
Abstract
Objective
We aimed to assess the prevalences of foot ulcer and foot self-care practices, and identify associated factors in adult patients with diabetes attending a referral hospital in south-east Ethiopia.
Methods
We performed a cross-sectional study of 267 diabetic patients. Multivariable binary logistic regression was used to identify factors associated with diabetic foot ulcer and foot self-care practice.
Results
The prevalence of diabetic foot ulcer was 11.2% (95% confidence interval [CI] 7.42–15.05). One hundred and forty-four (53.9%; 47.9, 59.9) patients demonstrated good foot self-care. Living rurally (adjusted odds ratio 2.27; 95% CI: 1.86–6.97), lack of regular exercise (3.91; 1.51–10.10), peripheral neuropathy (2.77; 1.05–7.33) and foot calluses (5.69; 1.74–18.59) were associated with diabetic foot ulcer. Urban inhabitants (2.01; 1.09–3.69), patients with diabetes for >10 years (2.92; 1.48–5.77), women (2.95; 1.66–5.22), and patients with a glucometer at home (2.05; 1.09–3.85) were more likely to have good foot self-care practice.
Conclusion
The prevalence of diabetic foot ulcer was 11.2%. This prevalence is lower than those identified in other Ethiopian studies. However, patient awareness regarding foot self-care practice and risk reduction should be improved.
Keywords
Introduction
Diabetes mellitus (DM) is a metabolic disorder characterised by high blood glucose concentration, resulting from defective insulin secretion or action, or both. 1 In 2017, the International Diabetes Federation (IDF) estimated that there were 451 million people aged between 18 and 99 years of age worldwide who had diabetes, and this number was predicted to increase to 693 million by 2045. 2 In 2019, the annual worldwide diabetes-related health expenditure was estimated to be USD 760 billion for adults aged between 20 and 79 years of age, and this was predicted to grow to USD 825 billion by 2030 and USD 845 billion by 2045. 3
Sub-Saharan Africa is also currently experiencing a heavy burden of diabetes. The Sub-Saharan region of Africa has an estimated 14.2 million people with diabetes, 4 and in Ethiopia, 1.6 million deaths were estimated to have been directly caused by diabetes in 2016. 5
With the increasing number of patients with diabetes, a higher incidence of diabetic complications is inevitable. Diabetic foot ulcer (DFU) is one of the most serious and common complications of DM,6,7 and can affect all aspects of an individual’s life. 8 A systematic review and meta-analysis conducted in Ethiopia showed that the prevalence of DFU was 12.98% 9 , and worldwide, 9.1 to 26.1 million patients with diabetes develop DFU annually. The lifetime incidence of DFU has been estimated to be 19% to 34%. 10 The prevalence of DFU has been estimated to be 6.3% worldwide and 7.2% in Africa; 11 and in Ethiopia, the estimate has varied from 11.6% to 31.1%.12,13
DFUs are a significant cause of lower extremity amputation in patients with diabetes. More than a million people lose a leg every year as a consequence of this disease worldwide. 14 Indeed, every 30 second, a lower limb or part of a lower limb is amputated somewhere in the world because of diabetes. 15 A study conducted in Turkey revealed that 41.4% of patients with DFU underwent amputation. 16 Hence, DFU has a significant impact on the quality of life of patients, often involving long-term hospitalisation, and imposes a heavy economic burden. 17
In Sub-Saharan Africa, the DFU burden is high because of late diagnosis, poor patient awareness, poor foot self-care practice, and poor access to diabetes care.18,19 Therefore, prevention is critical, including through the education of patients with diabetes regarding preventative strategies, including appropriate foot self-care, which has been poor in many countries, including Ethiopia.19–23 The risk of DFU is higher in rural locations, in patients with calluses on their feet, in obesity, if self-care is poor, in patients with type 2 diabetes mellitus, in patients with long-standing diabetes, in those of advanced age, when the haemoglobin A1C (HbA1c) is high, in the presence of dyslipidaemia, and in the presence of comorbidities.8,11,24 The probability of patients performing appropriate diabetic foot self-care has been shown to be affected by sex, educational status, geographical location and the duration of diabetes.19,22,25
Although it is possible to reduce the risk and prevent the adverse outcomes of diabetes by normalising blood glucose concentrations, diabetic complications, including DFU, continue to affect the physical, psychosocial, financial and overall quality of life of many patients with diabetes. 26 There have been a number of studies of DFU in Ethiopia, and substantial variations in the prevalences of DFU and appropriate foot self-care have been identified across the regions. This may be the result of the differing socio-demographic characteristics of patients, their lifestyle, and/or their access to ongoing treatment.27–29 Most of the studies to date have been performed in the north,19,24,29–31 west12,32 and east of the country, 27 and none have been performed in the south-east region. Therefore, in the present study, we aimed to estimate the prevalences of DFU and appropriate foot self-care practice, and to identify the factors associated, in adult patients with diabetes in south-east Ethiopia. The findings of the study could encourage the development of strategies aimed at preventing and reducing the risk of DFUs.
Methods and materials
Study area and duration
The study was conducted at Madda Walabu University Goba Referral Hospital, Bale Zone, south-east Ethiopia, between 1 June and 1 August 2021. Goba is found in Oromia Regional State, 444 km from Addis Ababa, the capital of Ethiopia. The hospital serves 115,442 inpatient and outpatients annually. Currently, the ambulatory clinic provides healthcare services for 1422 patients with diabetes.
Study design
We performed a cross-sectional study of patients with diabetes attending this single institution. We have followed the STROBE guidelines for the reporting of this study. 33
Sample and eligibility criteria
All the adult patients (≥18 years old) with diabetes mellitus who attended the ambulatory clinic at Goba Referral Hospital during the study period formed the study sample. Patients with traumatic ulcers resulting from road traffic accidents and those who were severely ill and unable to communicate were excluded.
Sample size determination
The sample size was determined using a single population proportion formula with the following assumptions: p = 11.6%, 12 d = 4% and Zα/2 = 1.96; and after the allowance of a 10% non-response rate, a required sample size of 271 was obtained. A systematic random sampling technique was used to select the study participants. The sampling interval was calculated by dividing the population size by the desired sample size. Hence, K = N/n = 1422/271 = ∼5. The first participant was randomly picked from numbers 1 to 5. Number four was randomly picked, and then every fifth participant was selected.
Data collection methods and measurements
Data regarding socio-demographic characteristics, foot self-care practice and behavioural factors were collected using a previously validated, pre-tested, structured questionnaire through face-to-face interviews. Physical measurements (height, body mass and blood pressure [BP]) and laboratory measurements (lipid profile and serum glucose concentration) were made, and a physical examination was performed for DFU. Clinical factors, such as the type of diabetes, were recorded at a patient interview, and medical records were used to identify documented comorbidities. Direct observation of the patients was performed to assess the condition of their feet and to perform Wagner classifications. A diabetic foot self-care practice questionnaire was completed. This was adapted from the validated Nottingham Assessment of Functional Foot care (NAFF).23,34 After preliminary testing, 10 items were selected out of the original 29 because they were the most appropriate to assess the behaviour of interest. The questionnaire was prepared in English, translated into the local language (Afan Oromo or Amharic) and retranslated into English to maintain consistency. Trained general practitioners and MSc-qualified nurses performed the data collection. Two days of training were provided for both the data collectors and supervisors.
Anthropometric, blood pressure and laboratory measurements
Height was measured using a stadiometer, with the participants standing erect against a wall, with their heels together, after removing their shoes, facing forward. Body mass was measured using a standardised digital scale (0 to 130 kg) while wearing minimal clothing and no footwear. Data collectors zeroed the scales before each measurement. Body mass index (BMI) was calculated by dividing body mass in kg by the square of height in metres. BMI <18.5 kg/m2 was interpreted as underweight, 18.5–24.9 kg/m2 as normal, 25.0–29.9 kg/m2 as overweight and ≥30.0 kg/m2 as obese. 24 Before measuring BP, the data collectors confirmed the respondents had not consumed any hot drinks, smoked or chewed tobacco, or undertaken vigorous physical activity during the 30 minutes preceding the interview. Three separate BP measurements were made using the left arm of each participant using a calibrated mercury sphygmomanometer, with the participants resting for at least 5 minutes in a seated position between each measurement. The mean value of the measurements was recorded as the BP of the participant. Hypertension was defined as a systolic BP ≥140, a diastolic BP ≥90 mmHg or a history of treatment with an anti-hypertensive agent.35,36
For laboratory measurements, 5 ml of fasting venous blood was collected from each participant into a serum separator tube. The blood samples were transported to the Madda Walabu University Goba Referral Hospital Clinical Chemistry Laboratory for analysis. The serum was separated within 2 hours of sample collection. A trained laboratory technician measured the lipid and glucose concentrations. Dyslipidaemia was defined as the presence of at least one of the following: high serum total cholesterol concentration (≥5.27 mmol/L), high triglyceride concentration (≥1.69 mmol/L), high low-density-lipoprotein (LDL)-cholesterol concentration (≥3.36 mmol/L), or low high-density lipoprotein (HDL)-cholesterol concentration (<1.03 mmol/L in men and <1.29 mmol/L in women). 37 Uncontrolled serum glucose was defined using a fasting serum glucose concentration of >6.99 mmol/L. 24
Outcome measurements
DFU and foot self-care practice were used as the dependent variables. DFU was graded according to Wagner’s classification: Grade 0, no ulcer, but the foot is at risk for ulceration; Grade 1, superficial ulceration; Grade 2, ulcer with deep infection, but without the involvement of the bone; Grade 3, ulcer with osteomyelitis; Grade 4, localised gangrene; and Grade 5, gangrene of the whole foot. 38 Diabetes foot self-care was defined as the care provided by the patient for their feet and general well-being. Ten items were used to assess foot self-care, which were graded using a three point Likert scale as “never”, “sometimes” or “always”, with responses recorded as 0 to 2, respectively. Good practice was defined using a score of greater than or equal to the mean and poor practice was defined using a score of less than the mean. 19
Independent variables
The independent variables used in the analysis were sociodemographic characteristics (age, sex, educational status and area of residence), behavioural factors (smoking habits, alcohol consumption and physical activity), and clinical factors (fasting serum glucose concentration, BMI, presence of comorbiditites, type of diabetes, lipid profile, peripheral neuropathy and duration of diabetes mellitus).
Data quality assurance
Analytical procedures were adapted from previously described studies to ensure data quality.19,24,28 Preliminary testing was performed on 5% of the total number of samples collected at Bale Robe General Hospital before the data collection period commenced. The data collectors were recruited from outside the study area, and the principal investigator trained the data collectors and supervisors. Trained supervisors provided regular supervision and spot-checks, and provided immediate feedback daily during the data collection. In addition, double data entries into Epi data version 4.6.0.2 (www.epidata.dk) were performed by two data clerks to ensure data accuracy.
Data analysis
The cleaned and coded data were entered into Epi Data Version 4.6.0.2 software and then exported into SPSS for Windows, version 25 (IBM, Inc., Armonk, NY, USA) for analysis. The frequencies, percentages, means and standard deviations of the data are used to describe the study sample. Bivariable logistic regression was performed to determine the crude relationships of each independent variable with DFU and diabetic foot self-care practice. Variables with p < 0.25 using a 95% confidence interval (CI) during binary logistic regression analysis were considered for inclusion in the multivariable binary logistic regression model, to control for potential confounders. Variables with p < 0.05 on multivariate analysis were considered to be statistically significant. Adjusted odds ratios (AORs), with 95% CIs, were used to estimate the strengths of the associations.
Ethics approval and consent to participate
Ethics approval was obtained from Madda Walabu University Ethics Review Committee (Ref. No. RDD/0098/13, given on 08/06/2013). The study conformed with the principles of the Declaration of Helsinki. First, a formal letter of permission and support was provided to Madda Walabu University Goba Referral Hospital by Madda Walabu University. Then, a letter was submitted to the hospital administrative body to obtain their consent for data collection. Informed written consent was obtained from each of the participants after explaining the aim, objectives and potential benefits of the study. Participants were informed regarding the confidentiality of their data and their right to refuse to complete the questionnaires and to withdraw at any time during the data collection. Patient confidentiality was maintained at all stages of the study. Participants who were diagnosed with DFU were referred to the diabetes clinic staff for treatment. Data were collected anonymously and are reported in aggregate.
Results
Socio-demographic characteristics of the participants
From the full list of patients under care (n = 1422), 271 patients were selected, and 267 completed the study (98.5%). The participants’ mean age was 49.9 years (SD ± 15.7 years) and the range was 18 to 86 years. Nearly a third, 94 (35.2%), had attended primary school; nearly two thirds, 182 (68.2%), lived in urban areas, and a quarter had a family history of diabetes mellitus (Table 1).
Socio-demographic characteristics of the study sample (n = 267).

Other*= day labourer or student.
Clinical and serum biochemical findings
Three quarters, 198 (74.2%), of the participants had type 2 diabetes, and 137 (51.3%) had confirmed comorbidities. A quarter, 68 (25.5%), had confirmed peripheral neuropathy, and 109 (40.8%) had hypertension. The mean systolic BP of the cohort was 133.55 mmHg (SD ± 20.86 mmHg) and the mean diastolic BP was 85.33 mmHg (SD ± 48.81 mmHg). More than four fifths, 227 (85.0%), had a fasting serum glucose concentration of ≥6.99 mmol/L. Half, 135 (50.6%), were administering insulin. More than half, 149 (55.8%), of the participants had total cholesterol concentrations <5.27 mmol/L. The majority, 226 (84.6%), had high (≥1.69 mmol/L) triglyceride concentrations, 148 (55.4%) had HDL-cholesterol concentrations of 1.16 to 1.55 mmol/L, and 237 (88.8%) had LDL-cholesterol concentrations <3.36 mmol/L. A majority, 240 (89.1%), of the participants had no foot callus (Table 2).
Summary of the clinical and serum biochemical parameters of the study sample (n = 267).
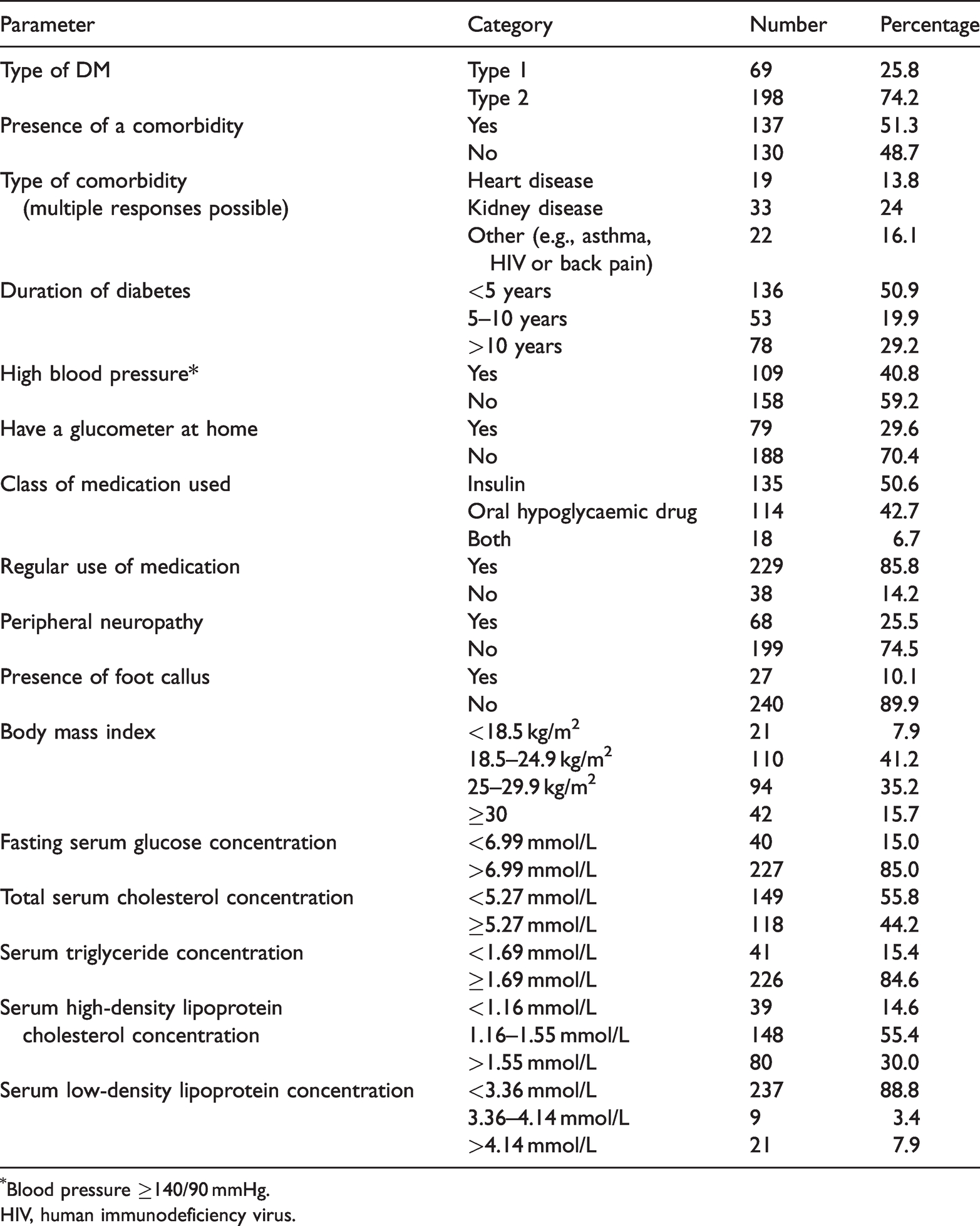
Blood pressure ≥140/90 mmHg.
HIV, human immunodeficiency virus.
Behavioural findings
Nearly one fifth of the participants, 44 (16.5%), had smoked cigarettes and 46 (17.2%) chewed chat. Similarly, one fifth, 57 (21.3%), had drunk alcohol. Two thirds, 175 (65.5%), of the participants undertook regular exercise (Table 3).
Behavioural factors in the study sample (n = 267).

Prevalence of diabetic foot ulcer
The overall prevalence of DFU was 11.2% (95% CI: 7.42–15.05). The majority of the participants had Grade 1 (40%) or Grade 2 (26.8%) ulcers (Figure 1).

Wagner classification of diabetic foot ulcers in patients with diabetes attending Goba Referral Hospital, south-east Ethiopia in 2021.
Diabetic foot self-care practice
One fifth, 56 (21%), of the participants sometimes walked barefoot. Nearly two thirds, 158 (59.2%), inspected their feet more than once a day; however, 173 (64.8%) never dried their legs using a towel. Over one third, 94 (35.2%), of the participants sometimes applied moisturising cream after washing their feet. Three quarters, 201 (75.3%), of the participants always inspected their shoes before wearing them, and 112 (41.9%) of the participants sometimes wore shoes without socks (Table 4). The overall prevalence of good diabetic foot self-care practice was 53.9% (n = 144; 95% CI: 47.9–59.9) and that of poor practice was 46.1% (n = 123).
Diabetic foot self-care practice by the study sample (n = 267).

Factors associated with diabetic foot ulcer
The independent variables included in the binary logistic regression analysis were age, sex, educational status, area of residence, presence of a comorbidity, regular use of medications, type of diabetes, duration of diabetes, history of smoking or drinking alcohol, chewing chat, regular exercise, peripheral neuropathy, presence of callus, BMI, fasting serum glucose concentration, and the serum concentrations of TG, LDL, HDL and total cholesterol. Variables with p < 0.25 were included in the multivariable logistic regression. The independent variables included in the final model were area of residence, performance of regular exercise, peripheral neuropathy, and presence of foot callus, because these were found to be significantly associated with DFU in the initial analysis.
Participants living in rural areas were found to be more than twice as likely to have DFU than those living in urban areas (AOR 2.27; 95% CI: 1.86–6.97). Participants who did not participate in regular exercise were almost four times more likely to have DFU than their counterparts (AOR 3.91; 95% CI: 1.51–10.10). Patients with peripheral neuropathy were found to be almost three times as likely to have DFU as those with no peripheral neuropathy (AOR 2.77; 95% CI: 1.05–7.33). Participants who had calluses on their feet were over five times more likely to have DFU than their counterparts (AOR 5.69; 95% CI: 1.74–18.59) (Table 5).
Factors associated with diabetic foot ulcer in the participants (n = 267).

Variable with p < 0.05 on multivariate analysis.
DFU, diabetic foot ulcer; COR, crude odds ratio; AOR, adjusted odds ratio; CI, confidence interval.
Factors associated with diabetic foot self-care practice
Multivariable analysis showed that being a woman, living in a town, having a glucometer at home, and having a long duration of diabetes were significantly associated with good foot self-care practice. Female participants were almost three times more likely to perform good foot care (AOR 2.95; 95% CI: 1.66–5.22) than men. Urban participants were twice as likely to practice good foot self-care as rural participants (AOR 2.01; 95% CI: 1.09–3.69). Similarly, participants who had a glucometer at home were twice as likely to practice good foot self-care than their counterparts (AOR 2.05; 95% CI: 1.09–3.85). In addition, participants who had had diabetes for >10 years were almost three times more likely to perform good foot care (AOR 2.92; 95% CI: 1.48–5.77) (Table 6).
Factors associated with diabetic foot self-care practice in the study sample (n = 267).

Variable with p < 0.05 on multivariate analysis.
COR, crude odds ratio; AOR, adjusted odds ratio; CI, confidence interval.
Discussion
In the present study, we determined the prevalences of DFU and good foot self-care practice, and identified the associated factors in patients attending Madda Walabu University Goba Referral Hospital, south-east Ethiopia. Of the 267 patients with diabetes that were studied, 11.2% had DFU during the study period. This finding was consistent with those of previous studies conducted in Ethiopia, which found the following prevalences: 11.6% in Jimma, 12 12% in Mekelle, 29 13.6% in Gondar, 24 14.8% in Arbaminch 39 and 12.98% nationally. 8 It is also consistent with the prevalence of 13% recorded for 19 African countries, 40 9.04% for a level 5 hospital in Nyeri, Kenya, 11% in Ghana, 41 14% in north India, 42 and 12% in Indonesia. However, the prevalence is lower than those reported for Harari Region (21.1%), 27 in two studies performed in Addis Ababa (31.1% and 20.7%),13,43 for Bahir Dar (17.05%) 30 and for Nekemte (17.86%). 32 The differences in prevalence may explained by differences in sample size, study design or study duration. In contrast, the calculated prevalence is higher than those calculated for Jordan (4.6%), 44 for Saudi Arabia (2.05%) 45 and worldwide (6.3%) 11 . These variations might be explained by differences in geographical location, study duration, health-seeking behaviours, and/or diabetic foot self-care practices. The prevalence calculated in the present study implies that diabetic complications are an ongoing problem, and they can result in leg amputation, hospitalisation and death. Therefore, all the stakeholders should be working hard to improve the prevention and reduce the risk of diabetic complications.
The prevalence of good diabetic foot self-care practice calculated in the present study was 53.9%, which is similar to those calculated in studies conducted in Bahir Dar (54.6%), north-west Ethiopia 31 and Thailand (50.7%). 25 However, it is higher than those calculated in studies conducted in Dessie (39%), north-east Ethiopia (39%), 19 India (19.4%), 46 Turkey (20.8%), 22 Lahore (14%) 21 and Malaysia 40.4%. 20 This might be explained by differences in sample size and/or the outcome variables. For example, the studies performed in India, Lahore and Malaysia categorised the standard of foot self-care as low, middle, and high, whereas in the present study, self-care practice was categorised as poor or good.
In the present study, living rurally, not performing regular exercise, peripheral neuropathy and foot calluses were found to be associated with DFU. Patients living in rural areas were 2.27 times more likely to develop DFU than those living in urban areas. This finding is consistent with the those of studies conducted in Gondar, Arbaminch, Mekele, Addis Ababa and north India.24,29,39,42,43 This may be because patients with diabetes who live in rural areas of Ethiopia often spend most of their time on farms or participating in outdoor activities; and therefore expose their feet to greater risk of abrasion, laceration or other injury, which can lead to the development of ulcers because of poor wound healing; living in rural areas may also be associated with a delay in seeking healthcare. 47 In addition, patients living in rural areas may lack awareness regarding personal hygiene and foot self-care practices, and often walk barefoot, even while working on a farm; predisposing themselves toward foot injury and the development of DFU.
We also found that patients with diabetes who did not perform regular exercise were at a higher risk of DFU. This finding is consistent with those of studies conducted in the Harari region of Ethiopia 27 and the Udupi district of India, 48 which showed that sedentary patients were twice as likely to develop diabetic foot. Similarly, a systematic review of the link between physical activity and diabetic foot-related outcomes revealed that physical activity and exercise are effective non-pharmacological interventions for the prevention and improvement of diabetic foot-related outcomes, because this is the primary strategy for the control of hyperglycaemia. 49 Thus, patients with diabetes who do not perform regular exercise may have poor blood glucose control, and therefore be at higher risk of diabetic complications, and particularly DFU. 49
We have also shown that patients with peripheral neuropathy are more likely to develop DFU than those without. This finding is consistent with those of studies conducted in Addis Ababa, 28 Gondar, 24 Pakistan, 50 Iran, 51 Australia 52 and Jordan. 44 Peripheral neuropathy is the result of direct damage to peripheral nerves, and causes weakness, pain and numbness, most often in the hands and feet. The prevalence of neuropathy among diabetic patients is relatively high, ranging from 16% to 66%, and increases the risk of DFU. 53
Patients with calluses on their feet were also found to be at higher risk of developing DFU, as shown previously. 8 Calluses develop secondary to peripheral neuropathy, leading to deformity and a lack of sensation, which results in persistent abnormal pressure on the foot. Skin cells react by greater keratinisation, resulting in a callus, which predisposes toward foot ulceration. 54
Diabetic foot self-care practice was found to be significantly associated with sex, the area of residence, the presence of a glucometer at home, and the duration of diabetes. Female patients were found to be more likely to practice foot self-care than men, which is consistent with studies conducted in north-east Ethiopia, 19 Malaysia 20 and Thailand. 25 This might be because men walk barefoot more often, do not check their feet as regularly, have poorer hygiene, and/or do not trim their nails appropriately. 55 Urban participants were more likely to demonstrate good foot self-care practice than participants living in rural areas, as previously shown to the Amhara region of Ethiopia.19,31 This may be explained by those who reside in rural areas spending more time outdoors, lacking awareness of foot care, and/or walking barefoot more often. In addition, differences in the socio-economic characteristics, health status, health beliefs and/or utilisation of healthcare may have explained these variations. 47
In the present study, we have also shown that patients with a glucometer at home are more likely to practice good diabetic foot self-care than their counterparts who do not have a home glucometer. This might be explained by those with a glucometer being better educated in diabetic preventive measures 56 and being more likely to attend routine check-ups, where they would be trained in integrated foot self-care practices. In addition, we have shown that those with a longer history of diabetes (>10 years) exhibited better foot care than those with a shorter history (<5 years), consistent with the results of studies conducted in Turkey 22 and Iraq. 57 A longer duration of disease provides more opportunity for patients to obtain advice from a healthcare provider, including with respect to foot self-care practices. The findings of the present study have significant clinical implications: they should alert local care-providers, hospital administrators, educators and other stakeholders to the importance of developing preventive strategies, which would increase quality of life, reduce the risk of hospitalisation, and minimise costs at the individual and family levels.
The present study had some limitations. First, it was conducted at a single institution, which limits our ability to generalise the findings to other populations. Second, the influence of behavioural factors might have been under- or overestimated because of the social desirability of participation and/or recall bias. Third, peripheral vascular sufficiency was not assessed in all of the participants, but this is associated with DFU, and may have affected its overall prevalence. In addition, HbA1c, which is frequently used to assess blood glucose status over the preceding 3 months and is more predictive of future complications of diabetes than blood glucose concentration, was not measured. Fourth, partially healed ulcers were classified according to their existing stage. Lastly, because this was a cross-sectional study, we cannot draw conclusions regarding cause-effect relationships.
Conclusion
The prevalence of DFU in patients with diabetes was found to be 11.2% in the present study setting. In total, 53.9% of the patients exhibited good foot self-care practice. Living in a rural area, a sedentary lifestyle, peripheral neuropathy and foot calluses were all found to be associated with DFU; and living in an urban area, having a glucometer at home and having had diabetes for a long time were associated with good foot self-care practice. Emphasis should be placed on integrating DFU risk assessment, education regarding prevention, including foot care, and the proper monitoring and management of blood glucose concentration.
Footnotes
Acknowledgements
The authors express special thanks to Madda Walabu University, the data collectors and supervisors, and the study participants.
Author Contributions
WN, TA, BS, AM, ZT, DS, HG, KB, YT, DZ, AT, AT, ZR, FD, TR, ZF, DA and TW contributed to the design of the study, the development of the proposal, data analysis, and drafting or revising the article. All agreed on the journal to which the article was submitted, gave final approval of the version to be published, and have agreed to be accountable for all aspects of the work.
Declaration of conflicting interests
The authors declare that there is no conflict of interest associated with this work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Madda Walabu University funded the data collection, but had no influence on the outcomes of the study.