
Abstract
Objective:
We measured the effects of a single bout of exercise on diurnal and nocturnal oxidative stress and glycaemic variability in obese subjects with type 2 diabetes mellitus or impaired glucose tolerance versus obese healthy controls.
Methods:
Subjects (in random order) performed either a single 30-min bout of moderate-intensity exercise or remained sedentary for 30 min at two separate visits. To quantify glycaemic variability, standard deviation of glucose (measured by continuous glucose monitoring system) and continuous overlapping net glycaemic action of 1-h intervals (CONGA-1) were calculated for three 12-h intervals during each visit. Oxidative stress was measured by 15-isoprostane F2t levels in urine collections for matching 12-h intervals.
Results:
Exercise reduced daytime glycaemic variability (ΔCONGA-1 = −12.62 ± 5.31 mg/dL, p = 0.04) and urinary isoprostanes (ΔCONGA-1 = −0.26 ± 0.12 ng/mg, p = 0.04) in the type 2 diabetes mellitus/impaired glucose tolerance group. Daytime exercise-induced change in urinary 15-isoprostane F2t was significantly correlated with both daytime standard deviation (r = 0.68, p = 0.03) and with subsequent overnight standard deviation (r = 0.73, p = 0.027) in the type 2 diabetes mellitus/impaired glucose tolerance group.
Conclusion:
Exercise significantly impacts the relationship between diurnal oxidative stress and nocturnal glycaemic variability in individuals with type 2 diabetes mellitus/impaired glucose tolerance.
Introduction
Investigations into the relationship between glycaemic variability and oxidative stress in diabetes have yielded conflicting results, with some investigators reporting a significant relationship1,2 but others not.3,4 One potential contributor to these inconsistent findings is, potentially significant, diurnal versus nocturnal differences in this relationship, which have not been systematically investigated.
Exercise has been shown to reduce both glycaemic variability 5 and oxidative stress,6,7 but these effects have not been simultaneously assessed. Thus, it is not known whether exercise-related decreases in glycaemic variability and oxidative stress are related.
The aims of this study were as follows: (1) to determine the correlated effects of aerobic exercise on glycaemic variability and oxidative stress in obese adults with type 2 diabetes mellitus (T2DM) or impaired glucose tolerance (IGT) as compared to healthy obese controls and (2) to define the distinct relationships between daytime and night-time parameters of glycaemic variability and oxidative stress.
Methods
Subjects
Physically untrained individuals 18–55 years of age, with T2DM of less than 7 years duration, and age- and body mass index (BMI)-matched individuals (controls) were recruited to participate in the study. Individuals were included if they had a BMI below 42, a haemoglobin A1c (HbA1c) < 9%, did not smoke, were not insulin-dependent and had no metabolic instability over the past 3 months. The study protocol was approved by the Institutional Review Board of the University of Illinois at Chicago.
Protocol
Subjects participated in two 3-day experimental periods, separated by at least 1 month. Prior to each experimental period, a maximal exercise stress test with VO2 measurement, an oral glucose tolerance test (OGTT) and resting energy expenditure assessment were conducted. Subjects were admitted (7 a.m.) to the General Clinical Research Centre for each experimental period. HbA1c was measured and a frequently sampled intravenous glucose tolerance test (FSIGTT) was performed, after which a standardized lunch and dinner were provided. Following dinner (around 17:00), a continuous glucose monitoring system (CGMS; Medtronic MiniMed, Inc.) was inserted. Monitoring was conducted for 36 h – from 7 pm on Day 1 to 7 am on Day 3 of admission. This period was broken into three 12-h segments (segment 1: 19:00–07:00; segment 2: 07:00–19:00; segment 3: 19:00–07:00) to allow separate determinations of nocturnal and diurnal relationships between glycaemic variation and oxidative stress using CGMS data and timed 12-h urine collections assayed for 15-isoprostane F2t levels.
Oral diabetes medication was withheld throughout each visit and resumed just prior to discharge. Starting at 21:00 on Day 1, subjects fasted from food and drink. On Day 2, subjects participated in either a sedentary or exercise session (one during each visit, in randomized order). The exercise session comprised 30 min of treadmill walking at 65% VO2max in the morning, while during the sedentary session subjects remained inactive. During the remainder of the day, subjects were fed three standardized meals. Subjects spent Night 2 in the General Clinical Research Centre. On Day 3, following breakfast, subjects were discharged.
Glycaemic variability
Glycaemic variability was assessed by calculating two measures for each 12-h segment: (1) the standard deviation (SD) of the 5-min glucose values and (2) continuous overlapping net glycaemic action of 1-h intervals (CONGA-1); herein referred to as CONGA. 8
Oxidative stress
Urinary 15-isoprostane F2t levels were quantified by competitive enzyme-linked immunoassay using a central laboratory. Levels are reported in ng/mg creatinine.
Statistical analysis
Paired t-tests were used to assess differences in glycaemic variability, mean glucose and oxidative stress between exercise and sedentary days. t-tests were used to assess differences between groups. A p value < 0.05 was considered to be significant. Bivariate Pearson’s correlations and regression analysis were used to define relationships among glucose SD, CONGA and 15-isoprostane F2t for each 12-h segment.
Six of the intended control subjects were found to have IGT, defined as a plasma glucose level between 110 and 126 mg/dL, 2 h after oral glucose load. For analysis purposes, subjects with IGT were included with the T2DM subjects.
Results
The control group comprised 20 subjects (5 men) with an average age of 43.5 years [10.44 (SD)], average BMI of 34.76 kg/m2 (3.25) and average HbA1c of 5.1% or 32 mmol/mol (0.4% or 4 mmol/mol). The combined T2DM/IGT group included 17 subjects (3 men) with an average age of 46.53 years (6.10), average BMI of 36.86 kg/m2 (3.79) and average HbA1c of 6.4% or 46 mmol/mol (0.9% or 10 mmol/mol).
As shown in Figure 1(a), exercise, as compared to sedentary behaviour, produced a significant decrease in daytime (segment 2) urinary 15-isoprostane F2t in the T2DM/IGT group [exercise: 1.32 ± 0.14 ng/mg (0.42 ± 0.05 µmol/mol) vs sedentary: 1.58 ± 0.16 ng/mg (0.5 ± 0.05 µmol/mol), p = 0.04], but no significant change in the control group. Furthermore, the daytime exercise-related decrease in the T2DM/IGT group [−0.26 ± 0.12 ng/mg (−0.08 ± 0.04 µmol/mol)] was significantly different from the change among control subjects [0.15 ± 0.11 ng/mg (0.05 ± 0.04 µmol/mol); p = 0.02].
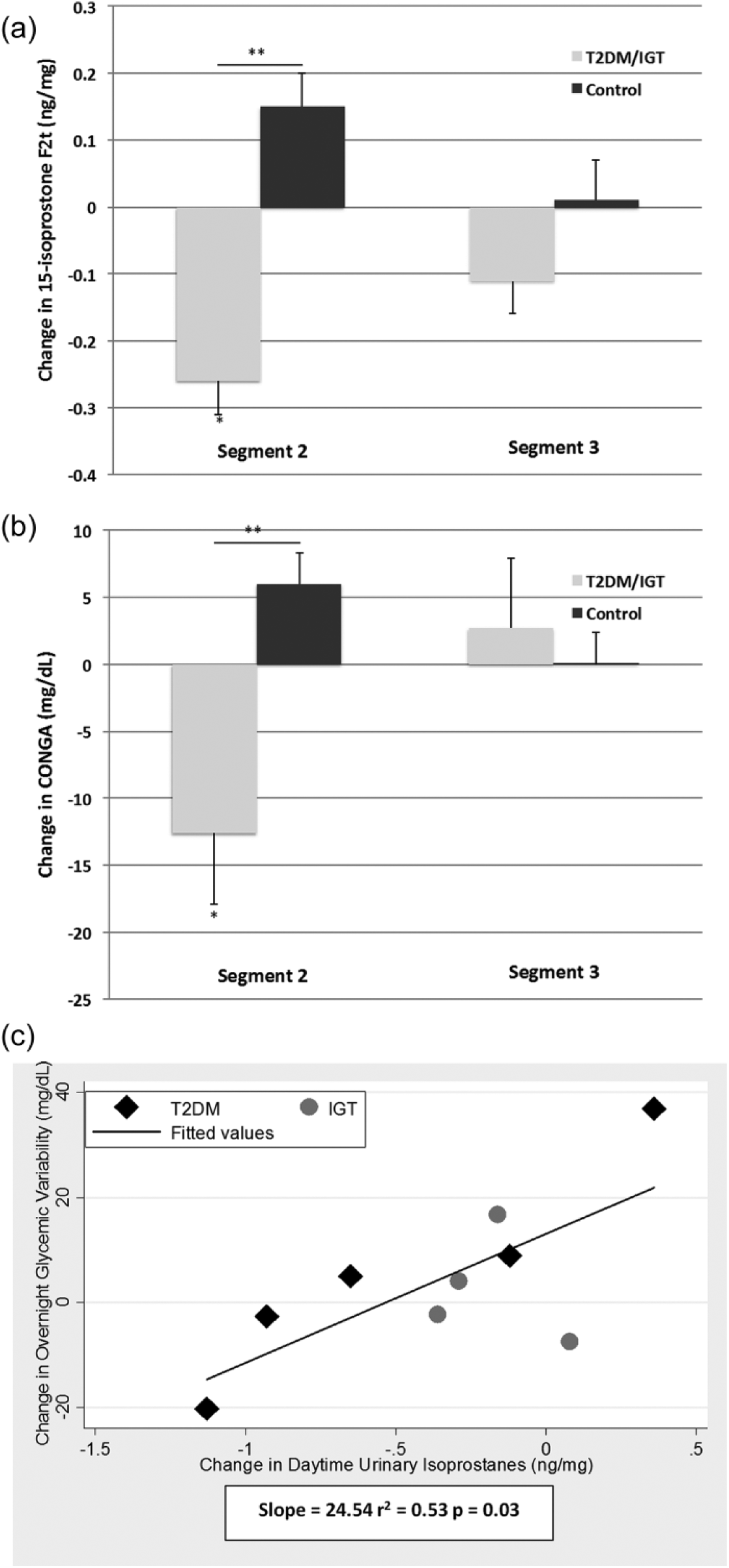
(a) Exercise-related change in urinary 15-isoprostane F2t. In the T2DM/IGT group, exercise was associated with significantly decreased daytime (segment 2) urinary 15-isoprostane F2t in comparison with sedentary conditions (*p = 0.04) and with respect to the change in controls (**p < 0.02); (b) exercise-related change in CONGA. In the T2DM/IGT group, exercise was associated with significantly decreased daytime (segment 2) CONGA in comparison with sedentary conditions (*p = 0.04) and with respect to the change in controls (**p < 0.005) and (c) prediction of overnight glycaemic variability by daytime urinary 15-isoprostane F2t. Exercise-related change in daytime urinary 15-isoprostane F2t levels predicts change in subsequent overnight glycaemic variability in subjects with T2DM/IGT.
Daytime glycaemic variability (segment 2 CONGA; Figure 1(b)) was significantly decreased by exercise in the T2DM/IGT group [mean change: −12.62 ± 5.31 mg/dL (−0.70 ± 0.30 mmol/L), p = 0.005 vs change in controls; exercise: 20.53 ± 2.09 (1.14 ± 0.12 mmol/L) vs sedentary: 33.15 ± 5.59 mg/dL (1.84 ± 0.31 mmol/L), p = 0.039]. A similar pattern was observed for segment 2 SD, but the difference failed to reach statistical significance [exercise: 22.02 ± 3.66 mg/dL (1.22 ± 0.20 mmol/L) vs sedentary: 31.44 ± 6.37 mg/dL (1.75 ± 0.35 mmol/L), p = 0.15].
No significant correlation existed between absolute urinary 15-isoprostane F2t level and either CONGA or SD of glucose within any 12-h segment. In contrast, the daytime (segment 2) exercise-induced change in urinary 15-isoprostane F2t was significantly correlated with both daytime SD (r = 0.68, p = 0.03) and with subsequent overnight (segment 3) SD (r = 0.73, p = 0.027) in the T2DM/IGT group but not the control group, with greater exercise-related increases in daytime urinary 15-isoprostane F2t on predicting higher daytime and subsequent overnight (Figure 1(c)) glycaemic variability in the T2DM/IGT group. When the IGT group was excluded, the relationship was strengthened for the T2DM group (r2 = 0.90; slope = 32.33; t = 5.20; p = 0.01). CONGA demonstrated the same pattern as SD, but the correlations did not reach statistical significance.
Discussion
This study demonstrates that a single bout of moderate-intensity early morning exercise reduced urinary 15-isoprostane F2t levels and glycaemic variability in obese T2DM/IGT subjects. These exercise-related reductions in oxidative stress and glycaemic variability were correlated during the daytime, but not during the subsequent overnight period. Despite this, the change in daytime urinary 15-isoprostane F2t level following exercise strongly predicted subsequent overnight change glycaemic variability in individuals with T2DM or IGT.
Previous investigations reported mixed findings regarding the baseline relationship between glycaemic variability and oxidative stress in adults with T2DM.2,3 We found a significant positive correlation between urinary isoprostanes and glycaemic variability but only after moderate exercise and only in subjects with T2DM/IGT. Furthermore, this relationship was apparent only during the daytime period immediately following the exercise bout. Previous groups have not considered potential diurnal/nocturnal shifts in this relationship.
The specific mechanism(s) by which a single brief early morning bout of aerobic exercise decreased daytime levels of urinary 15-isoprostane F2t and glycaemic variability in subjects with T2DM/IGT cannot be determined from this study. It is noteworthy that the magnitude of the exercise-related decrease in daytime isoprostane level was positively and significantly related to the subsequent decrease in both daytime and overnight glycaemic variability. To the best of our knowledge, this relationship between daytime markers of oxidative stress and subsequent overnight glycaemic variability has not been reported previously.
One possible explanation is that improved insulin sensitivity following exercise resulted in decreased oxidative stress. Indeed, increased oxidative stress has been related to increased insulin resistance in skeletal muscle.9,10 Moreover, sleep is characterized by intermittent perturbations to glucose homeostasis. Subjects with less exercise-related improvement in daytime insulin sensitivity, reflected as higher levels of oxidative stress, may have been more vulnerable to these neurohumoral disturbances to insulin sensitivity during the subsequent sleep period, thus exhibiting increased nocturnal glycaemic variability. Still, it cannot be ruled out that subjects with greater overnight glycaemic variability were simply individuals with continuously high glycaemic variability. In this case, daytime 15-isoprostane F2t levels may have acted as a biomarker for daytime glycaemic variability.
Circadian modulation also may play a role. Melatonin is a key circadian synchronizing factor. Mutations in the melatonin receptor are associated with increased incidence of T2DM 11 and various evidence suggests that reduced melatonin secretion can lead to insulin resistance. 12 It is plausible that exercise-induced reduction of systemic inflammatory processes may have allowed blunting of the circadian impairment in glucose regulation during the subsequent night. Future studies including direct melatonin assays or utilizing delayed sleep paradigms will be required to better assess the relationship between systemic inflammatory markers and glucose regulation. In conclusion, our results demonstrate that a single bout of moderate-intensity exercise reduces both oxidative stress and glycaemic variability in obese subjects with T2DM and IGT. Moreover, individuals exhibiting greater decreases in oxidative stress immediately following exercise also demonstrate improved glycaemic control during the subsequent overnight period.
Footnotes
Declaration of conflicting interests
The authors declare that they have no conflict of interest.
Funding
This study was supported by NIH-NINR R01 NR07760.