
Abstract
Aims:
This review is aimed at highlighting the potential mitogenic/tumour growth–promoting or antimitogenic/tumour growth–inhibiting effects of the main antihyperglycaemic drug classes.
Methods:
We review and discuss the most current studies evaluating the association between antidiabetic medications used in clinical practice and malignancies as described so far.
Results:
Metformin seems to be the only antidiabetic drug to exert protective effects both on monotherapy and also when combined with other oral antidiabetic drugs or insulins in several site-specific cancers. In contrast, several other drug classes may increase cancer risk. Some reason for concern remains regarding sulphonylureas and also the incretin-based therapies regarding pancreas and thyroid cancers and the sodium glucose cotransporter-2 inhibitors as well as pioglitazone regarding bladder cancer. The majority of meta-analyses suggest that there is no evidence for a causal relationship between insulin glargine and elevated cancer risk, although the studies have been controversially discussed. For α-glucosidase inhibitors and glinides, neutral or only few data upon cancer risk exist.
Conclusion:
Although the molecular mechanisms are not fully understood, a potential risk of mitogenicity and tumour growth promotion cannot be excluded in case of several antidiabetic drug classes. However, more large-scale, randomized, well-designed clinical studies with especially long follow-up time periods are needed to get reliable answers to these safety issues.
Introduction
Up to now, the number of people suffering from diabetes mellitus reached approximately 382 million people worldwide, and the number is estimated to rise to 592 million by 2035. 1 The incredible dynamic of the increase in the number of diabetic patients becomes clearer if we take into account the number of people affected 14 years ago: in 2000, only half as much, approximately 171 million people were reported to suffer from diabetes worldwide. 2
Alongside with increasing numbers of people suffering from diabetes, there is also a parallel rise in patients suffering from cancer, which is the second cause of death after cardiovascular diseases worldwide. In 2008, 12.7 million patients suffered from cancer, and there is a predicted increase in the incidence of all-cancer cases to 22.2 million by 2030. 3
Several epidemiological studies in many different populations have shown a relationship between type 2 diabetes mellitus and cancer risk. It appears as if both type 2 diabetes and obesity, as its key risk factor, are independently associated with an elevated risk of cancer incidence and with a poorer prognosis, namely, cancer-related mortality. For a comprehensive list of studies and clinical trials, see recent systematic reviews.4–13 As already shown in several meta-analyses, patients with type 2 diabetes have an elevated risk of pancreatic, bladder, hepatocellular, ovarian, breast, endometrial, renal, gastric, colorectal and thyroid cancers and, moreover, of non-Hodgkin’s lymphoma, leukaemia and myeloma.14–24 The underlying mechanisms are subject to ongoing investigations, but relevant factors appear to be hyperinsulinaemia due to either insulin resistance or insulin-based therapy, hyperglycaemia, hyperlipidaemia, altered levels of circulating oestrogens and androgens, and inflammatory processes, which have all been associated with an increase in cancer incidence and/or cancer mortality.
Besides the anticipated beneficial effects, we should keep in mind that all antihyperglycaemic therapies that are in clinical use today also display – less or more severe – adverse effects. In recent years, there is ongoing debate as to whether diabetes therapy itself may also influence cancer risk beyond the already mentioned increased risk of cancer due to the diagnosis of diabetes, and if yes, does it display a positive or a negative impact on cancer incidence and prognosis. Moreover, it is still unclear and under broad discussion whether some glucose-lowering therapies may be capable of directly inducing malignancy or only lead to an enhanced proliferation of pre-existing malignant cells. In the last years, there was a great number of studies published focusing on the risk of cancer in diabetic patients, especially in patients who received insulin or insulin analogues and, moreover, who were treated with metformin. Beyond such antidiabetic treatments that have been used in clinical practice for many years, further oral antidiabetic therapies have been newly developed in recent years without a long observation period and without a long-term clinical experience. Especially with regard to the last group, some of their biological functions are still not fully understood.
The subject of this review was therefore to highlight potential mitogenic/tumour growth–promoting or, alternatively, antimitogenic/tumour growth–inhibiting effects of the main antihyperglycaemic drug classes used in clinical practice as described so far and to give an update on current knowledge in this field. Here, we review and discuss the most current publications on antidiabetic medications with regard to an impact on cancer incidence and mortality.
Cancer risk of different antidiabetic therapies
Insulin sensitizers and cancer risk: biguanides and thiazolidinediones
Metformin
Metformin belongs to the biguanide group of antihyperglycaemic therapies used meanwhile for many years in clinical practice and is considered as a safe drug for type 2 diabetes with no risk of hypoglycaemia. Metformin displays several beneficial effects as it improves insulin sensitivity, decreases hepatic glucose output and leads to moderate weight loss.25–29 Besides, only little adverse effects are reported, and the most serious but rare adverse effect is lactic acidosis.
Several molecular mechanisms of metformin interfere with signalling pathways that are involved in cell growth, proliferation and apoptosis. One main mechanism of metformin is the activation of 5′ adenosine monophosphate–activated protein kinase (AMPK) through the tumour suppressor protein kinase, liver kinase B1 (LKB1). AMPK activation inhibits the mammalian target of rapamycin (mTOR) pathway, a pathway often activated in tumour cells. Inhibition of mTOR reduces protein synthesis, induces cell cycle arrest and apoptosis and decreases cancer cell growth in vitro.30–34 Moreover, metformin decreases hepatic glucose output, which indirectly leads to reduced hyperinsulinaemia and ameliorates insulin resistance. An in vivo study with metformin reported slower tumour growth in high-fat diet–fed mice displaying hyperinsulinaemia compared to mice on the control diet without hyperinsulinaemia, pointing to the lowering of insulin levels as a presumably important factor for metformin to reduce tumour growth. 35 In a recent study, metformin exerted actions on cancer stem cells suppressing the inflammatory response in cancer. 36 Further potential mechanisms on how metformin exerts its protective antimitogenic/tumour growth–inhibiting effects are still under investigation.
Due to the long time of clinical experience with this drug, up to now numerous studies have examined the impact of metformin on cancer survival and mortality in people with type 2 diabetes. Meanwhile, a large number of mostly retrospective case–control studies exist, indicating a cancer risk–reducing effect of metformin.30,37–47 A recent meta-analysis including five observational studies referred to an overall reduced cancer incidence of approximately 31% in patients taking metformin compared to those who used other glucose-lowering drugs, 48 and moreover, metformin is also reported to protect from cancer-related mortality.41,49–51 Besides protective effects in use as monotherapy compared to alternative glucose-lowering therapies, such as insulin secretagogues or insulin-based therapies, metformin is also capable of reducing the cancer risk when used in combination with sulphonylureas or with insulin, compared to sulphonylurea and insulin monotherapy, respectively. 38 Moreover, in 2529 type 2 diabetic women suffering from early-stage breast cancer, an additive metformin therapy leads to more frequent pathologic complete response rates in combination with a neoadjuvant chemotherapy compared to women receiving no metformin, but only the chemotherapy. 52
However, until now, only few randomized controlled trials (RCTs) are published, which investigated the cancer mortality in adults using metformin. One systematic review and meta-analysis included, in parallel to four cohort studies, two large RCTs in people with type 2 diabetes, namely, the ‘A Diabetes Outcome Progression Trial’ (ADOPT), a monotherapy study on the glucose-lowering effects of metformin, rosiglitazone and glibenclamide, including 1454, 1456 and 1441 individuals, respectively, and the ‘Rosiglitazone Evaluated for Cardiovascular Outcomes and Regulation of Glycaemia in Diabetes’ (RECORD) comparator clinical trial, a cardiovascular outcome study with rosiglitazone or metformin added to sulphonylurea compared to rosiglitazone or sulphonylurea added to metformin.53–55 This meta-analysis revealed a significantly lower risk of all-cancer mortality and incidence in diabetic patients using metformin. Another, and until now the most comprehensive, systematic review included, in addition to the two mentioned RCTs, seven more RCTs investigating cancer mortality of metformin compared with other glucose-lowering therapies or with placebo or usual care including RCTs with at least 500 participants and at least 1-year follow-up. 56 In line with the previous study, this meta-analysis could not detect any significant beneficial effect of metformin on cancer mortality either. However, the results of these studies should be interpreted with caution due to the following limitations of these trials: the nine RCTs included in the analysis were not designed a priori to examine cancer-related endpoints except the two ‘UK Prospective Diabetes Study Group’ (UKPDS) trials, but rather with the intention to collect data on diabetes-related endpoints. Another limitation is the large clinical heterogeneity of the trials, for example, the target population was in some studies a collective at risk of diabetes, while other studies were designed for people with type 2 diabetes. Furthermore, and very important to note, a limitation of the RCTs involved in this study with regard to cancer-related mortality is the short average follow-up time of 4.1 years, taking into account that, in several observational studies, the effect of metformin on cancer becomes more evident after 5 years of use. 48
Thus, metformin therapy does not have the same impact on all cancer types, pointing to site-specific effects on tumour growth. Metformin use is reported to site-specifically reduce the risk of certain types of cancer, especially colon, liver, breast and pancreatic cancers, but to have no impact on prostate cancer.38,40,42,57–62 Considering potential postulated mechanisms for metformin, for example, the inhibition of the nuclear translocation of the c-AMP response element–binding protein (CREB)–regulated transcription co-activator 2 through AMPK 63 and suppression of the expression of aromatase, 64 it is conceivable that metformin suppresses oestrogen levels in the breast, which might be an important way to protect against oestrogen receptor–positive breast cancer. In line with this, metformin was shown to inhibit breast cancer cell growth and colony formation inducing cell cycle arrest in vitro, 34 but it is also reported to act in triple-negative breast cancer (TNBC) cells in vitro. 65 Moreover, in several recent observational studies, evidence is rising that metformin may exert a synergistic protective effect when combined with chemotherapy.36,52
Although numerous in vitro cell line studies and lessons from rodents support the hypothesis that metformin has an antimitogenic effect, further trials will surely help to clarify the risk-reductive impact of metformin on site-specific cancers in future. As most published studies investigated the impact of metformin on cancer in comparison with other glucose-lowering therapies, such as sulphonylurea derivates or other insulin-based therapy regimens, and not with placebo-controlled populations, it remains questionable whether metformin may directly reduce cancer risk, or on the contrary, the compared therapies themselves may be associated with a higher cancer risk, finally leading to a possible overestimation of the anti-cancer properties of the drug. Because of its potent glucose-lowering effect, examining the impact of metformin on cancer in a non-diabetic population is difficult, and human studies in this regard are sparse. Although patients with type 2 diabetes display a higher risk of cancer as mentioned above, a recent retrospective cohort study reported a significantly reduced overall mortality of diabetic patients receiving metformin monotherapy even compared to a population without diabetes. 39 In another human randomized study of non-diabetic women with operable breast cancer, a 2-week metformin therapy prior to the surgery led to decreased cell proliferation, implicating direct protective biological impact of metformin on cancer cells. 66 Besides this human study, lessons from rodents point to a cancer risk–reducing effect of metformin in the absence of diabetes. 67 Thus, these human studies together with in vitro data suggest an independent antimitogenic impact of this drug. However, there is still a big need for more long-term RCTs comparing metformin with either placebo or usual care to answer this question.
Thiazolidinediones
The insulin sensitizers thiazolidinediones (TZDs) enhance the binding of peroxisome proliferator–activated receptor γ (PPARγ) to its DNA response element, leading to an increase in glucose uptake by skeletal muscle, reducing hepatic glucose production, decreasing liver fat, increasing lipolysis and improving whole-body insulin sensitivity.68,69 Two representatives of this group are pioglitazone and rosiglitazone. Rosiglitazone is, due to increased risk of adverse cardiovascular events, not approved any longer in Europe, and the Food and Drug Administration (FDA) also restricted its use.
Previous in vitro and in vivo animal studies were designed to answer the question whether TZDs may modify cancer risk, and the results of these studies are equivocal. Numerous studies pointed to a tumour suppressor effect of the TZDs reporting an impact on angiogenesis, inhibition of cell differentiation and invasion, cell cycle arrest and induction of apoptosis.70–80 Of note, this antimitogenic effect of TZDs may be independent of PPARγ itself, raising the need for further investigations regarding accurate molecular mechanisms. 81
In the meantime, several clinical trials are available linking TZD treatment to cancer incidence and survival in humans, although, also in this regard, conflicting results are reported with regard to site-specific cancers and differences between different representatives of this drug class. On the one hand, epidemiological studies exist, providing evidence for a possible protective effect of rosiglitazone, in particular with regard to lung cancer. 82 A very recently published meta-analysis included 22 RCTs reporting at least one cancer, enrolling 13,197 patients on TZD therapy (3710 on pioglitazone and 9487 on rosiglitazone) and 12,359 patients on placebo or active comparator groups. 83 This meta-analysis revealed a significant reduction in the incidence of overall malignancies in people treated with TZDs without any difference between rosiglitazone and pioglitazone. Another large meta-analysis which was set up to investigate the antimitogenic effect of rosiglitazone, retrieving 80 RCTs with 16,332 and 12,522 individuals in the rosiglitazone and comparator groups, respectively, was published by the same authors in 2008. The results of this meta-analysis also point to a lower cumulative incidence of cancer in people who received rosiglitazone, although there was no significant modification of cancer risk found with rosiglitazone. 84 Beyond studies reporting a possible protective effect of TZDs, further reports point to an at least neutral effect of TZDs with regard to cancer, suggesting the use of TZDs to be safe. A systematic review and meta-analysis of 17 observational studies could not confirm any association of the use of TZDs with risk of overall cancer. 85
On the other hand, however, some in vitro and rodent studies reported an enhanced mitogenic potential of the TZDs, especially regarding bladder and colon cancer.86–93 Indeed, when looking at site-specific cancers in humans, the positive association between pioglitazone and bladder cancer risk appears striking. While TZDs are not reported to rise overall cancer risk in humans, and in several studies are even associated with lower overall cancer risk, by now, numerous studies and systematic reviews exist, pointing to a higher risk of bladder cancer for patients treated with pioglitazone.83,85,91–96 First, evidence was given in this regard by the prospective randomized multicentre PROactive study that was designed for cardiovascular endpoints in 5238 people with type 2 diabetes. 97 In addition, the cancer risk was increasing with the dose exposure and when applied in a long-term way.93,98 Finally, the studies point to a particular drug-specific effect of pioglitazone as rosiglitazone did not raise the risk.
Regarding further detailed examination of TZD impact on site-specific cancers, the clinical trials investigating the association between TZD therapies and cancer risk have yielded inconsistent results. In contrast to bladder cancer and – if we take into account the few in vitro and rodent studies – to some extent also colon cancer, the risks of other site-specific cancers were reported to be either unaffected or even lowered by TZD use. In an already mentioned work, a retrospective case–control study obtained from the ‘Veterans Integrated Services Network 16’ (VISN 16) enrolling 87,678 individuals suggested a 33% reduced risk of lung cancer in patients treated with TZDs compared to non-users, 82 while in a nationwide case–control study from Taiwan with 606,583 type 2 diabetic patients included, no association was found between TZD therapy and lung cancer incidence. 99 In the same study, a significantly lower risk of liver cancer in patients using either rosiglitazone or pioglitazone was found, and the protective effects were reported to be stronger when the cumulative dosage was higher and the duration of the treatment longer, whereas in another systematic review and meta-analysis including 334,307 patients with type 2 diabetes, TZDs did not change the risk of hepatocellular cancer. 100 With regard to colorectal cancer, human studies do not confirm the in vitro and rodent findings. A systematic review and meta-analysis reporting 13,871 cases of colorectal cancer in 840,787 diabetic patients did not support an association between TZD use and colorectal cancer. 101 Moreover, in a very recently published 6-year population-based cohort study, even a dose-dependent decrease in cancer risk in diabetic patients using TZDs was reported regarding several site-specific cancers, including colorectal cancer and, in addition, breast, brain, uterus, stomach, prostate, ear–nose–throat, kidney, lung and lymphatic malignancies. 102
Few further reports exist regarding breast cancer risk. In the mentioned recent meta-analysis of RCTs, a significant reduction in breast cancer risk for pioglitazone, but not rosiglitazone, was attested. 83 This finding is supported by another meta-analysis including data from 3 case–control and 14 cohort studies that reported no association of TZDs with breast cancer. 85 Three nested case–control studies conducted among 126,971 patients with diabetes that focused on colon, prostate and breast cancers did not support a beneficial or a deleterious impact of TZDs on any of these cancer sites. 103 At least for troglitazone, a TZD which is in the meantime withdrawn from commercial use because of warnings for hepatic toxicity, little clinical value was attested in a phase 2 study including 22 patients with advanced breast cancer. 104 Of note, besides the potential mitogenic effect of pioglitazone regarding bladder tumour, troglitazone is the second TZD which was shown at least in rodents to raise the risk of a specific cancer, namely, hemangiosarcoma.105–108
Furthermore, as mentioned above, antihyperglycaemic drugs may not only act as suppressors or enhancers of cancer cell growth, or maybe also as initiators of cancer, they might also interfere with anti-cancer therapies. Phase 1 clinical trials indicate that efatutazone, a novel oral PPARγ agonist, combined with chemotherapy may have an acceptable safety profile and anti-tumour activity in advanced malignancies.109–111 Moreover, rosiglitazone was reported to enhance the radiosensitivity of human colorectal cancer cells. 112 Such interactions are of crucial clinical relevance, but studies in this regard are rare. Thus, the particular impact of each individual TZD drug on cancer may differ and has to be investigated carefully, and the results should be interpreted with caution.
Of note, one study among type 2 diabetic individuals pointed to a possible gender-dependent association between TZD use and cancer reporting a lower risk particularly among women who were treated with rosiglitazone. Interestingly, the same correlation was not found for pioglitazone. 113 As mentioned by the authors, this result is difficult to explain and needs further investigations to clarify whether this gender-stratified association is causal.
In summary, it has to be emphasized that a definitive conclusion regarding TZDs’ impact on modifying cancer risk, especially on site-specific cancers, is difficult due to the paucity of appropriately designed and sized randomized long-term clinical studies that should be set up to answer this particular question. Moreover, it should be taken into account that most reports that tried to clarify the TZD impact on cancer incidence and mortality until now were unable to explore the long-term effects of TZDs on cancer due to their relatively short treatment duration. On the basis of the available studies for the moment, TZD use appears to be safe with respect to cancer incidence with one exception: studies raise concerns on pioglitazone use because of the reports on bladder cancer incidence. Further studies are needed to clarify the potential impact of pioglitazone regarding this site-specific cancer.
Insulin secretagogues and cancer risk
Sulphonylureas
Sulphonylureas (e.g. glimepiride, glipizide and glibenclamide) bind to the pancreatic β-cell receptor sulphonylurea receptor 1 (SUR1) and inhibit the adenosine triphosphate (ATP)-dependent potassium channel Kir6.2 leading to cell depolarization and subsequent calcium influx into the β-cell. This triggers insulin release from the intracellular stores independently of glucose. 114 Sulphonylureas may lead to severe hypoglycaemia as serious side effect of this drug class.
Strong evidence from several epidemiological studies exists that points to an enhanced cancer risk in case of endogenous hyperinsulinaemia. 115 The underlying mechanisms will be discussed later when insulin therapy and insulin analogues and their potential impact on cancer will be systematically highlighted. As sulphonylureas are used to improve insulin secretion in β-cells when insulin resistance in type 2 diabetes occurs, they increase circulating insulin levels, potentially raising the risk of tumour growth.
Indeed, several epidemiological studies found an association between sulphonylurea use and cancer risk, and the majority of these studies reported an increased risk of cancer incidence and cancer-related mortality when type 2 diabetic patients were treated with sulphonylureas compared to patients exposed to metformin.38,43,44 Of note, as discussed elsewhere, based on these comparator studies, it is not possible to answer the question whether sulphonylureas may have mitogenic effects, metformin antimitogenic ones, or even both occur, as in the majority of the studies metformin was used as comparator drug. 43 A comprehensive meta-analysis addressed this question involving 315,517 people on type 2 diabetes. This meta-analysis reported a significantly increased all-cancer risk in patients treated with sulphonylureas compared to non-sulphonylurea users, however, only when based on the cohort studies included in the analysis. By contrast, the data from two RCTs could not confirm this result. 116 In this regard, it remains further unsolved whether the suggested mitogenic effects of sulphonylureas may be direct ones on tumour cells or actually indirect ones due to the hyperinsulinaemia following sulphonylurea treatment.
Regarding specific cancer sites, results from systematic meta-analyses indicated evidence for elevated risk of pancreatic, hepatocellular and colorectal cancer among diabetic patients with sulphonylurea treatment, although, regarding colorectal cancer, only a trend toward higher cancer risk could be detected among sulphonylurea users.100,101,117
However, when we carefully review the available preclinical and clinical data, it becomes apparent that, despite the univocal antimitogenic data for metformin, the impact of sulphonylureas on tumour growth is much less clear. In this context, it is important to consider that sulphonylureas represent a drug class of rather diverse biochemical substances with different pharmacokinetic and pharmacodynamic properties. This may explain the different outcomes of the drugs in the available preclinical and clinical studies concerning tumour growth, cancer incidence or mortality.
Regarding the preclinical data, several studies point to an antimitogenic effect of sulphonylureas. For a recent and comprehensive overview, see the study by Pasello et al. 118 In this work, the authors give a broad resume of the current knowledge regarding the antimitogenic effects of sulphonylureas and, moreover, specify the proposed antimitogenic mechanism of individual representatives of this drug class. As reported in this overview, numerous studies exist, suggesting a tumour growth–inhibitory effect of glibenclamide and, in few further studies, also gliclazide, but no evidence of an antimitogenic effect of glimepiride and glipizide. However, the authors also indicate that there is conflicting epidemiologic evidence regarding cancer incidence in patients treated with sulphonylureas.
By way of example, in contrast to the in vitro results mentioned above, a retrospective cohort study performed on 568 patients reported glibenclamide to be associated with a higher mortality due to malignancies compared to gliclazide, 119 and moreover, the same group reported in an observational cohort study including 2002 diabetic patients that, when combined with metformin, glibenclamide was associated with a higher mortality than gliclazide and also glimepiride, a third-generation sulphonylurea. 120 For the sake of completeness, it should be mentioned that few systematic studies exist displaying no impact of sulphonylureas on the risk of cancer at any site. 121 Thus, the mitogenic effects of the individual sulphonylurea compounds are currently equivocal, stressing the continuing demand for RCTs for further clarification.
Meglitinides (glinides)
Regarding their structure and their main molecular mode of action, namely, inhibiting the ATP-dependent potassium channel in pancreatic β-cells leading to release of insulin secretory vesicles, glinides (e.g. repaglinide and nateglinide) are closely related to the sulphonylureas. Therefore, the glinides are expected to have similar side effects. However, to our knowledge, no comprehensive studies exist exploring the risk of cancer under glinide treatment. In vitro, a very recent work attested repaglinide anti-cancer properties. 122 However, a nested case–control study from Barcelona with 275,164 type 2 diabetic patients included could not find evidence for altered cancer risk when treated with repaglinide compared to insulin-based therapies or other oral glucose-lowering drugs, including metformin, sulphonylureas and TZDs. 123 Because of the lack of suitable studies, no further information is available concerning a potential effect of this drug class on cancer incidence and mortality.
Incretin-based therapies and cancer risk
Incretins are insulinotropic gut hormones including glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP). It is well known that incretins regulate blood glucose by triggering insulin secretion and suppressing glucagon secretion in response to orally ingested glucose. 124 Moreover, they induce pancreatic β-cell proliferation and regulate cell differentiation and apoptosis.125–127 Incretin-based therapies represent a relatively new, but in the meantime also frequently prescribed, group of antihyperglycaemic drugs that are based either on GLP-1-receptor activation or on inhibiting the GLP-1–metabolizing enzyme dipeptidyl peptidase IV (DPPIV). In the following, the available preclinical and clinical human data on these medications with regard to modifying cancer risk will be reviewed.
GLP-1 agonists
The two GLP-1 agonists actually used in type 2 diabetes therapy, exenatide and liraglutide, are in general considered to be safe and well-tolerated drugs with only few adverse effects reported, such as nausea and mostly mild hypoglycaemia. Beyond this, however, two particular adverse effects have been reported in the meantime by numerous investigators, that is, warnings of potentially increased risk of acute pancreatitis and pancreatic cancer and of thyroid cancer. 128 The association with pancreatitis and pancreatic cancer was not only reported for GLP-1 agonists but also for DPPIV inhibitors, which will be discussed later on.
As exenatide, the first GLP-1–based therapy, is used since 2005 for the treatment of type 2 diabetes and liraglutide since 2010, more studies exist regarding exenatide treatment and cancer risk. Strong evidence for exenatide to evoke pancreatitis was reported from studies on rodents. Of note, pancreatitis is reported as a risk factor of pancreatic cancer in several publications.129,130 Histological analysis of the pancreas yielded in several rat and mouse studies evidence for acinar inflammation and formation of dysplastic lesions, for example, increased ductal turnover after exenatide treatment. 131 Moreover, exenatide was shown to accelerate pancreatic dysplasia in a mouse model of chronic pancreatitis. 132
In humans, already 1 year after exenatide was inaugurated as novel antidiabetic drug, first case reports pointed to an association between exenatide treatment and acute pancreatitis, 133 and in the following years, numerous further case reports followed, including also other members of this drug class such as liraglutide,128,134–138 which finally led to a safety alert by the FDA (http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm150839.htm). Of note, exenatide is administered to type 2 diabetic patients who are per se on a higher risk of acute pancreatitis.139,140 Regarding the previously mentioned study that includes 30 cases of pancreatitis after exenatide use, 128 in approximately 90% of the individuals also other causes for predisposing pancreatitis were present, as it is already commented elsewhere. 141 Thus, consistent with previous animal studies and case reports, examining the FDA’s database of reported adverse events, an increased risk of pancreatitis with GLP-1–based therapy was noted, and in this study, only type 2 diabetic patients were retrieved, excluding the previously mentioned bias. 137 Further cause for strong concern regarding pancreatitis and pancreatic cancer risk was given by a report on the FDA Adverse Event Reporting System (FDA AERS) database that investigated the association of these adverse effects with antidiabetic drug use, pointing to significantly elevated risk for exenatide and also for the DPPIV inhibitor sitagliptin. 142 The results and the limitations of this study were already accurately summarized elsewhere. 143 Moreover, independently of the FDA report, 11 cases of pancreatic cancer in association with exenatide treatment were reported in the German regulatory database. 144
In contrast to exenatide, liraglutide was very recently reported not to modify the risk of acute pancreatitis or pancreatic cancer when compared in a prospective claims-based assessment of other antidiabetic drugs, suggesting rather an individual effect of exenatide than a drug class effect. 145 This is supported by another study reporting no evidence for pancreatic changes or pancreatitis in three animal species (mice, rats and monkeys) upon treatment with liraglutide for 2 years at exposure levels up to 60 times higher than in humans 146 and in another study using Zucker diabetic fatty (ZDF) rats receiving liraglutide treatment for 13 weeks. 147 But of note, Jeong et al. recently published the results of eight phase-3 clinical trials that compared the safety of liraglutide treatment compared to other monotherapies or combination therapies. This group reported six cases of pancreatitis and five cases of cancer in the liraglutide group and only one case of pancreatitis in the exenatide and the glimepiride group, respectively, and one case of cancer under both metformin and sitagliptin. The small number of positive associations with pancreatitis or pancreatic cancer under liraglutide does not allow a proof of elevated risk, but as commented by the authors, there is a lack of evidence of long-term safety of GLP-1 agonists for the moment. 148
In addition to pancreatitis and pancreatic cancer risk, several previous in vitro and in vivo rodent studies raised concern about involvement of GLP-1 agonists in medullary thyroid cancer, first reported for liraglutide in 2009 based on preclinical toxicological studies in the context of the FDA Advisory Committee review of liraglutide, but in the meantime also for exenatide137,149 (http://www.fda.gov/downloads/AdvisoryCommittees/Committees%20MeetingMaterials/Drugs/EndocrinologicandMetabolicDrugsAdvisoryCommittee/UCM151129.pdf). Of note, GLP-1 receptors are differently expressed in C-cells between rodents and humans. They were mainly found in rat parafollicular thyroid C-cells and to a lesser extent in mice, and finally, humans and cynomolgus monkeys display only very low GLP-1 receptor expression in thyroid C-cells.150,151 This could explain different susceptibilities for GLP-1 agonists among different species provoking calcitonin release, C-cell hyperplasia and finally the transformation to thyroid cancer – GLP-1-mediated effects that have been previously proven in different studies.152–155 While long-term liraglutide administration led to calcitonin release, C-cell hyperplasia and tumour formation in rats and to a lesser extent in mice and C-cell tumours increased after liraglutide administration in a dose-dependent manner in rodents, no calcitonin release in humans or C-cell proliferation in monkeys was detected, revealing species-specific differences in GLP-1 receptor action and of course also receptor distribution in the thyroid. 150
In humans, long-term effects of GLP-1 agonists with regard to thyroid cancer are not unequivocal. The last mentioned study of Bjerre et al. 150 reported no liraglutide-provoked elevation of calcitonin in humans focusing on nine clinical trials of 20–104 weeks of duration. This result was first presented by Hegedüs et al. 156 summarizing the results of eight phase-3 clinical trials [the Liraglutide Effect and Action in Diabetes (LEAD) trials 1–6, two phase-3 trials in Japanese] and one phase-2 trial in non-diabetic subjects. This was also confirmed by the meta-analysis of Alves et al. 157 that included 25 studies evaluating exenatide and liraglutide which were found not to increase the risk of thyroid cancer. In contrast, Elashoff et al. 137 reported, after examining the US FDA’s database of reported adverse effects, a significantly elevated risk of thyroid cancer in patients treated with exenatide compared to rosiglitazone.
Considering that the GLP-1 receptor is broadly distributed in different organs, the question rises whether GLP-1 agonists may also promote cancers other than pancreatic and thyroid cancers. In this regard, the state of knowledge is unfortunately sparse. Very few in vitro data in colon and breast cancers exist, which surprisingly point to a protective role of exenatide inhibiting proliferation and inducing apoptosis of tumour cells.158,159 Considering the lack of GLP-1 receptors in breast cancer cells, GLP-1 may act through other still unidentified mechanisms on the tumour cells. Therefore, much more in vitro, rodent and also human studies are necessary to clarify the potential role and the molecular mechanisms of GLP-1 agonists in these cancer sites.
In 2013, a two-part point-counterpoint narrative was published in Diabetes Care discussing the still open question whether GLP agonist therapies are safe. While Butler et al. 160 pointed out the growing concern about risks of a GLP-1 agonist therapy, for Nauck, 161 the published data did not seem convincing enough to advise against GLP-1 agonist therapies. This point-counterpoint narrative reflects the still equivocal data on GLP-1 agonists with regard to pancreatic and medullary cancer risk accentuating the need for further clinical trials to clarify the safety of these antidiabetic drugs. However, one should be aware of several human studies that could not find any association between GLP-1 agonist use and cancer risk.162–166
In summary, based upon the in vitro, rodent and human studies, the currently available results suggest a reason for concern for the GLP-1 receptor agonists, especially for exenatide, with respect to pancreatitis and pancreatic cancer and furthermore for both receptor agonists with respect to medullary thyroid cancer. However, there are still conflicting data upon this issue, accentuating the need for further long-term prospective clinical studies. The ongoing clinical trial Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER, clinical trial: NCT01179048), a multicentre, randomized, double-blind placebo-controlled study, will surely help to highlight the potential risks of this GLP-1 agonist in the future. Since a potential risk cannot be ruled out for the present and as it was already discussed in numerous comments on this issue, a careful physical examination is thus needed with regard to positive family history for pancreatitis or pancreatic cancer and, accordingly, thyroid cancer before starting a glucose-lowering therapy with GLP-1 receptor agonists. For these patients, other antidiabetic therapies should be considered.
DPPIV inhibitors
Like the incretin-based therapies, DPPIV inhibitors display their mechanism of action in the GLP-1 receptor pathway, leading to an enhanced glucose-stimulated insulin secretion. Oral DPPIV inhibitors prolong the half-life of endogenously secreted GLP-1. 167 Because of their analogous way of acting on GLP-1 levels as the GLP-1 agonists, DPPIV inhibitors might carry similar risk with regard to cancer incidence. On the other hand, DPPIV (CD26) is reported to be a tumour suppressor antigen decreasing melanoma,168,169 prostate, 170 endometrial 171 and ovarial172–174 carcinoma cell metastasis, pointing to a different way of action compared to GLP-1 agonists.
In the meantime, both in vitro and rodent data, as well as numerous human data regarding cancer incidence under DPPIV inhibitor therapy, are available. In different rodent models, DPPIV inhibitors, such as sitagliptin as the first drug of this class approved, were shown to raise the risk of acute pancreatitis. However, in only manageable amount of rats, Matveyenko et al. 175 reported increased pancreatic ductal turnover, ductal metaplasia and, at least in one out of eight rats, pancreatitis in the human islet amyloid polypeptide (HIP rats) transgenic rat model of type 2 diabetes after 12 weeks of sitagliptin treatment. Nachnani et al. 131 found, in 10 Sprague-Dawley rats that were treated with exenatide for 75 days, more pancreatic acinar inflammation and more pyknotic nuclei than in control rats. Based on these rodent results, the question arises whether DPPIV inhibitors also display a negative impact on human pancreatic tissue under normal therapeutical dosage of the drugs, taking into account that in rodent studies the concentration of the used drugs is often higher. In humans, several studies indeed reported similar cancer risk with DPPIV inhibitors compared with placebo or other active drugs. For instance, in a previous report published in 2008 including the results from 12 RCTs, no association between sitagliptin users and non-users could be found after sitagliptin use between 12 and 106 weeks of duration with regard to the incidence of pancreatitis. 176 In a meta-analysis including all RCTs with a duration of at least 24 weeks, no short-term association was found between DPPIV inhibitors and cancer incidence, 177 and in a retrospective cohort study that analysed the data for 786,656 patients, no association was found either between the use of sitagliptin and acute pancreatitis, but there was an increased incidence of acute pancreatitis found in diabetic versus non-diabetic individuals. 162 In a study already mentioned above including 16,276 sitagliptin initiators, risk of pancreatitis was the same when treated with sitagliptin compared to metformin or glyburide, 165 and this was also recently reported in a pooled analysis of 25 clinical studies that included data from 14,611 patients with type 2 diabetes. The authors could not find an association between sitagliptin use and increased risk of pancreatitis or malignancy, but, of note, this work was conducted by the sitagliptin marketing company itself. 178 Very recently, a meta-analysis including 134 RCTs with a duration of more than 12 weeks with the DPPIV inhibitors sitagliptin, vildagliptin, saxagliptin, alogliptin, linagliptin and dutogliptin compared to placebo or active drugs was performed. The authors concluded that DPPIV inhibitors do not elevate the risk of acute pancreatitis in patients with type 2 diabetes, although they mentioned the small number of individuals with acute pancreatitis under therapy and the wide confidence intervals of risk estimates. 179 Further pooled analysis including 20 RCTs enrolling 9156 patients reported no elevated risk of pancreatitis or malignancy with saxagliptin therapy. 180 Moreover, two large clinical trials, ‘Examination of Cardiovascular Outcomes with Alogliptin versus Standard of Care’ (EXAMINE, investigating alogliptin) and ‘Saxagliptin Assessment of Vascular Outcomes Recorded in patients with diabetes mellitus’(SAVOR, investigating saxagliptin), reported no higher incidence of cancer and pancreatitis compared to placebo,181,182 although it has to be mentioned that both trials were set up primarily to study the effects of DPPIV inhibitors on cardiovascular outcomes and not on cancer incidence.
Despite these numerous reports in humans revealing no serious indication of the need for caution, however, there are also a number of case reports and case–control stud-ies that are consistent with animal study results emphasizing an elevated risk of pancreatitis and even pancrea-tic cancer under DPPIV treatment.137,138,183–186 The FDA reported an elevated risk of pancreatitis in patients treated with sitagliptin (http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/ucm183764.htm), and, as already mentioned, it is well known that chronic pancreatitis enhances the risk of pancreatic cancer. 130 Singh et al. 138 identified, among adults with type 2 diabetes in a large administrative database in the United States, 1269 hospitalized cases with pancreatitis, and compared to 1269 well-matched controls, they found an association with sitagliptin use and increased odds of hospitalization due to acute pancreatitis. Elashoff et al. 137 used the FDA AERS database for investigating the association between sitagliptin treatment and adverse effects such as pancreatitis, pancreatic cancer, thyroid or other cancers and reported an increased risk of pancreatitis with sitagliptin, increasing the odds ratio sixfold as compared with other therapies. Recently, a case/non-case study from the French Pharmacovigilance Database was published investigating the use of GLP-1 analogues and DPPIV inhibitors between March 2008 and March 2013 reporting 3109 serious adverse drug reactions, 147 (4.7%) cases of pancreatitis among them. The authors found the usage of all investigated incretin-based drugs (exenatide, liraglutide, sitagliptin, saxagliptin and vildagliptin) to be associated with an elevated risk of pancreatitis. 187 In a recent case report, vildagliptin was reported to induce acute pancreatitis after 5 weeks of therapy, of note, again in a type 2 diabetic woman with per se elevated risk of pancreatitis. 183
The inconsistent results may be explained – as already discussed elsewhere138,188 – by limited statistical power, short duration of follow-up or inadequate adjustment for confounders, such as diabetes severity. Therefore, for the moment, concerns remain regarding a possibly elevated risk of pancreatitis and pancreatic cancer when DPPIV inhibitors are used, which should be considered especially in cases of positive family history of pancreatitis. Further long-term randomized clinical human studies with adequate adjustments and suitable statistical power are needed to clarify the potential risk of DPPIV inhibitors to favour cancer growth.
Insulin-based therapies and cancer risk
In the last years, several publications demonstrated that some cancers are positively associated with elevated endogenous insulin and also higher insulin-like growth factor-1 (IGF-1) levels, and moreover, hyperinsulinaemia and insulin resistance are associated with worse outcomes of various cancers.5,189 The molecular mechanisms are still under ongoing debate. It is well known that the insulin-like growth factor-1 receptor (IGF1R) and the insulin receptor (IR) are homologous receptors. Signalling through the IGF1R, normally mediated by the IGFs, results mainly in mitogenic effects, such as cell growth and proliferation, whereas signalling through the IR mainly exerts metabolic effects playing a role in glucose metabolism, protein synthesis and inhibition of lipolysis. However, both insulin and IGF-1 share metabolic and mitogenic effects. Insulin can also bind to the IGF1R though with lower affinity than IGF-1. Therefore, hyperinsulinaemia may exert mitogenic effects mediated through the IGF1R, but as it was recently demonstrated in mice in vivo using the mitogenic insulin analogue AspB10, the mitogenic effects can also be exerted through the IR itself. 190 In parallel, it was also shown in previous in vitro studies that the IR, predominantly the more mitogenic IR-A isoform, is overexpressed in many types of cancer,191–195 and insulin as well as insulin analogues appears to be able to stimulate the growth of various tumour cells in vitro through IR-A, although the existing data revealed some heterogeneity.196–199
Here, we will focus on insulin analogues in humans trying to clarify the safety concerns raised by the in vitro studies. Most human data are available for insulin glargine, a long-acting insulin analogue first approved in 2000 in the European Union (EU) and in 2003 in the United States. The majority of the reported studies are observational. However, to clarify the role of insulin and insulin analogues in cancer development, prospective RCTs represent the best study design. The ‘Outcome Reduction with an Initial Glargine Intervention’ (ORIGIN) trial, a large RCT published in the New England Journal of Medicine in 2012 which was primarily designed for the investigation of cardiovascular events in 12,537 patients with cardiovascular risk factors receiving insulin glargine or standard care for median 6.2 years, could not confirm any difference between insulin glargine users and the control group with regard to cancers. 200 However, this study has several limitations, as it was commented by Vigneri et al.; 201 among them were the study design that was defined for cardiovascular and not cancer outcomes, the use of metformin which is reported to have beneficial protective effects on cancer, and sulfonylureas as potential cancer promoters, the lack of precise declaration of other medications potentially interfering with cancer, the temporarily or permanently discontinued use of glargine in 62% of the participants, the imprecise declaration of cancer diagnosis, the low dose of glargine and the short observation period. The second RCT investigating cancer incidence was published already in 2009 by Rosenstock et al. 202 This study enrolling 1017 individuals compared insulin glargine with human neutral protamine Hagedorn (NPH) insulin and was primarily designed to clarify differences between both insulins with regard to ocular complications in diabetic individuals for 5 years. No differences in cancer incidence were reported with insulin glargine compared to NPH insulin. This study has also limitations. As already mentioned, it was not designed to investigate cancer incidence. With regard to the size of both compared groups, the incidence of cancer reported was small. In the insulin glargine group (n = 514), 57 all-cancer cases were detected and 62 in the NPH insulin group. Regarding site-specific cancers, only malignant skin neoplasms were found in more than 10 individuals in the glargine group (vs 9 individuals in the NPH insulin group), while regarding all other cancers, the number of cancer cases was less than 10, for example, for breast cancer 3 and 5, respectively.
In line with these two RCTs, three meta-analyses were published, which could not find any association between insulin glargine use and elevated cancer risk. In the study of Home and Lagarenne, 203 31 RCTs and 10,880 individuals were included. Tang et al. 204 included one RCT and 10 observational studies, all together 448,928 individuals, in the analysis. The study from Du et al. 205 reported a meta-analysis from seven cohort studies.
Beyond these RCTs and meta-analyses, a broad panel of observational studies exist that investigated the cancer risk under therapy with mainly insulin glargine but also other types of insulin, most of them suggesting a neutral effect. 206 However, few observational studies point to a higher risk of cancer among insulin users. Hemkens et al. 207 included 127,031 diabetic patients in the study with a mean follow-up of 1.63 years who were treated with human insulin or with one of the three insulin analogues (insulin glargine, insulin lispro and insulin aspart). The authors reported a positive correlation between cancer incidence and insulin dose for all insulin types. Moreover, considering the lower mean daily dose for glargine and after adjusting, an elevated cancer incidence for glargine compared to human insulin was reported, supporting safety concerns on insulin glargine. Of note, however, the overall cancer incidence in the insulin glargine group was significantly lower. In the following months, this study was criticized by different authors to have several limitations, for example, the lack of data on glycaemic control under therapy and the short follow-up period. 208 In the study by Colhoun, 209 insulin glargine was associated with higher risk of both all cancers and also breast cancer compared to individuals receiving other insulins, but interestingly, together with the data from the third subset of patients who used insulin glargine together with other insulins, the overall risk of all cancers or site-specific cancers was not associated with insulin glargine treatment. The authors concluded that the differences noted in the insulin glargine group would reflect allocation bias, and in summary, they did not give reason for serious concern using insulin glargine. The study by Mannucci et al. 210 showed, in 1340 insulin-treated patients during a median follow-up of 75.9 months, an association of the use of insulin glargine with cancer incidence compared to users of human insulin or other analogues. Moreover, the authors found an association between cancer incidence and glargine doses in this study.
In line, another meta-analysis of observational studies from Colmers et al. 211 representing data from 1332,120 individuals compared both the new use of insulin to standard care and the new use of insulin glargine to other insulins. The authors reported an association of the new use of insulin or insulin glargine with an increased risk of pancreatic cancer. Moreover, the new use of insulin glargine was found associated with a decreased risk of colorectal but an increased risk of prostate cancer.
Among the observational studies, indeed, some could not prove an elevated risk of cancer of any type under insulin glargine therapy. However, they gave reason for concern with regard to some site-specific cancers. For instance, Jonasson et al. 212 who included 114,841 patients in the study could not find a significantly elevated risk of all types of cancer [relative risk (RR) of 1.07] for individuals receiving insulin therapy with glargine compared to the usage of other types of insulin, but an elevated risk of breast cancer. However, the authors themselves point to the limitations of the study and mention that the study does not allow conclusion about a causal relationship between insulin glargine use and enhanced cancer risk. In a second observational study, although no elevated risk for insulin glargine users compared to users of human insulin for all cancers could be found, the authors reported an elevated risk of breast cancer under insulin glargine therapy. 213
Taken together, based on the large RCTs and the majority of the meta-analyses, there is no evidence for a causal relationship between glargine and elevated cancer risk. The confidence in the effect estimate is highest for RCTs and lower for observational studies. So, RCTs are the best designed studies to prove a hypothesis. The neutral results of the few RCTs that focused on cancer risk under insulin therapy suggest that insulin therapy, and especially insulin glargine, is safe. However, as discussed above, the two RCTs display also several limitations, and based on in vitro and observational human studies available for the moment, a residual risk cannot be ruled out, in particular with regard to breast cancer. In general, many clinical studies display a too short follow-up time which makes them unfeasible to prove an impact on cancer risk under insulin therapy, considering that cancer initiation, promotion and progression usually need several years to occur. Furthermore, in diabetic patients who display per se elevated risk of cancer because of other factors than hyperinsulinaemia, for example, hyperglycaemia, oxidative stress or different medications, many confounding factors exist, which all have to be taken into account in a properly designed study. Therefore, more large-scale, randomized, well-designed clinical studies with an adequate mean follow-up period are strongly needed to get reliable answers to these safety issues under insulin therapy.
Other antihyperglycaemic therapy regimens and cancer risk
Alpha-glucosidase inhibitors
Alpha-glucosidase inhibitors inhibit the pancreatic α-amylase and intestinal α-glucosidase suppressing glucose absorption by the gastrointestinal tract. The representatives are acarbose, miglitol and voglibose.
In general, only few publications investigating α-glucosidase inhibitors and cancer risk exist. Quesada et al. 214 reported after 14 weeks of treatment with acarbose in APC gene 1309 knockout mice decreased size of gastrointestinal adenomas, providing early evidence for a possible modulatory impact of α-glucosidase inhibitors on colon cancer.
In humans, in a recently published population-based case–control study from the Taiwan National Health Insurance Database enrolling 116 patients with kidney cancer and 464 controls, a significant association between the use of α-glucosidase inhibitors and elevated risk of kidney cancer was found. 215 The study, however, displays several limitations, such as the small number of cases and the lack of adjustment for several covariates, such as smoking and body mass index, but also blood glucose levels and HbA1c. The same investigator group published two further population-based observational studies including 19,624/19,625 cases with newly diagnosed diabetes mellitus and 78,496/78,500 controls reporting the use of α-glucosidase inhibitors to be correlated with decreased lung and gastric cancer risk, respectively.216,217 Moreover, in another population-based study from Taiwan including 39,515 patients with newly diagnosed diabetes and 79,030 controls, the authors reported an association between the use of α-glucosidase inhibitors and lower risk of hepatic cancer. 218 In contrast, in the Barcelona case–control study including 1040 cases with any cancer and 3120 controls based on a cohort of 275,164 type 2 diabetic individuals, no association between the use of α-glucosidase inhibitors and risk of cancer was reported. Of note, in this study, none of the investigated oral antidiabetic drugs including metformin, sulphonylureas, repaglinide, TZDs, DPPIV inhibitors or several insulin types modified the risk of cancer. 123 A further Taiwanese study enrolling 495,199 men and 503,748 women could not find an association between acarbose use and bladder or thyroid cancer.219,220
Taken together, based on the published data, no serious cause for concern exists regarding cancer incidence under α-glucosidase inhibitor therapy. Since these antihyperglycaemic agents have been used for many years in diabetes treatment, it is remarkable that only few reports investigated their possible involvement in cancer. Particularly, with regard to the above-mentioned studies showing a possible involvement of α-glucosidase inhibitor treatment in cancer development, further studies are necessary to better understand these observations.
Sodium Glucose Cotransporter-2 inhibitors
Sodium glucose cotransporter-2 (SGLT-2) inhibitors belong to a novel class of oral antidiabetic drugs. They inhibit the renal glucose reabsorption in the proximal tubule of the nephron, leading to increased glucose excretion. They have only a low risk of hypoglycaemia and reveal the benefit of weight loss. Looking for possible cancer risk under SGLT-2 treatment, we must respect that there are only few reports regarding this issue due to the short availability. Beyond increased risk of genital or urinary tract infections which appears to be a manageable side effect of this drug class, safety concerns arose pointing to an increased risk of bladder and also breast cancer under therapy with dapagliflozin, the first approved SGLT-2 inhibitor. Based primarily on a FDA report, the number of patients who were diagnosed with bladder cancer under dapagliflozin was small: only nine male patients out of 5478 compared to one out of 3156 controls on placebo developed bladder cancer. The rate of cancer, however, was found elevated, as only two cases were expected in the control group (http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/EndocrinologicandMetabolicDrugsAdvisoryCommittee/UCM262994.pdf). In the same FDA report, nine cases of breast cancer were identified compared to only one woman in the control group. Thus, the FDA considered numeric imbalances in breast and bladder cancer cases. In another FDA report, no association between renal, bladder and breast cancers was found with canagliflozin usage (FDA Briefing Document NDA 204042). In summary, based upon the considerations of the FDA, potential safety concerns cannot be ruled out for the moment, which could be only cleared up by long-term clinical trials.
Conclusion and future perspectives
Today, the correlation between type 2 diabetes and elevated cancer risk, at least with regard to several site-specific cancers, appears generally allocated and widely accepted. However, type 2 diabetes is a multifactorial disease with many accompanying confounding factors, such as obesity, hyperinsulinaemia, hyperglycaemia, hyperlipidaemia, increased oxidative stress and also inflammation, which could themselves have an impact as risk factors on initiation, promotion or progression of cancer. Especially, hyperinsulinaemia is suggested to be a causal factor for the association between diabetes and cancer.
Although many epidemiological studies exist that investigated the possible associations between type 2 diabetes medications and cancer risk, by now several important questions remain unanswered, and this is mainly due to the lack of large, randomized, prospective and accurately for this special purpose–designed studies. Strongest data exist on metformin, which seems to have protective functions both on monotherapy and also when combined with other oral antidiabetic drugs and insulins in several site-specific cancers. Some reason for concern remains regarding sulphonylureas and also the incretin-based therapies regarding pancreas and thyroid cancers and the SGLT-2 inhibitors as well as pioglitazone regarding bladder cancer (Figure 1). However, as mentioned above, more large-scale, randomized, well-designed clinical studies with especially longer follow-up time period are needed to get reliable answers to these safety questions.
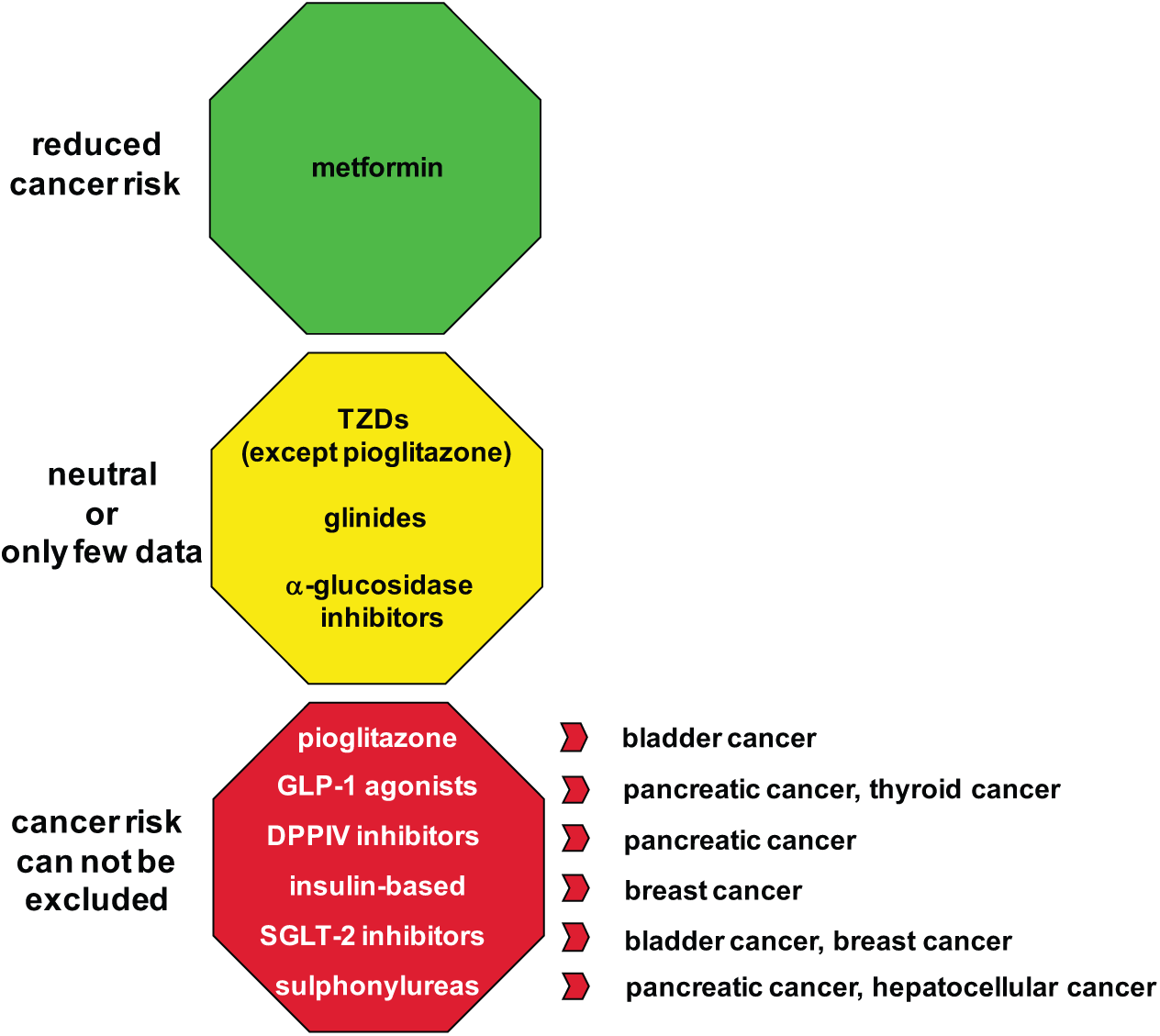
Proposed effects of antidiabetic therapies on cancer risk.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.