
Abstract
Purpose:
To examine the associations between the homeostatic model assessment for insulin resistance and self-reported muscular strengthening activity in a nationally representative sample of euglycaemic US adults.
Methods:
Sample included euglycaemic adults (⩾20 years of age (n = 2009)) from the 1999 to 2004 National Health and Nutrition Examination Survey. Homeostatic model assessment for insulin resistance was categorized into quartiles and was the primary independent variable of interest. No reported muscular strengthening activity was the dependent variable.
Results:
Following adjustment for covariates, those with homeostatic model assessment for insulin resistance values in fourth (odds ratio: 2.04, 95% confidence interval: 1.35−3.06, p < 0.001) quartile were found to have significantly greater odds of reporting no muscular strengthening activity. Following further adjustment for non-muscular strengthening activity specific aerobic leisure-time physical activity, results remained significant for the fourth (odds ratio: 2.30, 95% confidence interval: 1.50−3.52, p < 0.001) quartile. A significant trend was seen across quartiles of homeostatic model assessment for insulin resistance for increasing prevalence of no muscular strengthening activity (p < 0.001).
Conclusion:
Having a higher homeostatic model assessment for insulin resistance value is associated with greater odds of reporting no muscular strengthening activity among euglycaemic US adults. This implies that subjects with an increasing degree of insulin resistance are more likely to not engage in muscular strengthening activity, an exercise modality that has been shown to reduce the risk of several cardiometabolic diseases and improve glycaemic status.
Keywords
Introduction
The homeostatic model assessment for insulin resistance (HOMA-IR) has been extensively used as a measure for insulin resistance (IR) in epidemiological studies. Greater levels of IR have been shown to be highly associated with incidence of type 2 diabetes1,2 and cardiovascular disease (CVD).3–6 Previous studies using surveillance data have estimated that HOMA-derived IR 7 is highly prevalent, manifested in approximately one-third of US adults who are without diabetes or impaired fasting glucose.
Traditionally, muscular strengthening activity (MSA) has been examined as an independent predictor of IR in subjects without diabetes.8–15 For example, Miller et al. 9 reported a significant reduction in both basal insulin levels (37.5%, p < 0.05) and insulin levels in response to an oral glucose tolerance test (OGTT) (18%, p < 0.05) in eight young healthy male subjects following a 10-week high-resistance, isotonic weight-lifting programme. Cheng et al. 12 investigated the associations between volumes of MSA and IR, measured via the quantitative insulin sensitivity check index (QUICKI), in subjects without diabetes utilizing data from the 1999 to 2004 National Health and Nutrition Examination Survey (NHANES). Results revealed significantly higher QUICKI levels in subjects reporting ⩾1 day/week of MSA (p < 0.05). Following adjustment for covariates, results remained significant in females but not in males. Significance was only seen in volumes of MSA ⩾3 days/week (p < 0.05) in males.
Currently, no studies have examined these associations with MSA using HOMA-IR as the independent variable. This unique approach, defined as using a disease or adverse metabolic condition as the independent variable and physical activity (PA) as the dependent variable, has been used in a limited number of studies.16–22 Moreover, this approach allows for a clinical interpretation of surveillance data, by providing potential insight into MSA patterns in high-risk subjects. The purpose of this study was to investigate the associations between quartiles of HOMA-IR and self-reported MSA in a representative sample of euglycaemic adults in the United States. To the extent of our knowledge, this is the first study to examine the associations between HOMA-IR and MSA patterns using this unique approach.
Methods
This study utilized 6 years of data from the 1999 to 2004 NHANES, a continuous survey conducted by the National Center for Health Statistics Centers for Disease Control and Prevention. 23 The NHANES was designed to provide national estimates of the health and nutritional status of non-institutionalized US civilians over the age of 2 months. The total 1999–2004 NHANES sample was 31,126. For this study, we utilized data from subjects aged 20 years and older. Out of the 15,332 subjects who participated in the 1999–2004 NHANES, we excluded 833 women who reported being pregnant and 8781 subjects who were non-fasted. Subjects with diabetes (n = 690) or pre-diabetes (n = 1617) were excluded from the study as well. Following exclusion of those with missing data (n = 1402) for any variable included in the analysis, 2009 remained in our analysis as eligible study subjects. The final sample met the following conditions: (1) adult men and women ⩾20 years of age; (2) attended a morning medical examination in a mobile examination centre following an overnight fast; (3) if female, non-pregnant; (4) had complete data on all the variables of interest and (5) were euglycaemic (fasting glucose <100 mg/dL) and answered no to the question DIQ010: Other than during pregnancy, have you ever been told by a doctor or health care professional that you have diabetes or sugar diabetes?
Muscle strengthening activity
Current recommendations set forth by the US Department of Health and Human Services (DHHS) state that the healthy population should participate in MSA 2 or more days per week. 24 The dependent variable in this study was calculated from ‘self-reported’ MSA. The final sample provided responses to the following items which came from the PA questionnaire file item PAD440: Over the past 30 days, did you do any physical activities specifically designed to strengthen your muscles such as lifting weights, push-ups or sit-ups? Include all such activities even if you have mentioned them before in the past 12 months. MSA was dichotomized in the following manner: no MSA and any MSA. No MSA was the outcome of interest.
Insulin resistance
The primary independent variable of interest was IR. We used the HOMA-IR as a measure for IR, calculated using the equation by Matthews et al.: 25 [fasting serum insulin (mU/mL) × fasting plasma glucose (mmol/L)]/22.5. Age-adjusted log-transformed quartiles of HOMA-IR were created using every 25th percentile based on the early-morning fasting weight specific to NHANES: Q1 (<0.20), Q2 (⩾0.20 and <0.37), Q3 (⩾0.37 and ⩽0.55) and Q4 (>0.55).
Covariates
For prevalence rate calculations, age was categorized into five levels: 20–29, 30–39, 40–49, 50–59 and ⩾60 years. Age was analysed continuously in the logistic regression analysis. Four categories of race were created: non-Hispanic White, non-Hispanic Black, Mexican American and Other. Education was categorized into four groups: less than high school, high school graduate or General Educational Development (GED), some college and college graduate. Three categories of smoking were created: current smoker, former smoker (quit within last 6 months) and non-smoker. Three categories of alcohol consumption were created based on the US Department of Agriculture and DHHS gender-specific cut-points: non-drinker (0 drinks/day), moderate [>0 and ⩽1 (women), >0 and ⩽2 (men) drinks/day] and above moderate [>1 (women), >2 (men) drinks/day]. 26 For prevalence rate calculations, waist circumference (WC) was dichotomized: men (elevated: ⩾102 cm, normal: <102 cm) and women (elevated: ⩾88 cm, normal: <88 cm). 27 In the logistic regression analysis, WC was analysed continuously. Aerobic leisure-time physical activity (LTPA) was categorized into three levels: 0 min/week, >0 to <150 min/week and meeting the 2008 DHHS PA recommendations ⩾150 min/week. 24
Statistical analysis
The data in this study were initially managed using Statistical Analysis System (SAS) 9.2, 28 which was used to conduct both complex variable recodes and data coding validation. The SAS survey procedures were then used to conduct the analysis, incorporating sampling weights within the context of the correlated multi-stage complex sampling design inherent to NHANES. Age-adjusted prevalence estimates were calculated using PROC SURVEYREG. Non-overlapping 95% confidence intervals (CIs) with coinciding p-values illustrate significance (p < 0.05). Logistic regression (PROC SURVEYLOGISTIC) analysis was used to test the null hypotheses that individual regression coefficients are equal to zero for each quartile of HOMA-IR. Three logistic regression models were created. The crude model included the primary independent variable HOMA-IR unadjusted. The second model adjusted for age, race, gender, education, smoking, alcohol consumption, WC and HOMA-IR, and the third model further adjusted for other non-MSA specific aerobic LTPA. Initially, we included CVD status, hypertension and arthritis in the fully adjusted model. After a backward selection process, these covariates were eliminated from full analysis in order to ensure a parsimonious model.
Results
Table 1 provides a summary of the study sample characteristics. Table 2 provides prevalence estimates for reporting no self-reported MSA. The prevalence of reporting no MSA was significantly higher in subjects in the third (76.44%, 95% CI: 71.59−81.29) and fourth (80.83%, 95% CI: 75.79−85.87) quartiles of HOMA-IR compared to those in the first (64.35%, 95% CI: 59.69−69.01). No significant differences were found for prevalence of no MSA in the second quartile of HOMA-IR compared to the first. A significant trend was seen across quartiles of HOMA-IR (p < 0.05).
Characteristics of study sample, National Health and Nutrition Examination Survey 1999–2004.
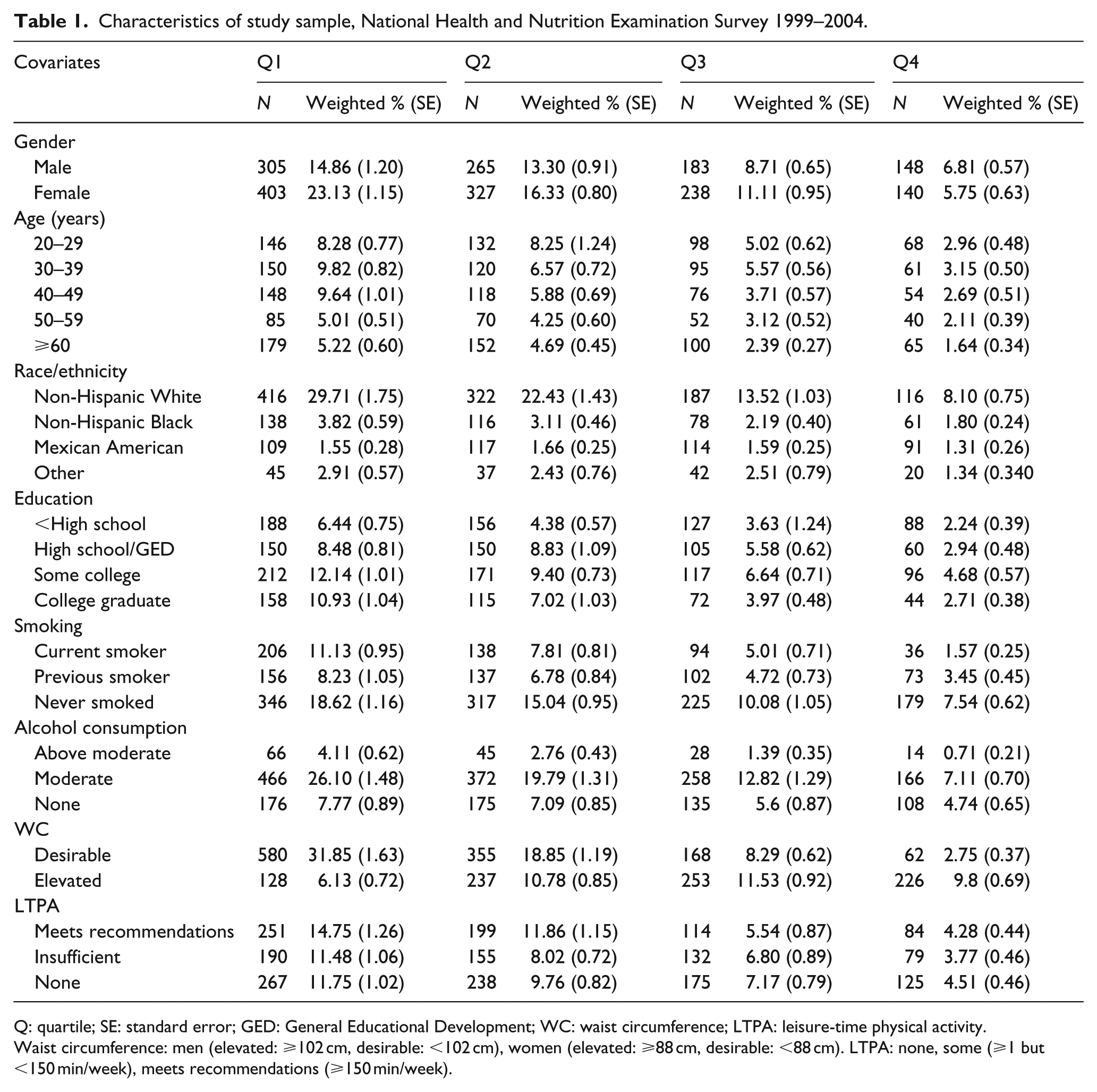
Q: quartile; SE: standard error; GED: General Educational Development; WC: waist circumference; LTPA: leisure-time physical activity.
Waist circumference: men (elevated: ⩾102 cm, desirable: <102 cm), women (elevated: ⩾88 cm, desirable: <88 cm). LTPA: none, some (⩾1 but <150 min/week), meets recommendations (⩾150 min/week).
Prevalence estimates for subjects reporting no MSA: 1999–2004 NHANES.
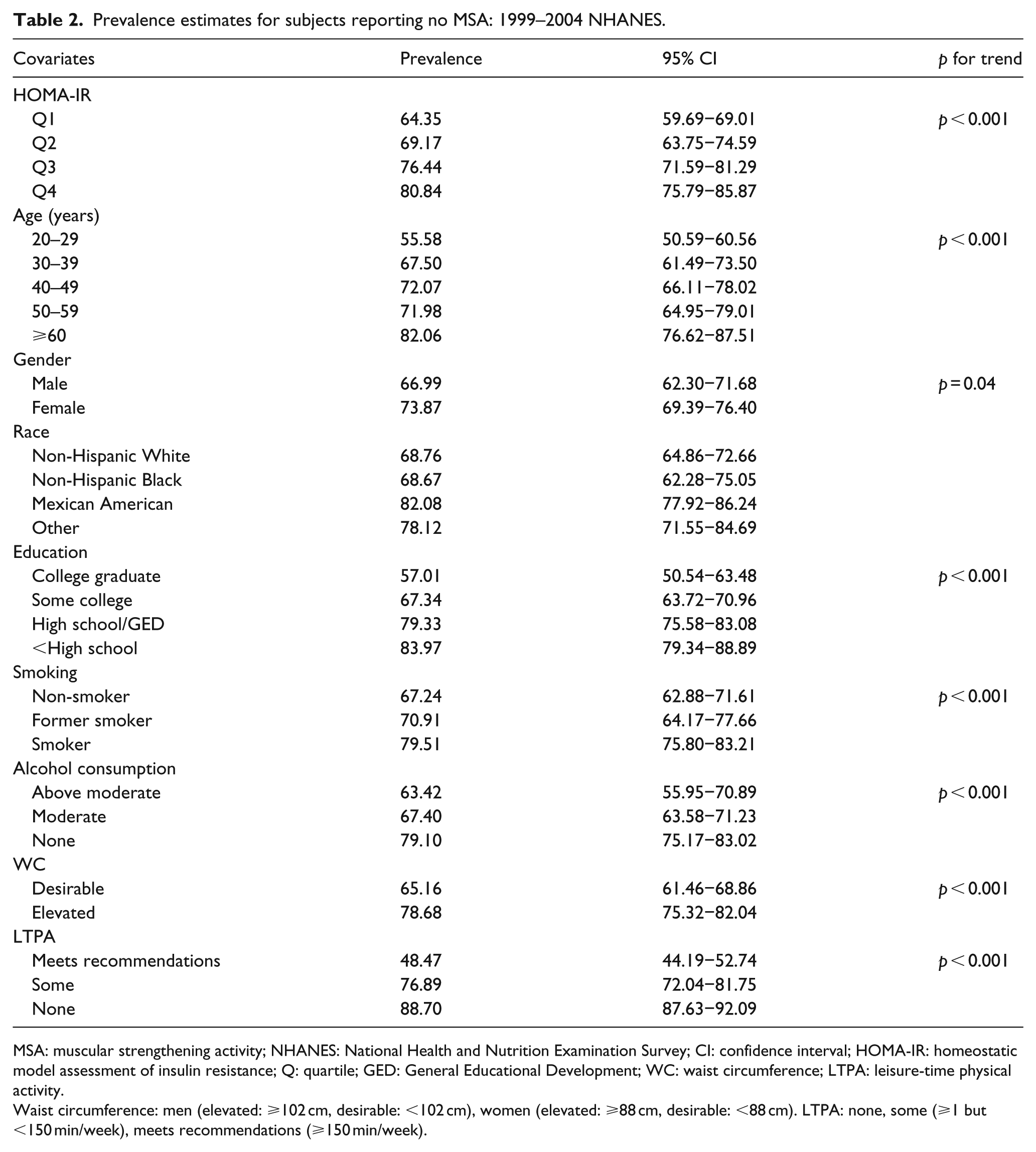
MSA: muscular strengthening activity; NHANES: National Health and Nutrition Examination Survey; CI: confidence interval; HOMA-IR: homeostatic model assessment of insulin resistance; Q: quartile; GED: General Educational Development; WC: waist circumference; LTPA: leisure-time physical activity.
Waist circumference: men (elevated: ⩾102 cm, desirable: <102 cm), women (elevated: ⩾88 cm, desirable: <88 cm). LTPA: none, some (⩾1 but <150 min/week), meets recommendations (⩾150 min/week).
Table 3 illustrates the results of the logistic regression analysis of the associations between quartiles of HOMA-IR and no self-reported MSA in euglycaemic adults. The unadjusted odds of reporting no self-reported MSA were significantly greater in subjects in the third (odds ratio (OR): 1.74, 95% CI: 1.37−2.22) and fourth (OR: 2.63, 95% CI: 1.93−3.57) quartiles of HOMA-IR compared to those in the first. Following adjustment for age, gender, race, education, smoking status, alcohol consumption and WC, results remained significant for only the fourth (OR: 2.04, 95% CI: 1.35−3.06) quartile. In the fully adjusted model, which included other non-MSA specific aerobic LTPA, the OR for reporting no MSA in the fourth quartile remained significant (OR: 2.30, 95% CI: 1.50−3.52).
Odds ratios for reporting no MSA in those without diabetes in the 1999–2004 NHANES.
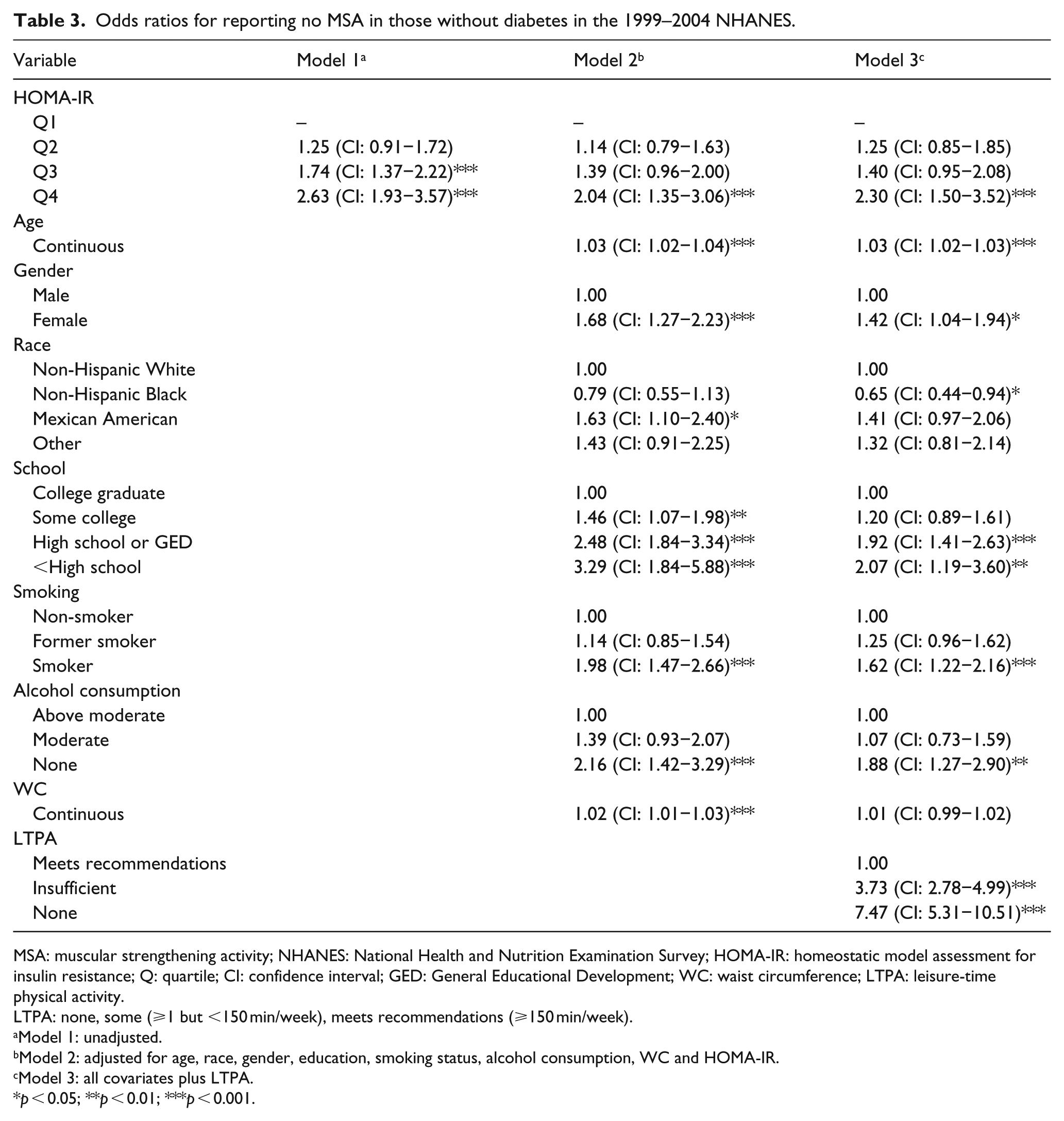
MSA: muscular strengthening activity; NHANES: National Health and Nutrition Examination Survey; HOMA-IR: homeostatic model assessment for insulin resistance; Q: quartile; CI: confidence interval; GED: General Educational Development; WC: waist circumference; LTPA: leisure-time physical activity.
LTPA: none, some (⩾1 but <150 min/week), meets recommendations (⩾150 min/week).
Model 1: unadjusted.
Model 2: adjusted for age, race, gender, education, smoking status, alcohol consumption, WC and HOMA-IR.
Model 3: all covariates plus LTPA.
p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
There is a paucity of data investigating PA and/or MSA behaviour among high-risk subjects without disease. Only a handful of studies have investigated associations between PA patterns and adverse metabolic conditions in subjects with and without cardiovascular and/or metabolic disease.16–22 To the best of our knowledge, the results of this analysis are the first to show significant increases in the prevalence of reporting no MSAs across increasing levels of HOMA-IR in euglycaemic US adults. Our results also revealed significantly greater odds of reporting no MSA in subjects in the third and fourth quartiles of HOMA-IR, independent of several covariates including aerobic LTPA.
Previous research supports an inverse relationship between MSA and IR in subjects with normal glycaemic levels8–15 utilizing a traditional approach. Miller et al. 8 reported significant reductions in basal insulin levels (37.5%, p < 0.05) and insulin levels in response to an OGTT (18.0%, p < 0.05) following a 10-week resistance training intervention. Another study conducted by Craig et al. 11 revealed significant decreases in insulin response (p < 0.05) to an OGTT independent of age (31.8% younger, 32.6% elderly) in healthy subjects completing a 12-week resistance training programme.
Two cross-sectional studies have also shown an association between IR and MSA.12,29 Churilla et al. 29 reported a significantly lowered odds (OR: 0.71, 95% CI: 0.54−0.93) for having impaired fasting glucose, potentially suggesting normal β-cell function and better metabolic health in subjects who report meeting the DHHS MSA recommendation compared to subjects reporting no MSA. In another analysis using 1999–2004 NHANES, Cheng et al. 12 investigated the associations between MSA and insulin sensitivity (measured via QUICKI 30 ) in euglycaemic subjects. Results revealed a significant difference in QUICKI levels for men and women reporting ⩾1 day/week of MSA (p < 0.05) compared to those reporting none. Following adjustment for covariates, results remained significant in females but not in males. Significance was only seen in volumes of MSA ⩾3 days/week (p < 0.05) in males. The results of these studies further indicate that MSA may be favourably associated with insulin sensitivity and glucose control.
The aforementioned studies have all shown inverse associations between MSA and IR in subjects without diabetes using MSA as the independent variable. However, our study investigated the associations between increasing HOMA-IR quartiles and no self-reported MSA utilizing HOMA-IR as the independent variable. This approach allows for the potential clinical examination and interpretation of surveillance data. Few studies have examined population-based data utilizing this method.16–22 Churilla et al. 20 reported the prevalence of meeting the 2008 DHHS PA recommendations to be 59.1% among participants with high cholesterol (HC) and 68.3% among participants with normal HC (p < 0.05), suggesting that individuals with elevated cholesterol levels may not be as physically active as individuals with desirable levels. Similar studies have investigated diabetes and PA patterns16,17 as well as diabetes and MSA patterns. 21 A recent study conducted by Mu et al. 21 reported that 12.4% of subjects with diabetes met the 2004 American Diabetes Association MSA recommendations. These data suggest that subjects with diabetes, HC, coronary heart disease (CHD) and hypertension may be less likely to engage in a volume of PA or volume of MSA (specific to those with diabetes) that may prevent chronic diseases and promote health. Furthermore, the use of this unique approach in surveillance research may allow clinicians (e.g. physicians, physician assistants, nurse practitioners) to better utilize their time with patients who need lifestyle counselling and coaching. Our study suggests that healthy subjects with high levels of IR (specifically the upper 75th percentile) have greater odds not performing muscular strengthening activities. Results from the few analyses and the current analysis may begin to provide clinicians an understanding of behavioural patterns in population data, thus revealing an increased need for recommendations in therapeutic lifestyle interventions (PA, MSA and dietary changes) within high-risk or diseased populations.
The current prevalence estimates for engaging in adequate amounts of MSA are approximately 21.9%–31.7%.31–34 Loustalot et al. 32 reported that 31.7% of respondents reported participation in MSA ⩾2 days/week. The most recent estimate, using the 2011 Behavioural Risk Factor Surveillance System (BRFSS), is approximately 29.3%. 34 From these data it can be estimated that approximately 70% of US adults are not engaging in adequate amounts of MSA. Our study adds to this knowledge within the context of chronic disease(s), specifically IR at the population level. Our findings specifically suggest that euglycaemic subjects in the upper quartile (80.83%, 95% CI: 76.79−85.87) and third quartile (76.44%, 95% CI: 71.59−81.29) of IR have a significantly greater prevalence of reporting no MSA compared to subjects in the lowest quartile (64.35%, 95% CI: 59.69−69.01). This suggests that more people, both apparently healthy and those with chronic conditions, need to be educated on the current MSA recommendations.
According to Barnes and Schoenborn 35 the prevalence of physicians recommending exercise or PA to adult patients is approximately 32.4%. Moreover, this study illustrated that subjects with disease (e.g. diabetes, obesity, CVD, cancer and hypertension) had a greater prevalence of physician recommended exercise volumes compared to those without disease or those with a desirable body mass index (BMI). Despite increased prevalence of physician recommendations, Zhao et al. 17 showed that subjects with diabetes have lower odds of reporting participation in adequate volumes of PA. Interestingly, subjects with IR, who may have normal glucose levels, are in a state of increased risk of disease development (i.e. CVD 4 and diabetes 1 ), and there are no data currently reporting the prevalence of physician recommended PA, specifically with IR status. Furthermore, our study results reveal the importance of continuing research into this area in order to combat the increasing incidence and prevalence of IR which have been shown to be highly associated with increased risk of CVD,3,4 diabetes1,36 and a number of adverse metabolic conditions including obesity,37,38 dyslipidaemia,39,40 inflammation 41 and hypertension. 42
A previous review 43 investigating the role of MSA and the risk of CVD revealed that MSA can improve insulin action, glucose response, reduce body fat and reduce visceral adipose tissue, all of which are risk factors of CVD at abnormal levels. A recent study by Grøntved et al., 44 investigating the effects of MSA on type 2 diabetes, revealed that men who participate in aerobic training (AT) and MSA for at least 150 min per week have a 59% reduction in risk for diabetes. Furthermore, a study investigating MSA and risk of CHD by Tanasescu et al. 45 reported a 23% (relative risk: 0.77, p < 0.05) reduction in risk for CHD in men who participated in at least 30 min of MSA per week compared with men who did no MSA. These results suggest that participation in routine PA, inclusive of MSA, could have a favourable impact on the risk of diabetes and other chronic disease including CVD. 46 Due to the relationship between CVD and diabetes, as shown in a review by Grundy et al., 46 it is imperative for health care professionals to recommend PA, inclusive of MSA, to everyone capable of safely participating. Furthermore, due to the preventive effects MSA can have on diabetes and CVD risk, it is vital that adults in higher risk categories (i.e. higher levels of IR despite normal glucose levels) be counselled on therapeutic lifestyle changes, including engaging in MSA.
The strengths of our study include strong external validity owing to the use of a large representative sample and the use of validated assays to measure insulin and glucose. Moreover, the unique approach to this study design provides clinicians insight into the MSA patterns of euglycaemic subjects with across increasing degrees of IR. The limitations of our study include the cross-sectional study design, which does not allow for causation to be established, and residual confounding including PA participation the day before testing. Also, the use of questionnaires for the assessment of MSA may be subject to recall bias.
Conclusion
Euglycaemic adults who fall in the upper 75th percentile of HOMA-IR were more likely to report no MSA independent of several covariates. MSA has been shown to improve insulin action, glycaemic control and reduce the risk of CVD and type 2 diabetes. Thus, it may become increasingly important for health care professionals to advocate MSA participation in all populations that can safely participate, specifically those with greater levels of IR.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.