
Abstract
Diabetes is associated with increased cardiovascular risk. We have recently shown that the naturally occurring flavonol quercetin (Que) or the synthetic flavonol 3′,4′-dihydroxyflavonol (DiOHF) inhibits platelet function and delays thrombus formation in healthy mice. Therefore, the aim of this study was to investigate the effect of Que or DiOHF treatment on platelet function and ferric chloride–induced carotid artery thrombosis in a mouse model of type 1 diabetes. Diabetic mice treated with Que or DiOHF maintained blood flow at a significantly higher level than untreated diabetic mice at the end of the recording period. In addition, treatment with Que or DiOHF significantly reduced diabetes-induced platelet hyper-aggregability in response to platelet agonist stimulation. Furthermore, treatment with Que or DiOHF significantly inhibited dense, but not alpha, granule exocytosis in diabetic and control mice. Our demonstration that flavonols delay thrombus formation in diabetes suggests a potential clinical role for these compounds in anti-platelet therapy.
Introduction
Diabetes is a growing health problem, and it has been estimated that the number of people with diabetes will rise to 439 million by 2030 worldwide. 1 In Australia, approximately 4.4% of the total population has been diagnosed with diabetes. In addition to its high prevalence, diabetes costs Australians in excess of AUD $6 billion per year.2,3 Hyperglycaemia is often associated with macro-vascular complications, 4 presenting as accelerated atherosclerosis leading to coronary, cerebral and peripheral arterial disease. Diabetes is therefore an important independent risk factor for cardiovascular disease (CVD) and a major contributor to cardiovascular events, particularly in Western countries. The incidence of CVD is between 2 and 4 §§times greater in people with diabetes, 5 and people with diabetes have a poorer prognosis.6 –8 Indeed, recent reports from the World Health Organization (WHO) state that 50% of diabetic patients will die from CVD. 9 Thrombotic complications of CVD, such as myocardial infarction (MI) and stroke, are responsible for up to 84% of deaths in people with diabetes aged 65 years and older.5,10 In Australia, it was reported that 65% of all CVD deaths occur in people with diabetes or impaired glucose metabolism. 11 Therefore, it is vital to develop new treatments to reduce diabetes-induced CVD.
Antithrombotic agents are regularly used for the secondary prevention of cardiovascular events in diabetic patients and in primary prevention of high-risk individuals, 12 but there are growing data to suggest inadequate cardiovascular protection by these agents. 13 Over the last decade, many naturally occurring food components have been investigated for their health benefits, particularly, in reducing diabetes-induced complications. 14 Flavonols are one of the most common food-derived polyphenolic compounds, which are associated with beneficial effects on the vasculature. 15
The Rotterdam study showed a reduction in the occurrence of MI with increased flavonol intake. 16 Furthermore, previous studies have shown that ingestion of flavonol-rich foods and beverages reduce platelet aggregation.17–20 Quercetin (Que) is ubiquitously found in a variety of fruits and vegetables and is one of the most abundant naturally occurring flavonols. 21 It has been reported in animal models of diabetes that treatment with Que restores endothelial function 22 and reduces pancreatic β-cell injury, 23 systolic blood pressure, plasma lipids and plasma glucose levels.24,25 3′,4′-Dihydroxyflavonol (DiOHF) also has demonstrated ability to prevent diabetes-induced endothelial dysfunction, 26 increase nitric oxide activity 27 and to acutely restore endothelium-dependent relaxation in both type 1 and type 2 diabetes. 28
We have recently shown that Que and DiOHF, a synthetic flavonol of similar structure to Que, inhibit human platelet aggregation and dense granule exocytosis in a concentration-dependent manner. 29 Furthermore, we showed that the administration of Que or DiOHF at 6 mg/kg for seven consecutive days inhibits platelet function and reduces thrombus formation in a mouse model of platelet-mediated arterial thrombosis. 30
Therefore, the aim of this study was to investigate the effects of Que or DiOHF on in vivo arterial thrombus formation in animal models with diabetes and study the effects on platelet function ex vivo.
Materials and methods
Animals
Age- and sex-matched C57BL/6 mice were used in this study. Mice were given free access to food and water. All experimental procedures performed in this study were approved by the Animal Experimentation Ethics Committee of RMIT University and were conducted in accordance with the guidelines of the National Health and Medical Research Council of Australia for the care and use of animals for scientific purposes, Animal Ethics Committee number 1136.
Induction of diabetes and administration of investigational agents
Diabetes was induced according to previously described methods31,32 with minor modifications. Briefly, diabetes was developed in C57BL/6 mice (n = 32) following a series of five intraperitoneal (i.p.) injections with streptozotocin (STZ; 60 mg/kg) dissolved in citrate buffer. Diabetes was confirmed when the blood glucose level was >13 mmol/L. Mice that did not develop diabetes within 4 days of the last STZ injection were given a second series of five STZ injections. Where blood glucose exceeded >30 mmol/L and insulin was administered at 0.1–0.2 U/mouse i.p. 2–3 times a week. Control mice (n = 32) received an equal amount of citrate buffer alone. Following 8 weeks of STZ-induced diabetes or an equivalent control period, mice were randomised to receive Que (6 mg/kg), DiOHF (6 mg/kg) or vehicle [0.5% (v/v) dimethyl sulphoxide (DMSO) plus 20% (w/v) polyethylene glycol (PEG) and saline], via i.p. injection daily for 7 days. Experimental procedures and blood collection were performed 24 h following the last treatment.
Ferric chloride–induced carotid injury
In a subset of mice (n = 24), ferric chloride–induced arterial injury was performed as previously described. 30 Briefly, mice were anaesthetised with ketamine and xylazine (200:10 mg/kg) by i.p. injection. A midline cervical incision was made and the carotid artery exposed. A laser Doppler flow probe (Moor Instruments, Axminster, UK) was placed adjacent to the carotid artery to measure baseline blood flow. After baseline blood flow was established, a 2 × 4 mm2 filter paper saturated with 20% (w/v) ferric chloride was applied to the carotid artery on the adventitial surface of the carotid artery for 4 min. Following the removal of the filter paper, blood flow through the carotid artery was monitored for 30 min or until 95% reduction in blood flow was reached. At the end of each experiment and while the mouse was under deep anaesthesia, it was euthanized by cervical dislocation.
Sample preparation for platelet aggregation and dense granule exocytosis
In a separate subset of mice (n = 40), fresh whole blood was collected via cardiac puncture and placed into tubes containing 100 µL of 3.2% (w/v) sodium citrate. Platelet-rich plasma (PRP) was obtained by centrifugation at 200 × g for 15 min at room temperature with no brake. Platelet poor plasma (PPP) was obtained by centrifugation of the remaining blood at 1200 × g for 15 min at room temperature. Platelet count was performed using a Beckman Coulter Ac · T 5diff Haematology Analyser (Brea, CA, USA). Platelet count was normalised in all treatment groups to 100 × 109 L−1 in Ringer’s citrate dextrose (RCD) buffer, pH 7.4 (108 mM NaCl, 38 mM KCl, 1.7 mM NaHCO3, 21.2 mM sodium citrate, 27.8 mM glucose and 1.1 mM MgCl2·6 H2O, with pH adjusted to 7.4).
Platelet aggregation
Platelet aggregation was measured by turbidimetric aggregometry using a Chrono-log 700 aggregometer (Chrono-log Corp., Havertown, PA, USA). 30 In brief, PRP aggregation was performed in the presence of 100 µg/mL fibrinogen and 1 mM CaCl2 at 37°C with constant stirring (1000 r/min). Platelet aggregation baseline was set against murine PPP diluted 1:2 in RCD buffer pH 7.4. Platelet aggregation was stimulated using 250 µM of the protease-activated receptor 4 (PAR 4) agonist peptide H-Ala-Tyr-Pro-Gly-Lys-Phe-NH2 (AYPGKF-NH2) (GL chemicals, China).29,33 The maximal aggregation amplitude over a 9-min period was recorded.
Assessment of granule exocytosis
Flow cytometric analysis was performed using a FACSCanto II flow cytometer (BD Pharmingen, San Jose, CA, USA) with excitation at 488 nm. Dense granule exocytosis was measured by flow cytometry using fluorescent quinacrine uptake and AYPGKF-NH2-induced release as previously described. 30 The percentage decrease in fluorescence intensity following stimulation is a measure of thrombin-induced dense granule exocytosis.33,34 Aliquots of mouse PRP were incubated with 100 µM quinacrine at 37°C for 20 min in the dark. The platelets were then washed using RCD buffer pH 6.5 by centrifugation at 500 × g for 10 min with no brake at room temperature and resuspended in RCD buffer pH 6.5. Aliquots were incubated with 250 µM AYPGKF-NH2 at 37°C for 5 min in the dark. The reaction was stopped by 1:12 dilution of RCD buffer pH 7.4 and immediately analysed by flow cytometry. Percentage of decrease in [488] 530/30 nm mean fluorescence intensity (MFI) relative to unstimulated platelets was recorded.
P-selectin (CD62P) is a component of the alpha granule of platelets which is expressed on the surface membrane only after fusion of the alpha and plasma membranes during alpha granule exocytosis. Alpha granule exocytosis can therefore be measured by platelet surface CD62P expression.34,35 Alpha granule exocytosis was measured in separate aliquots of PRP by incubating with 1:50 anti-mouse CD62P-PE (BD Pharmingen) and 250 µM AYPGKF-NH2 at 37°C for 30 min. [488] 585/42 nm MFI, corresponding to CD62P-PE, was recorded.
Statistical analysis
All values are expressed as mean ± standard error of the mean (SEM). Comparisons between test samples and control were performed using one-way analysis of variance (ANOVA) test with Dunnett’s test, for post hoc comparisons. An unpaired Student’s t-test was performed to compare diabetic and non-diabetic platelet aggregation and dense granule exocytosis. Two-way ANOVA test with Bonferroni’s test, for post hoc comparisons, was performed to compare body weight and random plasma glucose in diabetic and non-diabetic mice. All statistical analysis was performed using GraphPad Prism (version 5).
Results
Body weight and plasma glucose levels
Over the 8-week period, the STZ-treated mice gained less weight compared to non-diabetic control (Figure 1(a)). Similarly, the random blood glucose levels in STZ-treated mice were significantly higher than in non-diabetic mice (Figure 1(b)).
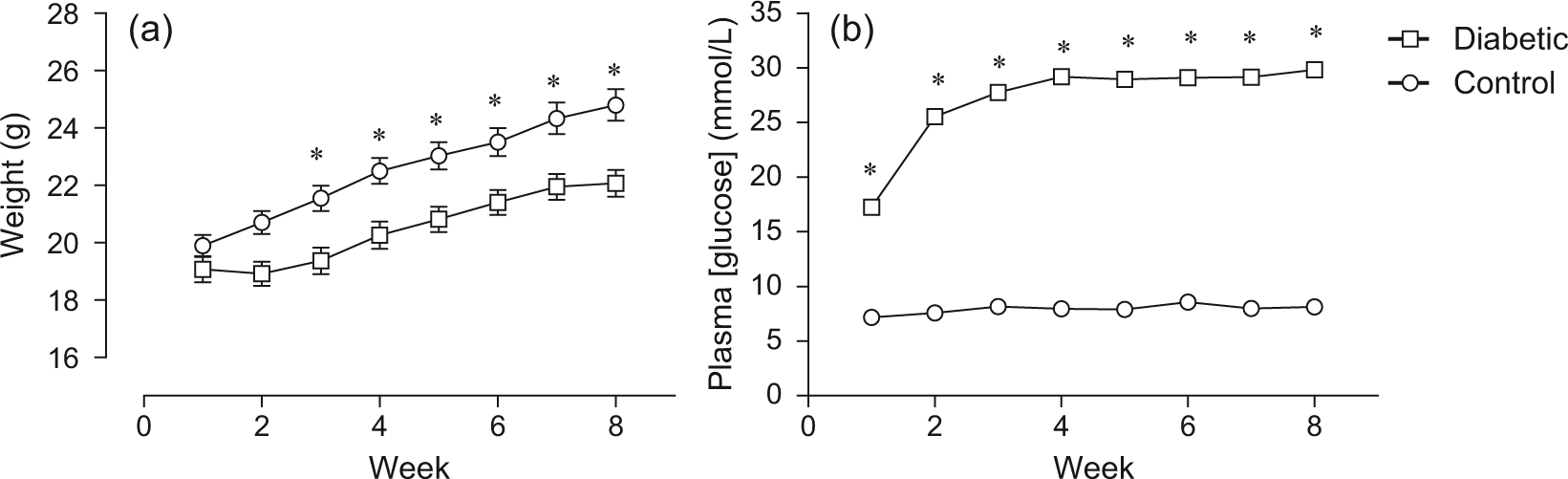
STZ-induced diabetes in C57BL/6 mice: (a) weight of diabetic and non-diabetic mice over the 8-week period and (b) random plasma glucose levels of diabetic and non-diabetic mice during the 8-week period (n = 32 for each group).
Effect of Que and DiOHF on FeCl3-induced arterial thrombosis
Diabetic mice showed rapid thrombus formation when compared to the non-diabetic mice. In vehicle-treated diabetic mice, carotid blood flow was reduced to 50% ± 17% of baseline 5 min after the removal of FeCl3 (Figure 2), while vehicle-treated control mice maintained greater than 90% blood flow (94% ± 7% flow, p < 0.05 vs diabetic vehicle-treated mice, Figure 2). However, at 15 min after the removal of FeCl3, both diabetic and non-diabetic vehicle-treated mice had near-complete vessel occlusion (5% ± 1% flow vs 6% ± 1% flow, respectively, Figure 2). There was no blood flow at 30 min as there was complete occlusion for both vehicle-treated diabetic and non-diabetic mice.
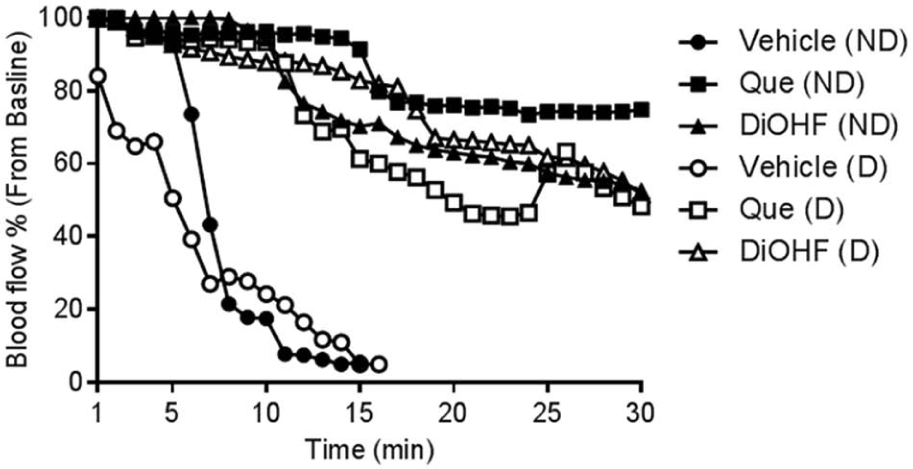
Mean carotid blood flow in diabetic and control mice treated with 6 mg/kg Que, 6 mg/kg DiOHF or vehicle control after the removal of FeCl3 (n = 4 for each treatment group). For clarity, results are shown as the mean only, without SEM.
Treatment of diabetic mice with 6 mg/kg of Que or DiOHF significantly improved blood flow in the carotid artery at 5 min (Que 94% ± 5% flow, DiOHF 93% ± 7% flow, p < 0.05 vs diabetic vehicle-treated mice, Figure 2). At 15 min, flavonol-treated diabetic mice maintained significant blood flow (Que 61% ± 15% flow, DiOHF 83% ± 18% flow, p < 0.05 vs diabetic vehicle-treated mice, Figure 2). Similarly, blood flow at 15 min was well maintained in non-diabetic mice treated with 6 mg/kg of either Que or DiOHF (Que 91% ± 6% flow, DiOHF 70% ± 18% flow, p < 0.05 vs non-diabetic vehicle-treated mice, Figure 2). Blood flow at 30 min after FeCl3 injury was well maintained in diabetic mice treated with the flavonols (Que 48% ± 21% flow, DiOHF 52% ± 19% flow, Figure 2). When non-diabetic mice were treated with the flavonols, both Que and DiOHF maintained blood flow at 30 min after FeCl3 injury. When blood flow in both diabetic and non-diabetic mice was expressed as the area under the curve, flavonol-treated mice showed significantly greater blood flow than vehicle-treated diabetic and non-diabetic mice (Figure 3).
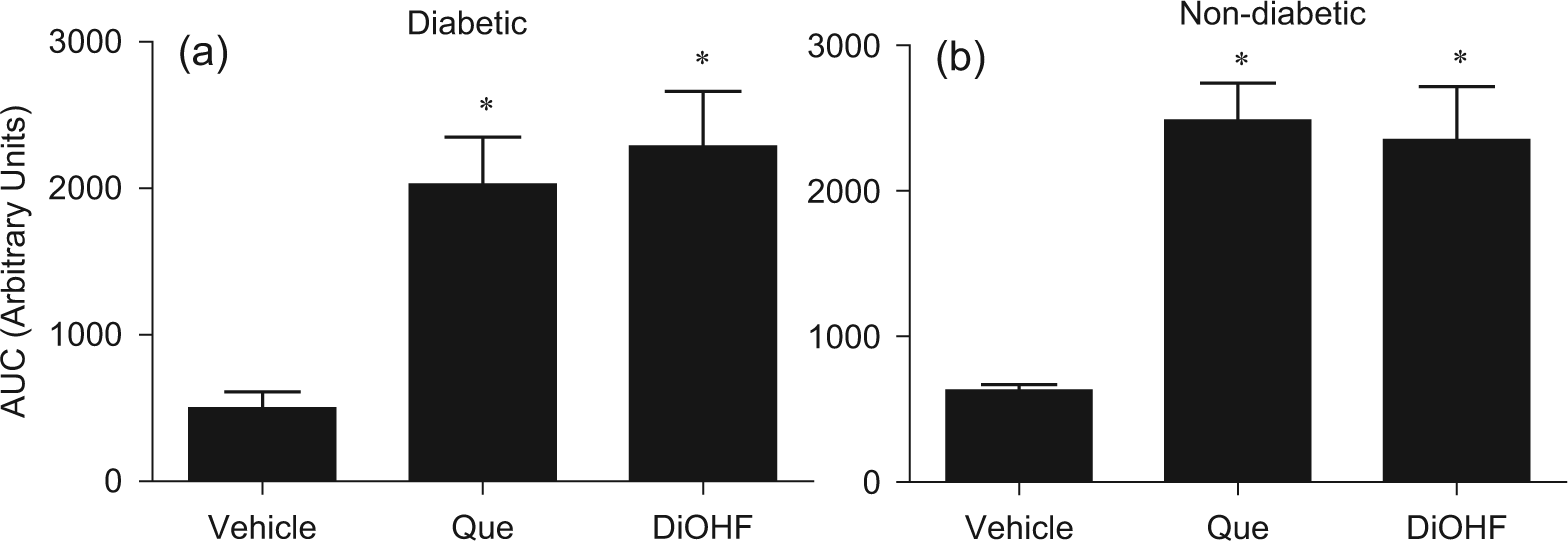
Carotid artery blood flow expressed as the AUC over 30 min for the mice treated with 6 mg/kg Que, 6 mg/kg DiOHF or vehicle control following ferric chloride–induced arterial injury: (a) diabetic mice and (b) non-diabetic mice.
Effect of Que and DiOHF on platelet aggregation
Platelets derived from diabetic mice showed a higher level of aggregation to AYPGKF-NH2 stimulation when compared to the vehicle-treated control mice (102% ± 9% diabetic platelets vs 78% ± 2% control platelets, p < 0.05). Platelet hyper-aggregability in diabetic mice was significantly reduced following 7-day treatment with Que or DiOHF (Que 64% ± 7% and DiOHF 70% ± 9%, p < 0.05 vs vehicle, Figure 4(a)). In control mice, Que or DiOHF treatments, as expected, significantly reduced platelet aggregation (Que 53% ± 6% and DiOHF 53% ± 10%, p < 0.05 vs vehicle, Figure 4(b)).
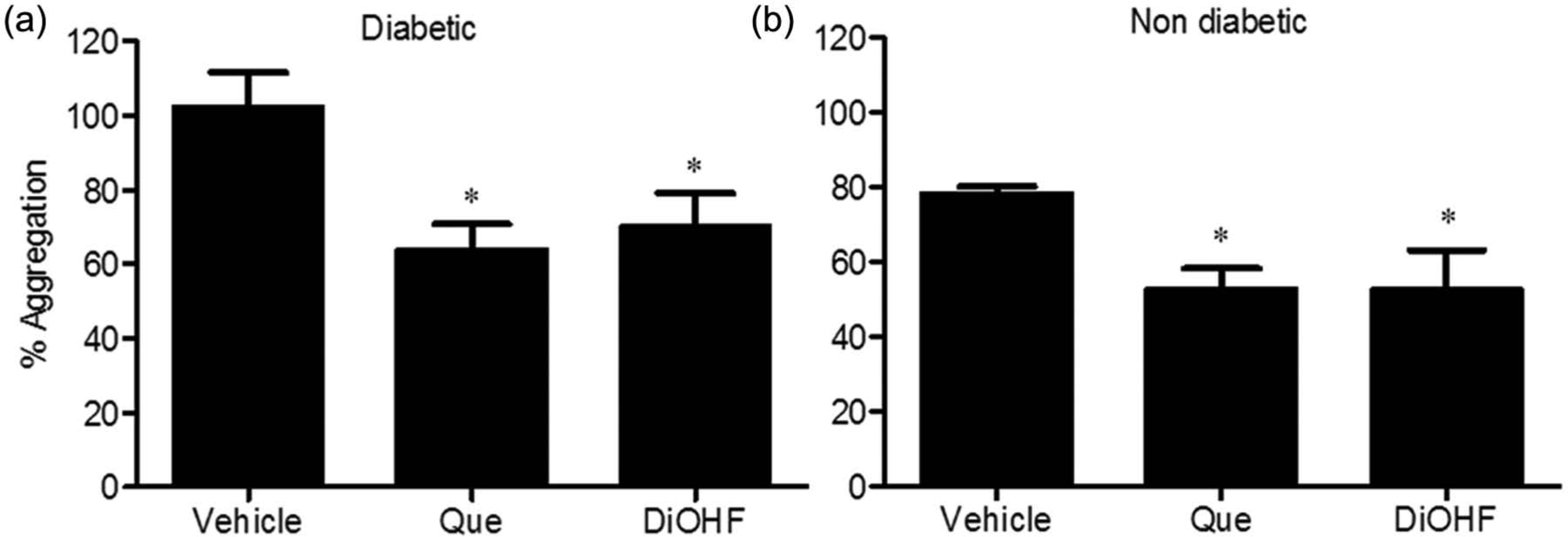
Platelet aggregation stimulated with AYPGKF-NH2 (250 µM). Platelets were obtained from diabetic and non-diabetic mice treated with 6 mg/kg Que (n = 5), DiOHF (n = 5) or vehicle (n = 4). Platelet count was normalised to 100 × 109 L−1 in all test groups: (a) diabetic mice and (b) non-diabetic mice.
Effect of Que and DiOHF on granule exocytosis
There was no significant difference in AYPGKF-NH2-induced dense granule exocytosis, as measured by quinacrine release, between vehicle-treated diabetic and non-diabetic mice (51% ± 4% vs 58% ± 3%, p > 0.05). Treatment with 6 mg/kg of Que or DiOHF significantly inhibited dense granule exocytosis in diabetic (Que 34% ± 4% and DiOHF 34% ± 3%, p < 0.05 vs vehicle, Figure 5(a)) and non-diabetic mice (Que 48% ± 3% and DiOHF 46% ± 2%, p < 0.05 vs vehicle, Figure 5(b)).
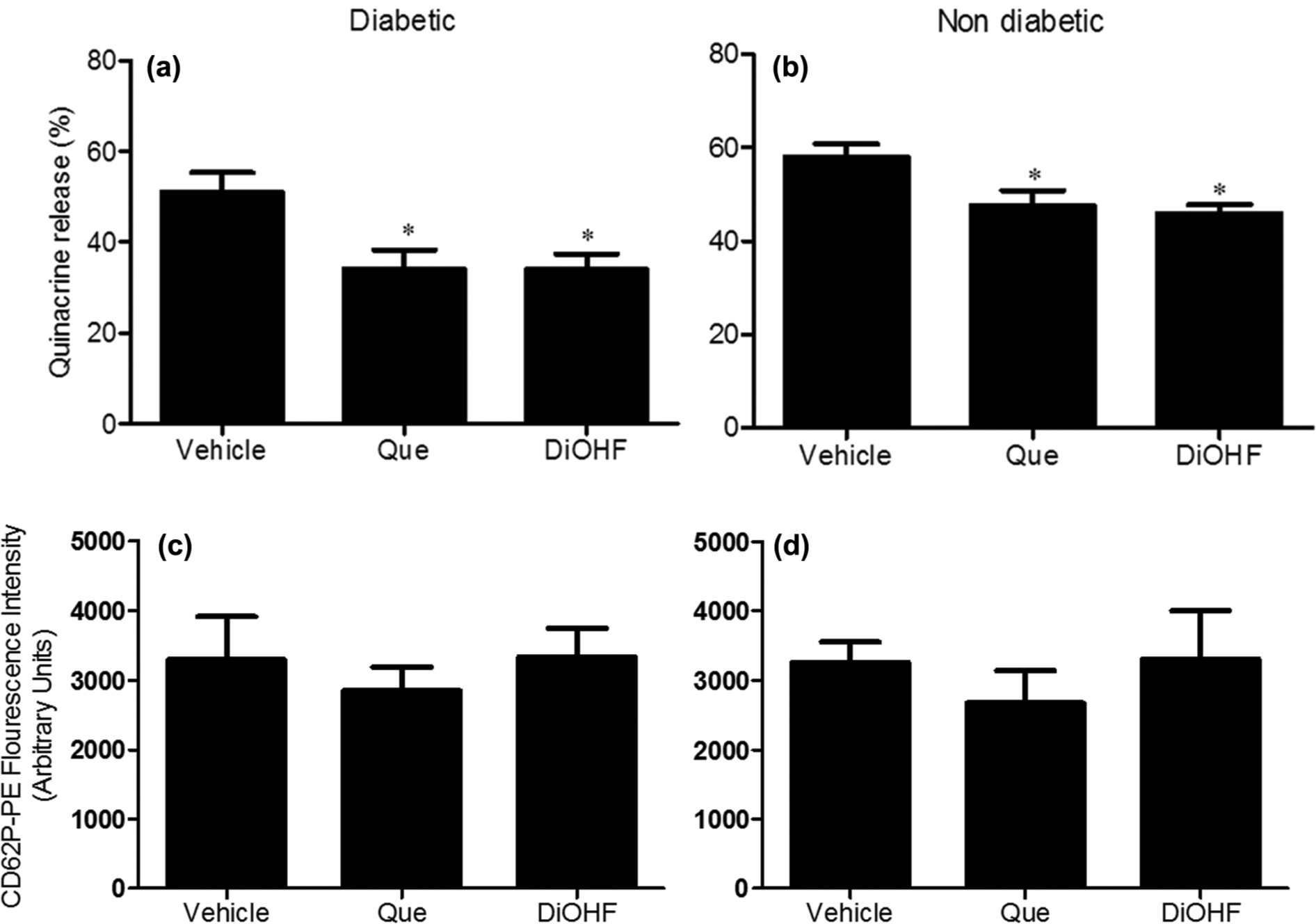
Granule exocytosis stimulated with AYPGKF-NH2 (250 µM). Platelets were obtained from diabetic and non-diabetic mice treated with 6 mg/kg Que (n = 6), DiOHF (n = 6) or vehicle (n = 6). Platelet count was normalised to 100 × 109 L−1 in all test groups. (a) Dense granule exocytosis as measured by quinacrine release in diabetic mice. (b) Dense granule exocytosis as measured by quinacrine release in non-diabetic mice. (c) Alpha granule exocytosis as measured by P-selectin expression in diabetic mice. (d) Alpha granule exocytosis as measured by P-selectin expression in non-diabetic mice.
There was no significant difference in AYPGKF-NH2-induced alpha granule exocytosis, as measured by platelet membrane P-selectin expression, between vehicle-treated diabetic and non-diabetic mice (3296 ± 619 vs 3257 ± 297 MFI, p > 0.05). Treatment with 6 mg/kg of Que or DiOHF had no impact on alpha granule exocytosis in either diabetic (Que 2850 ± 334 fluorescence intensity and DiOHF 3328 ± 420 MFI vs vehicle 3296 ± 619 fluorescence intensity, p > 0.05, Figure 5(c)) or non-diabetic mice (Que 2671 ± 463 fluorescence intensity and DiOHF 3306 ± 694 fluorescence intensity vs vehicle 3257 ± 297 fluorescence intensity, p > 0.05, Figure 5(d)).
Discussion
In this study, we have shown that i.p. treatment with Que or DiOHF for seven consecutive days delays thrombus formation in a model of platelet-mediated thrombosis in type 1 diabetic mice. Furthermore, we show that the delay in thrombus formation is at least in part due to the inhibition of platelet aggregation and dense granule exocytosis.
Platelet hyper-sensitivity plays a major role in cardiovascular complications of diabetes.36,37 Therefore, the aim of the study was to investigate the effects of Que and DiOHF on platelet function and thrombus formation. In this study, STZ was used to induce type 1 diabetes in C57BL/6 mice. FeCl3 was used to induce arterial thrombosis in the carotid artery. FeCl3 induces platelet-mediated thrombus formation by damaging the endothelial lining, causing RBC haemolysis and haemoglobin oxidation. This leads to reactive oxygen species (ROS) production, causing further endothelial damage, resulting in increased platelet activation and adhesion at the site of injury. 38
Diabetic mice showed rapid thrombus formation when compared to healthy mice. Indeed, thrombus formation in diabetic mice commenced prior to the removal of the FeCl3 strip, and when the FeCl3 strip was removed, blood flow had fallen below the baseline. In contrast, non-diabetic mice maintained 100% blood flow during and after FeCl3 application. Furthermore, at 5 min after FeCl3 removal, blood flow in diabetic mice was less than 50% of baseline, while blood flow in control mice was close to pre-injury levels. This supports previous observations that in mice, hyperglycaemia accelerates thrombus formation when induced by FeCl3. 39 This suggests that diabetes accelerates thrombus formation, but there is no difference in the magnitude of thrombus formation over 30 min. It is well established that impairment of endothelial function is associated with diabetes and is likely to contribute to the accelerated thrombus generation in diabetics. This may be due to the reduced production of NO 40 and other vasorelaxant and antithrombotic agents such as prostacyclin from the endothelial cells, in addition to the enhanced platelet aggregation associated with this disease state.
Treatment with 6 mg/kg of either Que or DiOHF significantly improved blood flow and delayed thrombus formation in diabetic mice. Indeed, blood flow in flavonol-treated diabetic mice was maintained to near 100% flow 5 min after FeCl3 removal, and there was no significant difference in blood flow between diabetic and non-diabetic mice. In addition, full vessel occlusion did not occur even 30 min after FeCl3 injury.
In our diabetic model, platelets were found to be hyper-aggregable in response to AYPGKF-NH2 when compared to non-diabetic mice. This observation is in agreement with previous observations that diabetic animals show enhanced platelet aggregation41–43 and also corresponds with the rapid formation of a platelet-mediated thrombus in vivo. In contrast, alpha and dense granule exocytosis was not significantly different between diabetic and non-diabetic mice. Treatment with 6 mg/kg of Que or DiOHF for seven consecutive days significantly reduced platelet aggregation and inhibited dense, but not alpha, granule exocytosis in response to AYPGKF-NH2. This is consistent with our previous observations in healthy mice. 30 In this study, we demonstrate a greater than 30% inhibition of platelet aggregation in diabetic mice, eliminating the hyper-aggregability in this condition and resulting in levels similar to that of the non-diabetic mice.
Although the delay in thrombus formation observed in this study corresponds to the reduction of platelet aggregation and dense granule exocytosis, it is likely that the previously described effects of these flavonols on endothelial function also contributed to the overall vascular benefits achieved. Que and DiOHF have been reported to produce potent vasoprotective effects on both healthy and diabetic models. Que has also been demonstrated to exert beneficial vascular effects in a range of pathological conditions including diabetes.44–46 Indeed, it has been shown to restore endothelial relaxation in diabetes in response to acetylcholine, increase NO, neutralise free radicals and reduce oxidative damage in STZ-treated rats.22,47,48 Que has also been reported to inhibit lipid peroxidation via inhibition of xanthine oxidase. 49
This study demonstrates that 6 mg/kg of the flavonols is capable of delaying thrombus formation in diabetes, which is consistent with our previous studies26
–28 which reported that daily i.p. treatments of 6 mg/kg of flavonols for 7 days reduced
Limitations
This study demonstrates that the flavonols Que and DiOHF improved blood flow and reduced platelet aggregation in an animal model of type 1 diabetes. It is unclear whether similar effects take place in animal models of insulin resistance and type 2 diabetes, which remains an area for future research. Furthermore, the optimal dose range and the effect of these flavonols on platelet function induced by different agonists should also be determined. Although DiOHF perhaps appeared to be more effective than Que in diabetic mice, such a comparison requires the use of further doses of each agent. Finally, reduced platelet aggregation might be associated with increased bleeding risks, and although significant bleeding was not observed, appropriate studies investigating the effect of these flavonols on bleeding times are warranted.
Footnotes
Acknowledgements
The authors wish to gratefully acknowledge Mr Musaed Alshahrani for his help with the animal model. Flow cytometry was performed at the RMIT University Flow Cytometry Core Facility.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.