the funnel plots was conducted to identify any potential publication bias. In addition, Egger’s tests and Begg’s tests were carried out to examine the degree of publication bias (p < 0.05 was considered indicative of statistically significant publication bias). We also undertook a sensitivity analysis by omitting one study at a time to assess the stability of the meta-analysis results. Of note, because all the subjects included in the meta-analysis were patients, there was no need to check for departure from Hardy–Weinberg equilibrium. 42
Results
Characteristics of the available studies
In our initial search, a total of 312 potentially relevant articles in the PubMed, Web of Science and CNKI databases were collected, with 114 duplicates. After careful retrieval and close reading, eight studies comprising 6422 cases were finally included for the meta-analysis (Figure 1). Table 1 lists the general characteristics of each included study. Except Fu et al.’s 38 study published in 2006, all the other included studies were published between 2010 and 2014. All studies were case-control studies, of which two studies were performed on East Asian and six on Caucasian. Three studies had larger sample sizes,36,38,39 the total cases were 1139, 1129 and 1206, respectively. Other five studies had relatively small sizes (numbers of cases < 1000).32,34,35,37,40 Table 2 lists the detailed allele and genotype distributions of each eligible study. The frequencies of variant T allele of rs7903146 in all participants were similar among the studies of Caucasian subjects, ranging from 33.5% to 44.9%. Two studies on the East Asian participants reported a much lower frequency of T allele, which are 4.47% and 6.997%, respectively.35,38 For the genotype comparisons in these studies, six studies provided the number of TT/TC/CC in cases and controls, while two studies focused on the comparison of TT + TC versus CC for the shortage with T allele.
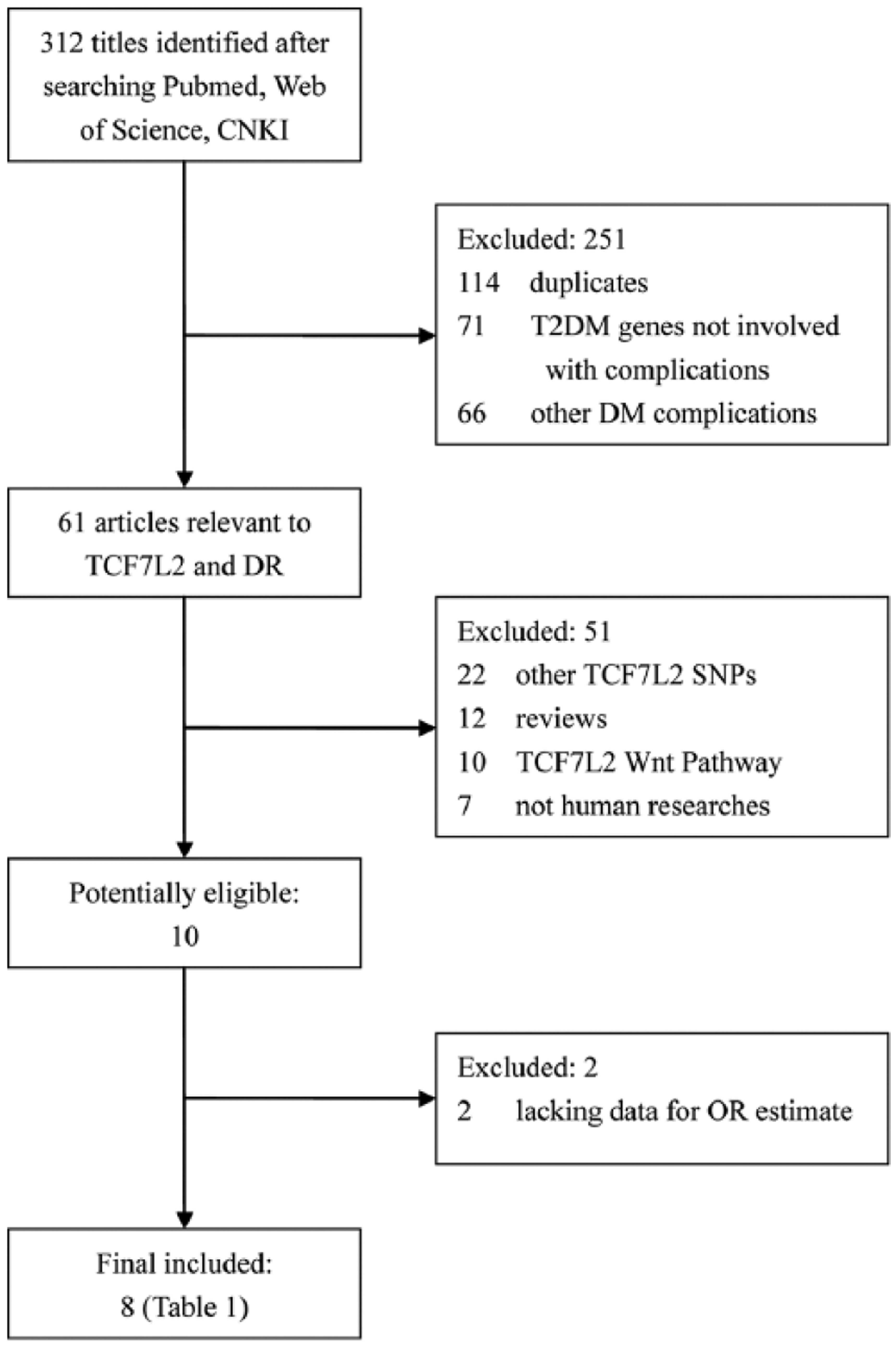
Flow diagram of the identification of relevant studies. Results of literature search strategy. Flow diagram depicts the screening process of retrieved articles, including the reason for and number of exclusions.
General characteristics of the included studies.
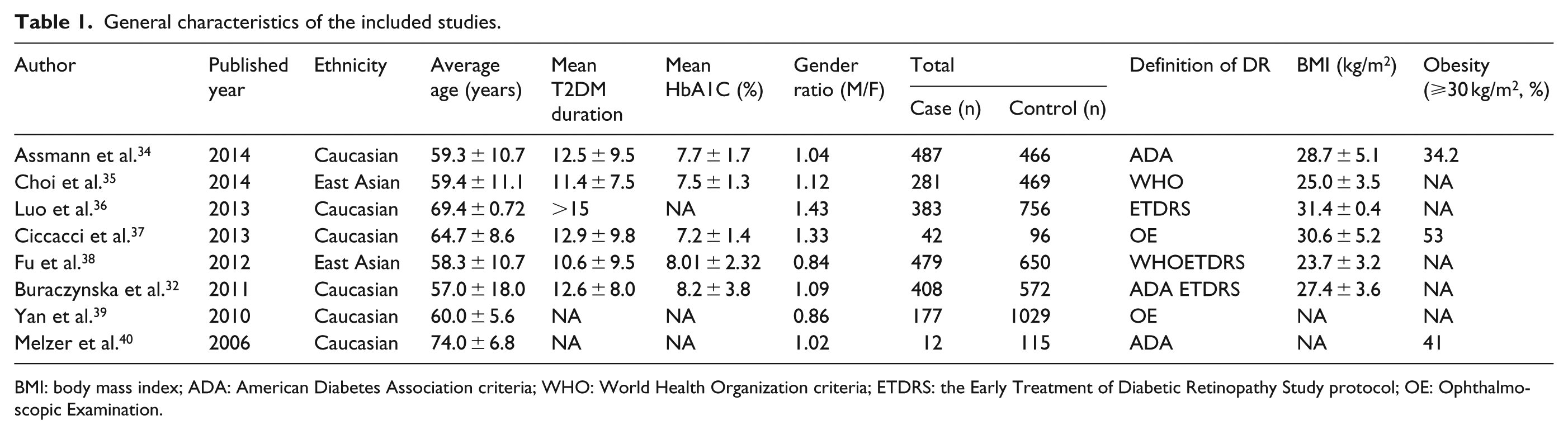
BMI: body mass index; ADA: American Diabetes Association criteria; WHO: World Health Organization criteria; ETDRS: the Early Treatment of Diabetic Retinopathy Study protocol; OE: Ophthalmoscopic Examination.
Distribution of the rs7903146 genotype for cases and controls and the allele frequencies.
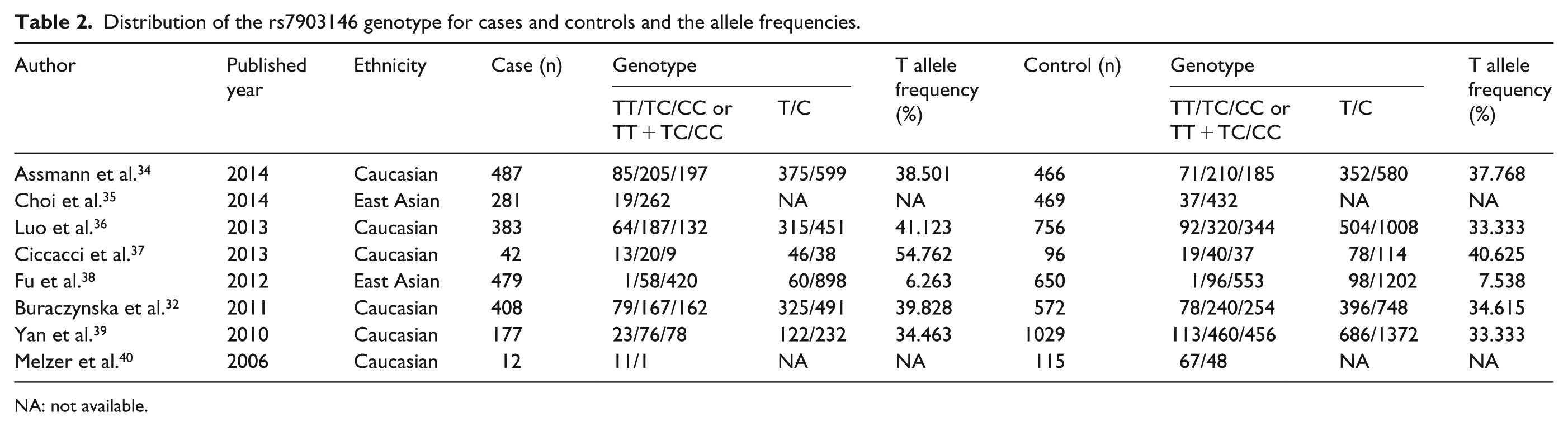
NA: not available.
Main results of meta-analysis
Table 3 shows the main results of this meta-analysis. In the overall analysis of the association between rs7903146 polymorphism of TCF7L2 gene and susceptibility of T2DM with DR, a significant p value was observed for TT versus CC (OR = 1.47, 95% CI = 1.19–1.81, p = 0.000). No significant difference was found for other genotype comparisons (TC vs CC: OR = 1.08, 95% CI = 0.86–1.35, p = 0.497; TT + TC vs CC: OR = 1.14, 95% CI = 0.91–1.44, p = 0.245; T vs C: OR = 1.16, 95% CI = 0.99–1.36, p = 0.074). Subgroup analysis was performed based on ethnicity. The results of analyses performed on Caucasian participants suggested a significant association between rs7903146 polymorphism and the susceptibility of T2DM with DR in TT versus CC and T versus C genotype comparisons (TT vs CC: OR = 1.47, 95% CI = 1.16–1.87, p = 0.001; TC vs CC: OR = 1.15, 95% CI = 0.91–1.45, p = 0.246; TT + TC vs CC: OR = 1.27, 95% CI = 0.98–1.63, p = 0.066; T vs C: OR = 1.21, 95% CI = 1.05–1.41, p = 0.011; Figure 2). However, only Fu’s study was included in the subgroup Asian group and no obvious evidence of associations were found in all genetic models (Table 3).
Determination of the genetic effect of rs7903146 polymorphism on T2DM-DR and subgroup analyses.
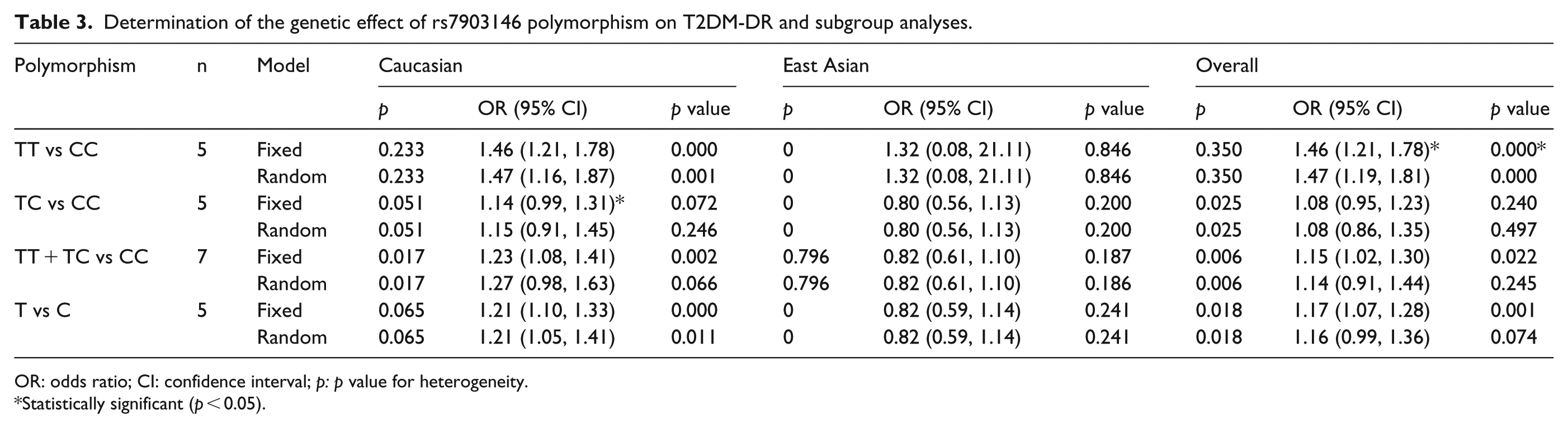
OR: odds ratio; CI: confidence interval; p: p value for heterogeneity.
Statistically significant (p < 0.05).
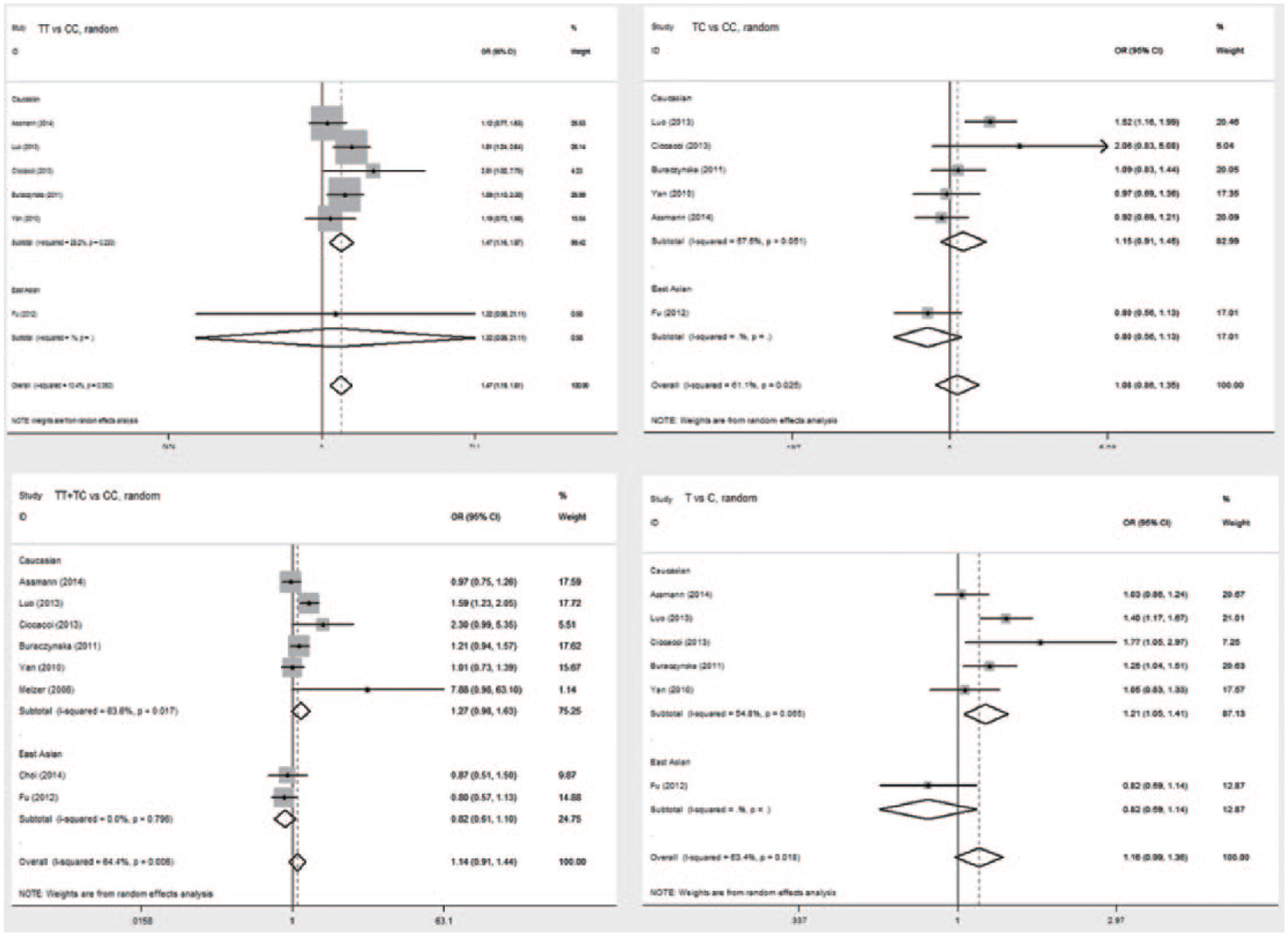
Forest plots of rs7903146 polymorphism and T2DM-DR susceptibility in overall and subgroup comparisons based on ethnicity.
Test for heterogeneity
Significant heterogeneity was found in the following three genetic models: TC vs CC – p heterogeneity = 0.025; TT + TC vs CC – p heterogeneity = 0.006; T vs C – p heterogeneity = 0.018. When patients were stratified based on ethnicity, the heterogeneity of the Caucasian samples disappeared in the following two genetic models: TC vs CC – p heterogeneity = 0.051; T vs C – p heterogeneity = 0.065. The heterogeneity of the Caucasian samples still existed in TT + TC vs CC group (p heterogeneity = 0.017). Data of heterogeneity test are listed in Table 3.
Sensitivity analyses
Sensitivity analyses were performed after sequential removal of each of the included studies to examine the influence of each individual dataset on the pooled ORs. No single study qualitatively changed the pooled ORs in most comparison model, which indicated that the results of this meta-analysis were basically stable and robust (Figure 3). Only when excluding the data of Fu et al., the statistical p changed to be significant for T versus C comparison (OR = 1.21, 95% CI = 1.05–1.41).
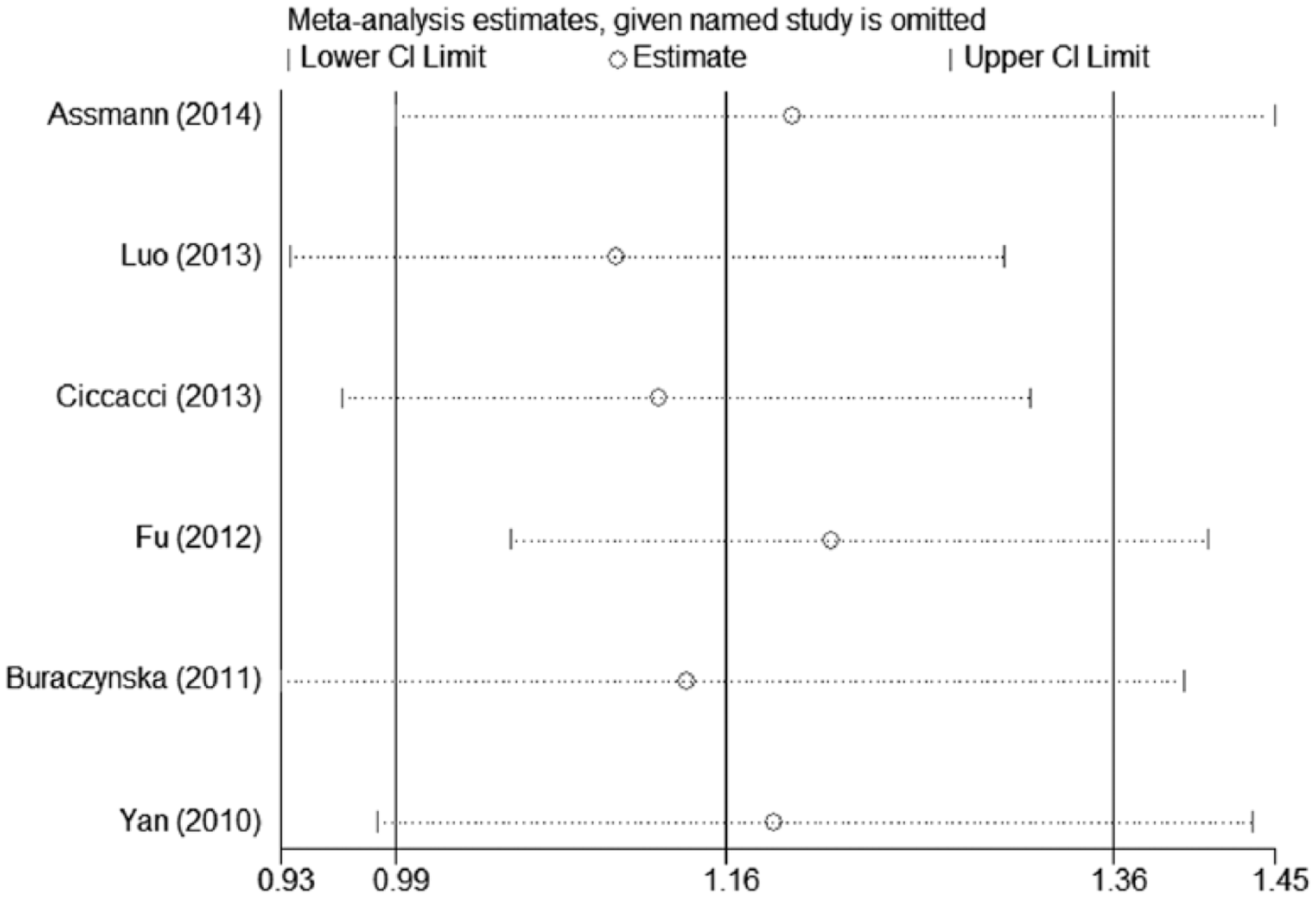
Sensitivity analyses through deletion of one study at a time to reflect the influence of the individual dataset to the pooled ORs.
Publication bias diagnostics
Funnel plots and Egger’s tests were used to assess potential publication biases of the literatures. The shapes of the funnel plots did not reveal any evidence of obvious asymmetries (Figure 4). Similarly, the results of Egger’s tests and Begg’s tests did not show significant publication biases in the current meta-analysis.
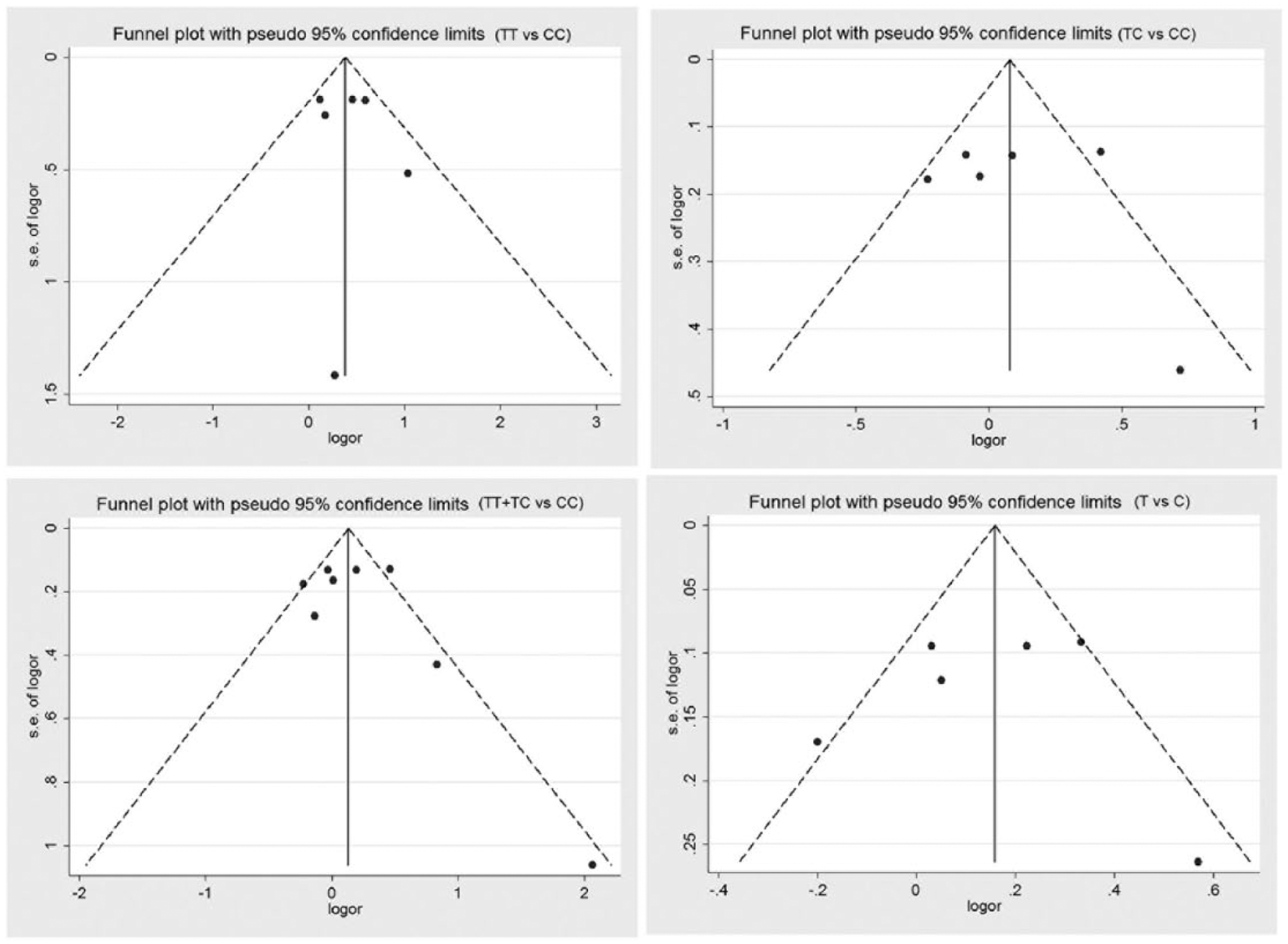
Funnel plots of studies included in the meta-analysis. The axis represents SE of ln (OR) and the horizontal axis represents ln (OR).
Discussion
Various genes have been studied in T2DM susceptibility, and TCF7L2 gene has been considered the strongest genetic determinant for the risk of developing T2DM.8,43,44 However, only a few studies have investigated the gene polymorphisms associated with DR. Ciccacci et al.’s 37 findings suggest that subjects carrying the rs12255372 or rs7903146 variant had a higher risk of developing DR than non-carriers, while the rs7901695 variant was not associated with it. In Chinese population, although significant differences were not observed, three TCF7L2 SNPs (rs6585205, rs7903146 and rs11196218) were considered potentially linked with DR. 38 We therefore focused on the association between the most studied one (rs7903146) in TCF7L2 gene and the risk of DR. We found a significant association between rs7903146 and DR in the overall populations, especially in Caucasian populations. T allele might be a DR-causing locus and the homozygote genotype had a stronger effect than the heterozygote genotype.
Nevertheless, there are only two studies focusing on the relationship between rs7903146 SNP and DR in East Asian populations. The rs7903146 SNP variant (T allele) in TCF7L2 is quite rare among East Asian population. In the 1879 qualified cases, there were only 217 heterozygotes and 4 variant homozygotes.35,37 No significant association between this variant and the phenotypes was found in East Asian ethnic groups (the T allele frequencies among East Asian groups are only 4.47% for Choi’s study and 6.997% for Fu’s study). Since the rarity of this particular SNP among East Asians might have reduced the statistical power, no significant difference was observed. To draw an accurate conclusion, more studies with large sizes are needed to confirm the impact of this TCF7L2 variant on T2DM with DR in East Asian.
In the overall population, the results suggested a significant difference in the comparison of TT versus CC, while the significance of the difference disappeared in the comparison of T versus C (OR = 1.16, 95% CI = 0.99–1.36, p = 0.074). However, the sensitivity test suggested that the exclusion of the study by Fu would affect the assessment of significance. Fu’s study focused on East Asian and had limited number of patients carrying T allele. Thus, it can be inferred that the data in Fu et al.’s 38 study have impacted the evaluation of the role of T allele in the DR susceptibility.
Heterogeneity is a potential problem that might affect the results of our meta-analysis. Significant heterogeneity was observed in the overall population analysis in the following genetic groups: TC versus CC, TT + TC versus CC and T versus C. Heterogeneity may have arisen from differences in the patients’ genetic backgrounds, Western-style diet, living environments, a sedentary lifestyle, age, duration of diabetes or genotyping methods collected in different studies. After the subgroup analysis based on ethnicity, the heterogeneity disappeared in Caucasian population in TC versus CC and T versus C groups.
The TCF7L2 is one of the polymorphisms found to be related with diabetes, 28 and subsequently, its association has been confirmed in several studies,8,29 making it among the most reproducible markers of T2DM. Studies have shown that this SNP leads to conformational changes in chromatin structure according to the allele type. In particular, the risk allele (T) induces an open conformation of the chromatin, resulting in an increased transcriptional activity and TCF7L2 messenger RNA (mRNA) levels.45,46 It has been demonstrated that the increase of expression of TCF7L2 leads to a progressive reduction of glucose tolerance in vivo. 47 TCF7L2 may impair a patient’s ability to control serum glucose levels, and chronic hyperglycaemia may increase the risk of DR.
To our knowledge, there are few reviews involving the association between polymorphisms and DR. Although one review tried to examine the association, the limitations of data they collected make it difficult to draw conclusions. We significantly increased the statistical power of our meta-analysis by including a substantial number of cases and controls from published studies. Other than the published data from selected databases, some eligible studies that have not been published were also researched for data in the publically available genome-wide association studies (GWASs) or on HuGeNEt. GWAS of DR in Taiwanese, 48 Mexican-Americans 49 and Chinese 50 population identified several DR-associated SNPs which involved inflammation, oxidative stress or cell adhesion for the development and progression of DR. However, the TCF7L2 rs7903146 variant was not reported in these large studies and data were unavailable, and publication bias therefore appeared as an irresistible fact. Otherwise, the qualities of the studies identified in our meta-analysis were satisfactory and met our inclusion criteria. The methodological issues of meta-analysis, such as heterogeneity and the stability of results, were all carefully investigated. To explain the results, some limitations of the current meta-analysis should also be acknowledged. First, due to the lack of retinopathy information from the eligible studies, we were unable to classify DR types into non-proliferative diabetic retinopathy (NDPR) and proliferative diabetic retinopathy (PDR), and the subgroup analyses based on DR types were not conducted. Second, due to the limited availability of published results, only eight publications were included in our meta-analysis, and this low number is bound to bias the analyses results. With more GWAS research, gene study of TCF7L2 in DR will be brought to the forefront in the near future. We expect that more studies with larger samples and case-controlled trials will become available. In summary, this meta-analysis provided evidence that the TCF7L2 variant rs7903146 is associated with T2DM-DR susceptibility in Caucasians while not associated with the risk in East Asian. The T allele variant of rs7903146 might act as a promising genetic risk marker for predicting DR in Caucasians. Well-designed case-control studies with adequate numbers of cases are warranted to confirm our findings, especially in East Asian populations.
Footnotes
Acknowledgements
The authors would like to thank all those who are not listed as co-authors, for their assistance in searching papers, obtaining full-text articles and analysing the results.
Declaration of conflicting interests
The authors have no relevant conflicts of interest to disclose.
Funding
This research was supported by Jiangsu Provincial Special Program of Medical Science (BL2014089).