
Abstract
Introduction:
Almost all studies on diabetic foot syndrome focused on prevention of amputation and did not investigate long-term prognosis and survival of patients as a primary outcome parameter.
Methods:
We did a retrospective cohort study including 314 patients who had diabetic foot syndrome and underwent amputation between December 1995 and January 2001.
Results:
A total of 48% of patients received minor amputation (group I), 15% only major amputation (group II) and 36% initially underwent a minor amputation that was followed by a major amputation (group III). Statistically significant differences were observed in comparison of the median survival of group I to group II (51 vs 40 months; p = 0.016) and of group II to group III (40 vs 55 months; p = 0.003).
Discussion:
The prognosis of patients with major amputation due to diabetic foot syndrome is comparable to patients with malignant diseases. Vascular interventions did not improve the individual prognosis of patients.
Introduction
Diabetic foot syndrome (DFS) is one of the most important but simultaneously one of the most neglected long-term complications in diabetes mellitus. Depending on patient age and type of diabetes, the prevalence of DFS ranges between 1.7% and 10%. 1
Generally, the principles in treatment of DFS are well established. Close monitoring of blood-glucose levels, resection of necrotic tissue, special attention to the feet, infection control with antibiotics and careful and specialized wound management are essential for every patient. A lot of patients need vascular surgery or interventions for adequate perfusion of the lower extremities at some point. Although all these points are known for several decades, long-term prognosis of patients with chronic diabetic foot infection is still poor.1–3
Pressure ulcers resulting from inadequate shoes, diabetic polyneuropathy and vascular disease together with systemic manifestation of hypertension and obesity often end up in an adverse outcome of patients with DFS together with minor and major amputations. 4 Amputations should only be considered after a multidisciplinary discussion of the individual patient and after utilizing all non-operative options mentioned before.
Long-term prognosis of patients with a DFS and amputation is bad and bears an attributed 3-year mortality of 35%–50%. 5 Amputations are associated with a severe reduction of survival and the quality of life. Furthermore, socioeconomic costs are vast resulting from chronic syndrome and demographic changes.4,6,7
Studies from different European countries were able to show a statistically significant decrease in the incidence of diabetes-associated amputations over the last decade.8–11 It was observed that this was the result of a significant reduction in major amputation rates with a growing incidence of minor amputations. 12 Most available studies focused on the prevention of amputation and did not investigate the long-term prognosis and survival of patients. In this study, we focused on the two latter parameters. As secondary outcome parameters, we analysed several risk factors and concomitant diseases for their impact on patient survival.
Methods
The data of all patients of the Department of Surgery of the University Clinic of Schleswig-Holstein, Campus Luebeck, with a minor or major amputation associated with DFS were included in an electronic data base after prior informed consent. The study was approved by the local ethics committee. Data were recorded between December 1996 and January 2004. Data and follow-up data were included beginning with the first amputation. We predefined patient groups with minor amputation (amputation below the ankle joint) and major amputation (amputation above the ankle joint). As a result of these specifications, three groups of patients were analysed (Table 1). A retrospective evaluation of the data was performed.
Patient groups.

Arterial hypertension was defined as systolic blood pressure >130 mmHg or diastolic blood pressure >80 mmHg. Cardio-vascular disease was defined as prior myocardial infarction or ischaemic stroke or acute coronary syndrome. Diabetic nephropathy was defined as serum creatinine level above 104 μmol/L. Vascular interventions were also included in the data evaluation: vascular surgery and percutaneous techniques with and without vascular stents. The perfusion, extent/size, depth/tissue loss, infection, sensation (PEDIS) classification (Table 2) was used for DFS classification to enable a more precise comparison in patients.
Infectious Diseases Society of America (IDSA) and International Working Group on the Diabetic Foot classifications of diabetic foot infection. 1
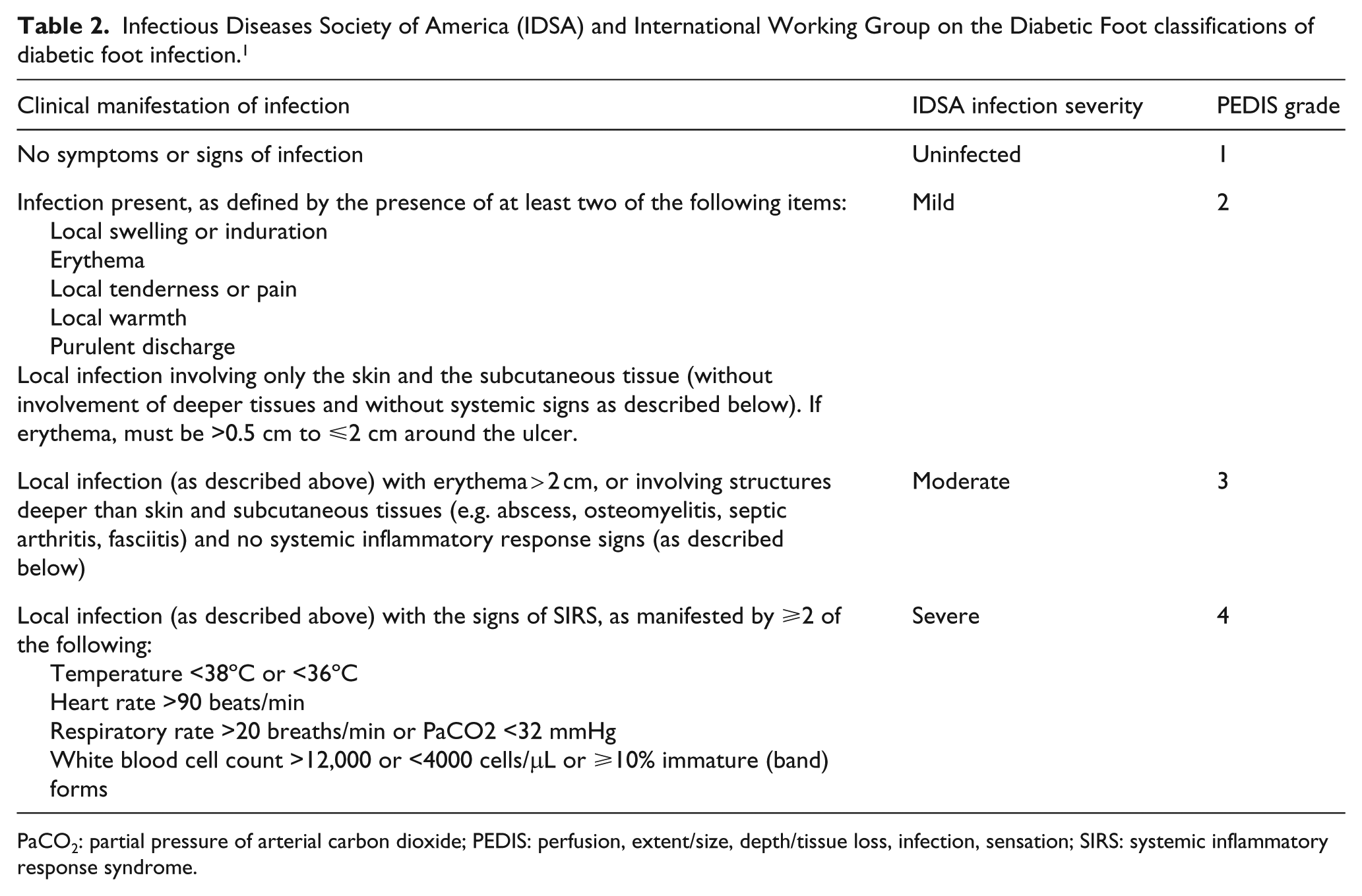
PaCO2: partial pressure of arterial carbon dioxide; PEDIS: perfusion, extent/size, depth/tissue loss, infection, sensation; SIRS: systemic inflammatory response syndrome.
Mortality and patient survival were calculated with reference to the first amputation. The follow-up period was between 3 months and 15 years. The last follow-up for mortality data from the central mortality registry of Schleswig-Holstein was in December 2010.
Overall survival of the patients in the three prespecified groups was defined as the primary outcome parameter. Additionally, we did subgroup analyses of the patients’ risk factors for an adverse outcome (renal insufficiency, cardio-vascular disease, hypertension, insulin-dependent diabetes mellitus, gender, age); 30 days in-hospital mortality was not included in the statistical analysis of patient survival (9 patients).
Statistical analysis was done with SPSS Version 17.0 (SPSS Inc., Chicago, IL). We used the Kaplan–Meier method for survival estimates together with the log-rank test. Comparison of median values was done with student’s t-test; the χ2 test for frequencies was used for frequency associations in the different groups. A p-value <0.05 was considered to be statistically significant.
Results
A total of 314 patients were included in the statistical analysis. Group I had the largest number of patients with a total of 152; groups II and III had 48 and 114 patients, respectively (Table 2).
The PEDIS classification was used to categorize the patients after amputation. Table 3 shows the distribution of the different PEDIS stages in the three groups. The median interval between minor and major amputation in group III was 361 ± 782.17 (3–4279) days.
PEDIS stages in the different groups at first amputation.
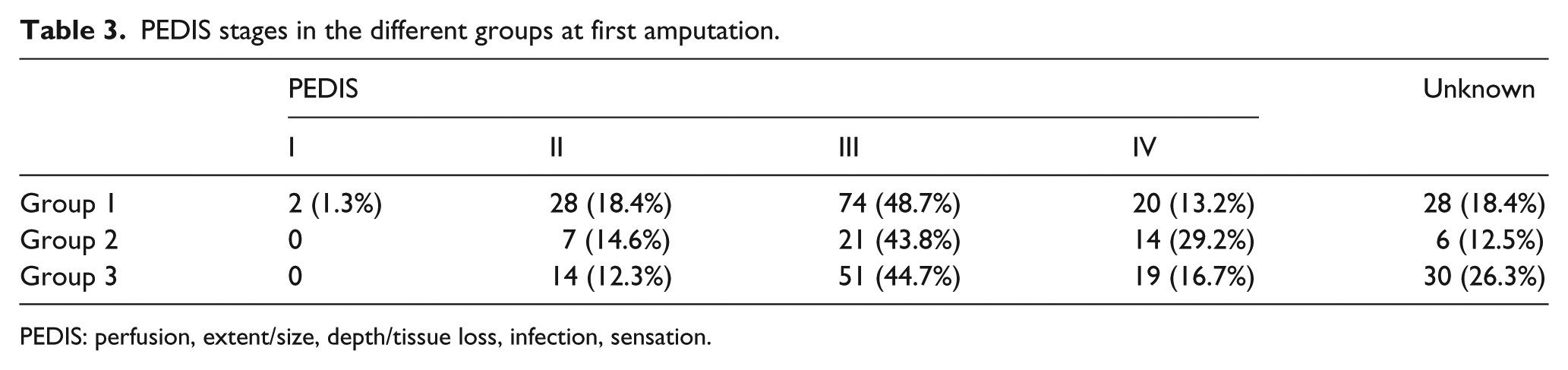
PEDIS: perfusion, extent/size, depth/tissue loss, infection, sensation.
Demographic data
A total of 204 men underwent amputation at a median age of 64.5 ± 11.2 (33–96) years, while 110 women with a median age of 74.0 ± 10.8 (43–95) years were amputated. This difference in median age was statistically significant between male and female gender (p < 0.0001).
A further differentiation of patients according to the three predefined groups was able to show further statistically significant differences concerning age between groups I (67.00 ± 12.04 (33–96) years) and II (74.00 ± 11.42 (45–95) years) and between groups II and III (64.50 ± 11.49 (36–92) years) (p = 0.002).
Table 4 shows the distribution of male and female gender in the three groups. There were statistically significant more male patients in groups I and III.
Male/female ratio in the three groups.
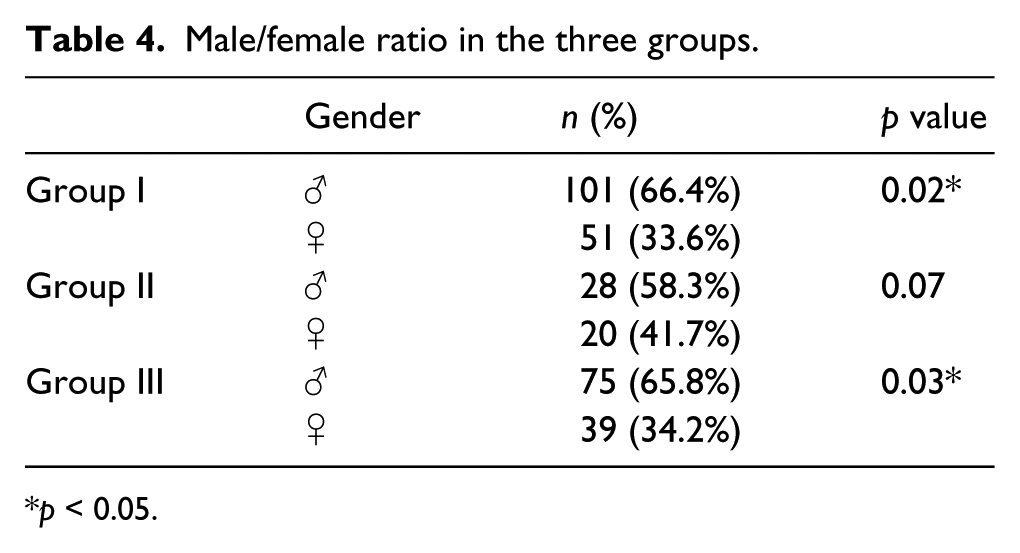
p < 0.05.
Hospitalization
The median number of hospitalization was 1.80 ± 1.103 (1–7). The overall number of hospitalization days was 68 days (median). Table 5 shows the number of patient hospitalization days in the three groups.
Hospitalization data for the three patient groups.

Statistically significant differences with regard to the length of overall hospitalization were found between groups I and II and groups II and III (p < 0.0001).
Comorbidity
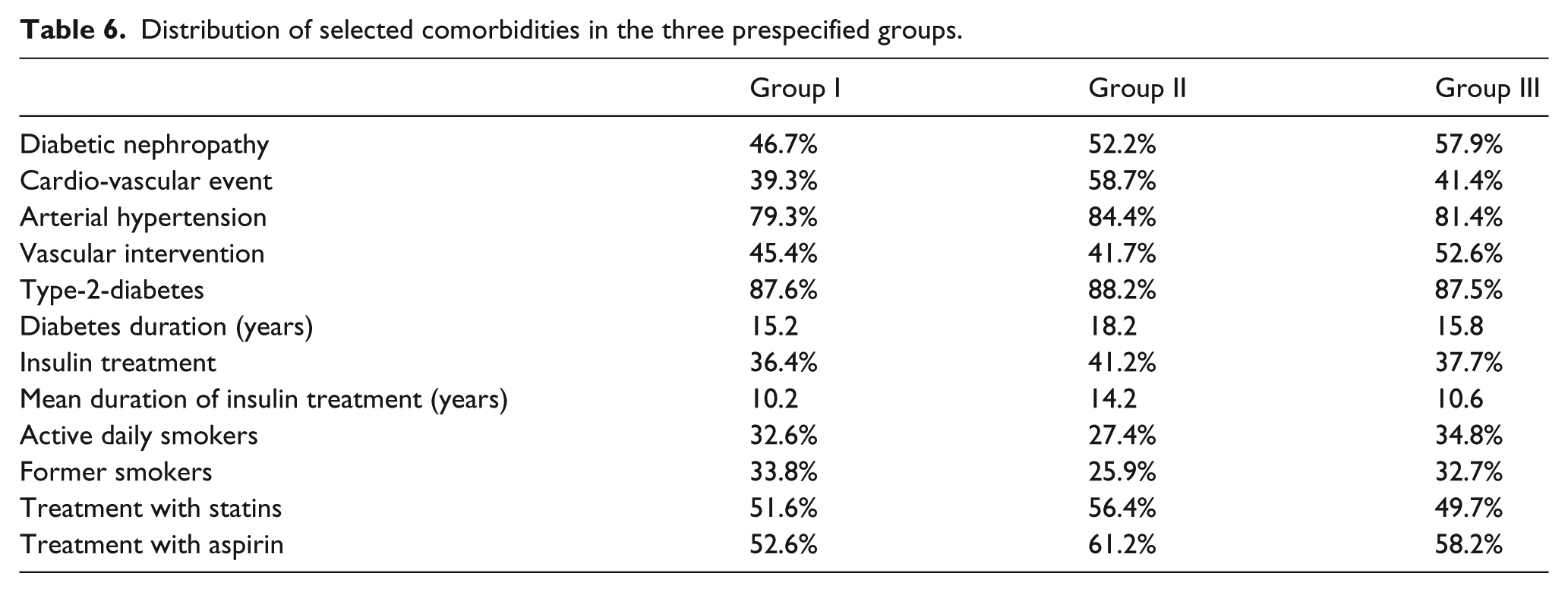
In Table 6, the prevalence of selected comorbidities in the three patient groups is shown. The long-term survival of patients with diabetic nephropathy or prior cardio-vascular events was significantly worse than that of patients without these pre-existing syndromes (p < 0.0001 and p = 0.002; Table 7). The risk factors arterial hypertension and insulin-dependent diabetes mellitus did not have a statistically significant impact on the survival of patients.
Distribution of selected comorbidities in the three prespecified groups.
Survival with reference to comorbidities.

Survival
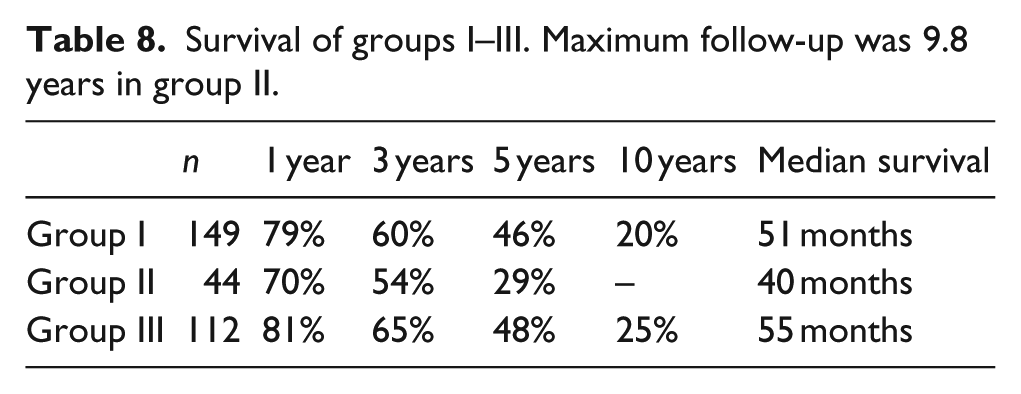
Nine patients died within 30 days following the index amputation and were excluded from the statistical analysis. The remaining 305 patients had 1-, 3-, 5- and 10-year survival rates of 78%, 61%, 44% and 19%, respectively. The median survival was 50 months. The survival rates in the 1-, 3-, 5- and 10-year follow-up of the three predefined groups is presented in Table 8 and Figure 1.
Survival of groups I–III. Maximum follow-up was 9.8 years in group II.
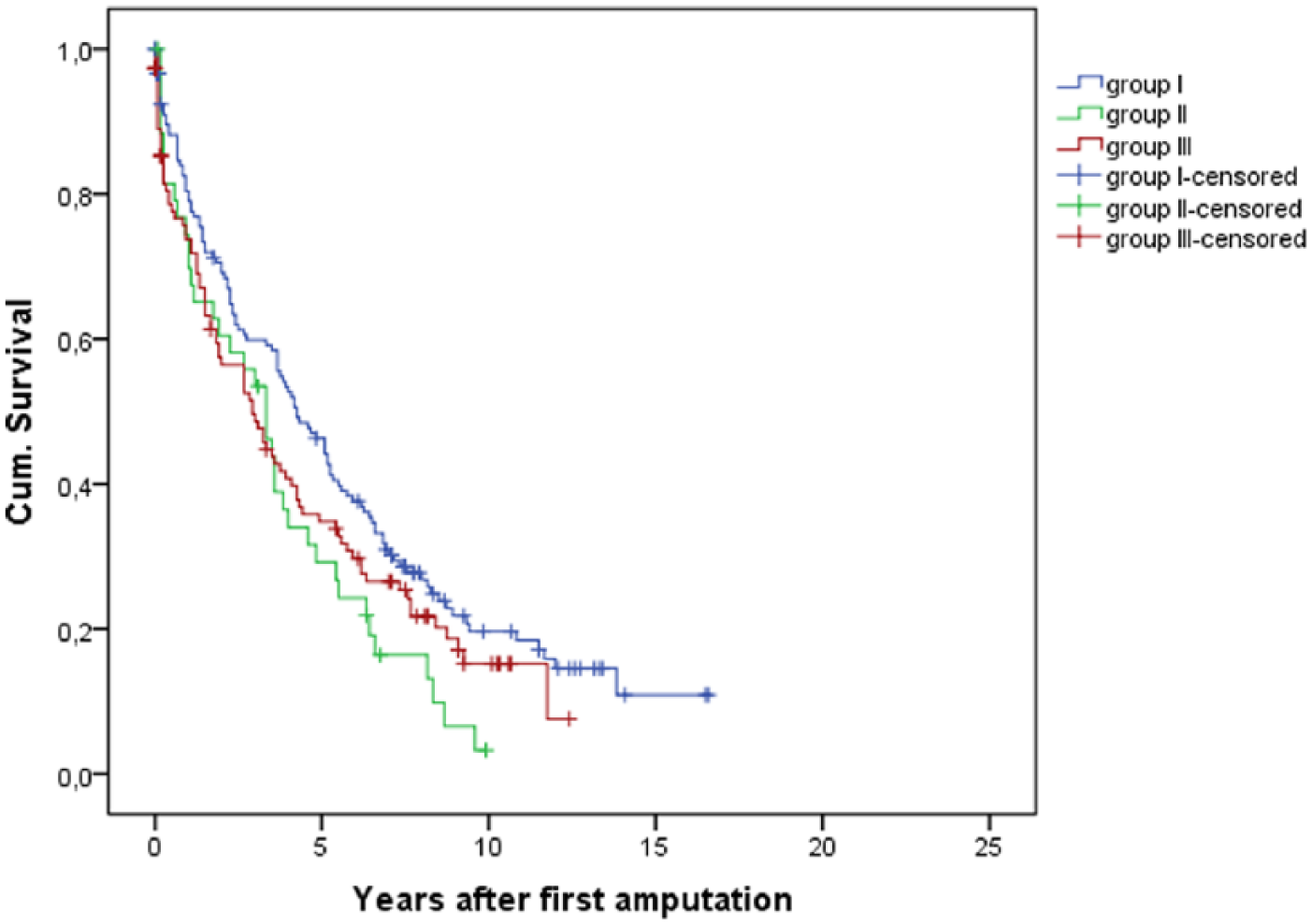
Median survival of groups I–III (Kaplan–Meier).
We were not able to show statistically significant differences in survival between patient groups I and III in the log-rank test. Statistically significant differences with reference to survival were observed between groups I and II (p = 0.016) and groups II and III (p = 0.003). In a comparison of groups II and III with the major amputation as the index amputation, the survival advantage was no more verifiable. Patient survival was absolutely identical in this analysis.
Vascular interventions/surgery
A total of 149 patients had vascular interventions prior to first amputation. In all, 45 patients received stent implantation, 62 patients underwent bypass surgery and 41 patients received stent placement followed by vascular surgery. There were no statistically significant differences between the three groups with regard to the prevalence of vascular interventions.
Patients who underwent a vascular intervention before the first amputation did not feature better survival compared to patients without vascular intervention.
Gender/comorbidity
We observed a highly statistical significant difference with reference to survival between male and female gender after first amputation (p = 0.002). This difference was no more detectable after adjustment for age; the age-associated mortality was not statistically significant between male and female gender.
Type of ulcer
We subclassified the ulcers as neuropathic, ischaemic or mixed ulcers. We were not able to observe any statistically significant differences with reference to survival between the different types of ulcers. The prevalence of any type of ulcers was not different in the three groups.
Surgery/results of surgery
We collected data concerning type of surgery and the extent of amputation (below or above the ankle, below or above the knee). Additionally, we collected data on the postoperative morbidity of patients and especially impaired wound healing. There were no statistically significant differences between groups II and III with regard to the extent of amputations. We observed a statistically significant difference with regard to the incidence of impaired wound healing in the comparison of groups I and II (p = 0.012) and groups II and III (p < 0.01). No statistically significant difference was observed in comparison of groups I and III.
Discussion
DFS is associated with a high 5-year mortality.13–15 Only few studies were designed to investigate the individual prognosis after minor or major leg amputation. This study may be criticized because of the inexistence of a control group of patients with diabetes without amputation. From the authors’ point of view, this comparison is not justified because the primary outcome parameter of the study was mortality after any amputation. A comparison with a group that did not have an amputation would thus make no sense.
During the review process of the present literature, we were only able to identify a few studies that focused on patient survival. One study was performed by Larsson in 1998. They showed 1-, 3- and 5-year mortality rates of 15%, 38% and 68%, respectively, in patients with DFS. 5 Another study by Tentolouris et al. 16 described a 5-year mortality rate of 44% after first major amputation.
We found 1-, 3-, 5- and 10-year survival rates of 78%, 61%, 44% and 19%, respectively, in our study. Our results are in accordance with the studies mentioned above and the results of a recent single centre study of a large diabetes centre that did a follow-up of patients without major amputation at the time of study inclusion for 12–13 years. The study described 1-, 3-, 5- and 10-year survival rates of 83%, 65%, 52% and 28%, respectively. 17
The extent of amputation bore the highest impact on prognosis of the individual patient. We observed a highly statistical significant difference in patients with minor and major amputation. A major amputation was associated with an adverse outcome and reduced long-term survival.18,19 These results are further supported by the studies of Larsson et al. 12 and Faglia et al. 20
We observed a highly significant difference in the comparison of long-term survival between groups II and III. The median survival rate in group III was 15 months longer than in group II. This difference was only detectable if the minor amputation was defined as the index operation. After any major amputation, long-term survival was absolutely comparable in both groups II and III. The difference in overall survival between groups I, II and III was associated with a significant difference in hospitalization days.
The patients in groups I and III showed a survival advantage, but the percentage of days spent in hospital of the 15 months that they lived longer compared with group II was very high. Additionally, they showed a significantly higher incidence of impaired wound healing. This resulted on the one hand in prolonged hospitalization and on the other hand in reduced mobilization and the need for support by nursing home facilities and ambulatory wound care teams. We do not have sufficient data on the quality of life of these patients. It is subject to speculation if the survival advantage resulted in a drop of quality of life.
Groups I and III were not different in regard to long-term survival. DFS is one of several clinical presentations of a complex generalized disease. The management of local wound infections and minor or major amputations are features in treating this complex generalized disease. The leading cause for mortality in patients with diabetes mellitus is cardio-vascular events.20,21 Patients who needed major amputations suffered from a more severe cardio-vascular disease than others. Therefore, the attributed mortality of major amputations is higher because of a more complex generalized disease.
The results of our subgroup analysis of potential risk factors were heterogeneous. Female gender was a risk factor for reduced survival in our study. Peek and coworkers also identified female gender as a risk factor in their study, while another group was not able to detect any statistically significant difference between genders.22,23 As in our study, these effects were alleviated if gender was analysed alongside the age at first amputation. Female patients were significantly older at first amputation (74 years) compared to male patients (64 years). Age adjusted analyses were not able to detect any statistically significant differences between male and female gender. The higher attributed mortality is thus a result of the significantly higher median age of the overall female cohort.
Previous studies identified diabetic nephropathy as a risk factor for a significantly lower long-term survival.15,17,24 These results are supported by the results of our study. As pointed out before, cardio-vascular disease and cardio-vascular events are of high prognostic relevance for patients with diabetes mellitus. 25 Patients with a preceding cardio-vascular event (myocardial infarction, ischaemic stroke) had a significantly worse outcome compared to patients without any cardio-vascular events.
The prevalence of insulin dependency was not of prognostic relevance for mortality. These results of our study are supported by previous trials of Aulivola et al. 24 and Takahara et al.24,26
One of the mainstays of the therapy of DFS is surgical or interventional revascularization. A study group of Moulik et al. was investigating the prognosis of patients with DFS. As a secondary study objective, they focused on different types of diabetic foot ulcers. Mortality and morbidity were high in all three types of diabetic foot ulcers (neuropathic ulcers, neuropathic–ischaemic ulcers, ischaemic ulcers). Ischaemic ulcers showed the highest rate in 5-year mortality and bore a significantly higher rate than the one in neuropathic ulcers. 13 This difference only reached statistical significance in a univariate analysis, while it was no more observed in multivariate analysis. The type of ulcer is therefore not an established risk factor for mortality. Likewise, our study was also not able to show a statistically significant difference between the different types of diabetic ulcers.
A strong argument for revascularization in DFS is the severe impairment of the quality of life as a result of any amputation, especially of any major amputation.
Multidisciplinary patient care led to a revascularization in more than 90% of all patients with DFS. A study by the Vascular Surgical Society of Great Britain and Ireland was able to show that an amputation was prevented in 80% of all patients who underwent revascularization. 27 Hence, the quality of life was much better in these patients.
The results of this study are not supportive for a survival advantage in patients who underwent any revascularization therapy before amputation. On the contrary, an Italian study was able to demonstrate a statistically significant survival advantage in patients who underwent revascularization therapy before amputation. 28 These results are not contradictory to those generated by this study because as mentioned before, the long-term prognosis of the patients is determined by the generalized cardio-vascular syndrome and not by the results of interventions on the lower extremities. Our study clearly shows that a major amputation is associated with a high mortality and that this outcome is independent from any intervention before. Vascular surgery or interventions hence are only prolonging life without major amputation. The results of the interventions may have implications on the quality of life of the patients, but this was not part of this study protocol.
We were able to show that major amputation is the main predictor of mortality in a large non-selected patient group of a university hospital. Mortality is comparable to patients with systemic malignant disease with median survival rates of 40–55 months after the first amputation.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.