
Abstract
Objective:
We analysed the association between serum potassium, within the normal range, and early signs of diabetes in an Israeli population.
Research design and methods:
A computerized database of the Clalit Health Services was used for obtaining information regarding patients’ baseline serum potassium levels. The main study outcome was dysglycaemia, defined as fasting glucose > 100 mg/dL, HbA1C > 6.5 gr% (48 mmol/mol) or a new diagnosis of diabetes. A secondary outcome was overt diabetes.
Results:
Included in the study were 71,597 patients, mean age 40.8 ± 13.4 years. After a mean follow-up period of 5.3 ± 2.2 years, dysglycaemia decreased [odds ratio (OR) = 0.95; 95% confidence interval (CI) = 0.906–0.997; p = 0.038], as did the incidence of overt diabetes (OR = 0.86; 95% CI = 0.793–0.934; p = 0.0001), for every 1 mmol/L elevation in serum potassium in the normal range. But analysis of subpopulation reveals that when elevated serum potassium was associated with low adjusted ORs for predicting dysglycaemia (OR = 0.904 with a 95% CI of 0.849–0.963; p = 0.002), the opposite effect was demonstrated over the age of 41 years (OR = 1.113 with a 95% CI of 1.048–1.104; p < 0.001).
Conclusions:
This study demonstrates age-related association between serum potassium and the risk of dysglycaemia.
Background
An association between low serum potassium and the development of type 2 diabetes has been the subject of extensive research for more than five decades. Early evidence emerged in the 1960s demonstrating aggravation of pre-existent type 2 diabetes mellitus in patients treated with thiazide diuretics. 1 Since then, the adverse metabolic effects of thiazide diuretics have been demonstrated in a number of randomized controlled trials.2,3 The precise aetiology is not clear, although most evidence points to low serum potassium as the common thread, showing a positive correlation between thiazide-induced hypokalaemia and the incidence of type 2 diabetes, most probably via the inhibitory effect of low potassium on insulin secretion.4,5 Oral potassium supplementation has been shown to reduce thiazide-induced hypokalaemia and possibly reverse glucose intolerance. 2 Angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs), unlike diuretic drugs, were found, by some6–8 but not all of the trials, 9 to be associated with decreased risk of type 2 diabetes mellitus. The possibility arises that in contrast to diuretics, ACE inhibitors decrease the risk of type 2 diabetes by elevating serum potassium levels. However, a recent trial on valsartan was not able to demonstrate a protective effect of serum potassium on type 2 diabetes risk. 10
Low serum potassium levels, even within the normal range, have been found to be associated with higher incidence of type 2 diabetes in populations of Americans, 11 healthy Japanese males 12 and hypertensive Germans. 13 Serum potassium levels per se, as well as the relationship between serum potassium and the incidence of type 2 diabetes, may be affected by a number of factors, such as environment, ethnicity, lifestyle and dietary habits. Genetic factors, such as those influencing the renin and aldosterone synthesis, may also have an effect.
Information regarding the relationship between serum potassium and the incidence of type 2 diabetes in a Mediterranean population consuming high potassium diet is limited. The aim of this study was to investigate the possible relationship between serum potassium levels and impaired fasting glucose (FG), as well as with the development of type 2 diabetes, in a Mediterranean population of Israeli patients receiving no medications known to interfere with either potassium levels or the risk of type 2 diabetes.
Methods
The study was carried out in the central district of Clalit Health Services (CHS), the largest Managed Care Organization (MCO) in Israel. CHS provides medical care to about 450,000 patients residing in this district, which is mainly urban in nature. CHS has introduced computerized medical files containing all demographic, clinical and laboratory data of the patients since 1998. We conducted a large retrospective cohort study of individuals who underwent at least one ambulatory serum potassium test during the period of 1 January 2002 until 31 December 2005. Patient outcomes were followed to 31 December 2010. The CHS computerized database was used to identify the patients’ baseline characteristics and outcomes.
Study inclusion criteria were age 18–80 years and the presence of baseline data on serum potassium levels at the start of the study period. Exclusion criteria were diagnosed type 1 or type 2 diabetes mellitus; HbA1C > 5.7 gr% (39 mmol/mol); FG > 5.5 mmol/L; a prescription for diuretics, ACE inhibitors, ARBs or aldospirone at any time before the first potassium lab result; congestive heart failure; estimated glomerular filtration rate (eGFR) less than 60 mL/min [as calculated by the Modification of Diet in Renal Disease (MDRD) formula]; and a prescription for steroids for 3 months or more prior to the first potassium level result.
We also extracted data about age, gender, body mass index (BMI), drug consumption and other baseline laboratory tests. The main outcome was dysglycaemia, defined as impaired FG or type 2 diabetes, and assessed by one, or more, of the following conditions: FG > 5.5 mmol/L, HbA1C > 6.5 gr% (48 mmol/mol) and diagnosis of type 2 diabetes by a physician. A second outcome was overt type 2 diabetes mellitus, defined as FG > 7 mmol/L, HbA1C > 6.5 gr% (48 mmol/mol) or diagnosis of type 2 diabetes by a physician.
Each individual was followed until 31 December 2010, irrespective of the date of inclusion. The study was approved by the CHS local Institutional Review Board.
Statistical analysis
Mean [± standard deviation (SD)] values were calculated for continuous variables; categorical variables were expressed in frequencies. Serum potassium was categorized into four groups within the normal range: 3.5–4.0, 4.0–4.5, 4.5–5.0 and 5.0–5.5 (mmol/L). To compare the means of continuous variables measured between these groups, one-way analysis of variance (ANOVA) was used. Categorical data were compared among these groups by χ2 tests. We used Pearson’s correlation coefficient r for analyses of associations between continuous variables. Multivariate linear regression analysis was performed to obtain partial (adjusted) correlations.
Associations of incident dysglycaemia and type 2 diabetes with continuous or categorical variables were analysed using the univariate logistic regression model. Continuous or categorical variables that correlated or tended to correlate to the risk of the incidence of type 2 diabetes were further analysed using multiple logistic regression models. The odds ratio (OR) and 95% confidence intervals (CIs) were calculated to summarize the effects of each variable.
The cut-offs for the most accurate discrimination of newly diagnosed dysglycaemia for serum potassium and age were derived using standard receiver operating characteristic (ROC) curves. The interaction analysis between serum potassium and age for predicting incidence of dysglycaemia was investigated by logistic regression by simultaneously including into the multiple regression models serum K, age and K × age. To further explore the association between serum K and incidence of dysglycaemia, serum K was modelled by a restricted cubic spline with knots at the 5th, 35th, 65th and 95th percentiles. This method allows to examine nonlinear associations as continuous predictors of incidence of dysglycaemia as an alternative to inappropriate linearity assumptions. 14
All statistical tests were two-sided with a value of p < 0.05 considered significant. All statistical analyses were performed using SPSS software (version 16.0; SPSS Inc., Chicago, IL, USA).
Results
On January 2002, CHS central district provided medical care to 458,916 patients, 71,597 of whom were eligible for the study (Figure 1). The baseline characteristics of the study cohort were as follows: mean age 40.8 ± 13.4 years (18–80 years), 56% females, mean BMI 26.3 ± 5.3 kg/m2 and mean serum potassium 4.35 ± 0.42 mmol/L (Table 1). Missing data for baseline variables were as follows: BMI 10.6%, hypertension (HTN) 2.05%, smoking 7.04%, Na 0.13%, creatinine 0.93% and uric acid 18.7%. Table 1 presents demographic and clinical characteristics of the cohort according to serum potassium concentrations. During the follow-up period of mean 5.3 ± 2.2 years, 29,354 individuals (41.0%) developed dysglycaemia. Of them, 29,100 had FG > 5.5 mmol/L, 146 had HbA1C > 6.5% (48 mmol/mol) and 225 were diagnosed by their family physician as having type 2 diabetes mellitus. Of our cohort, 7% (5012) developed overt type 2 diabetes during the study period; of them, 4976 had a FG test that was greater than 7 mmol/L.
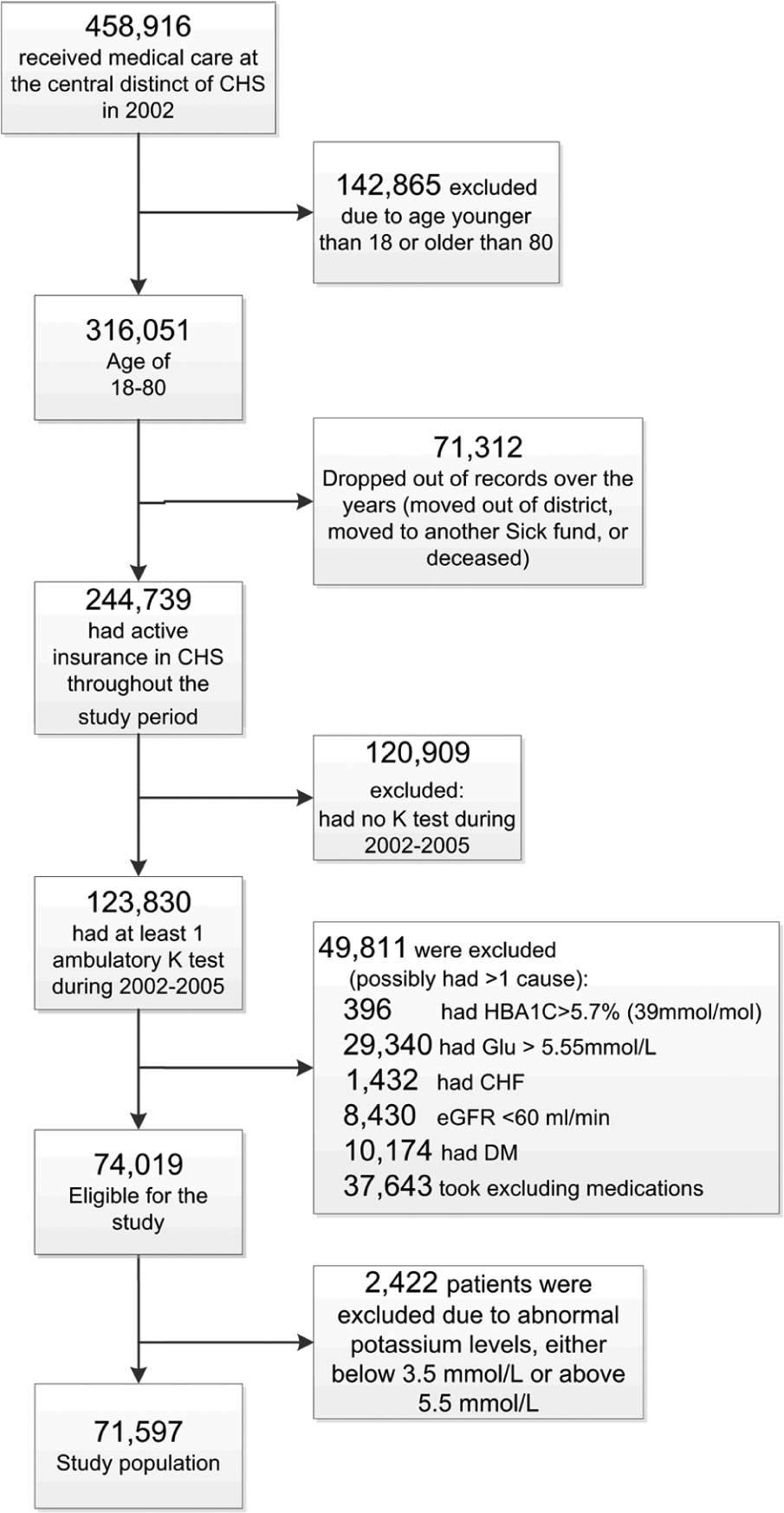
Research population.
Baseline characteristics of the study population according to serum K levels (n = 71,597).
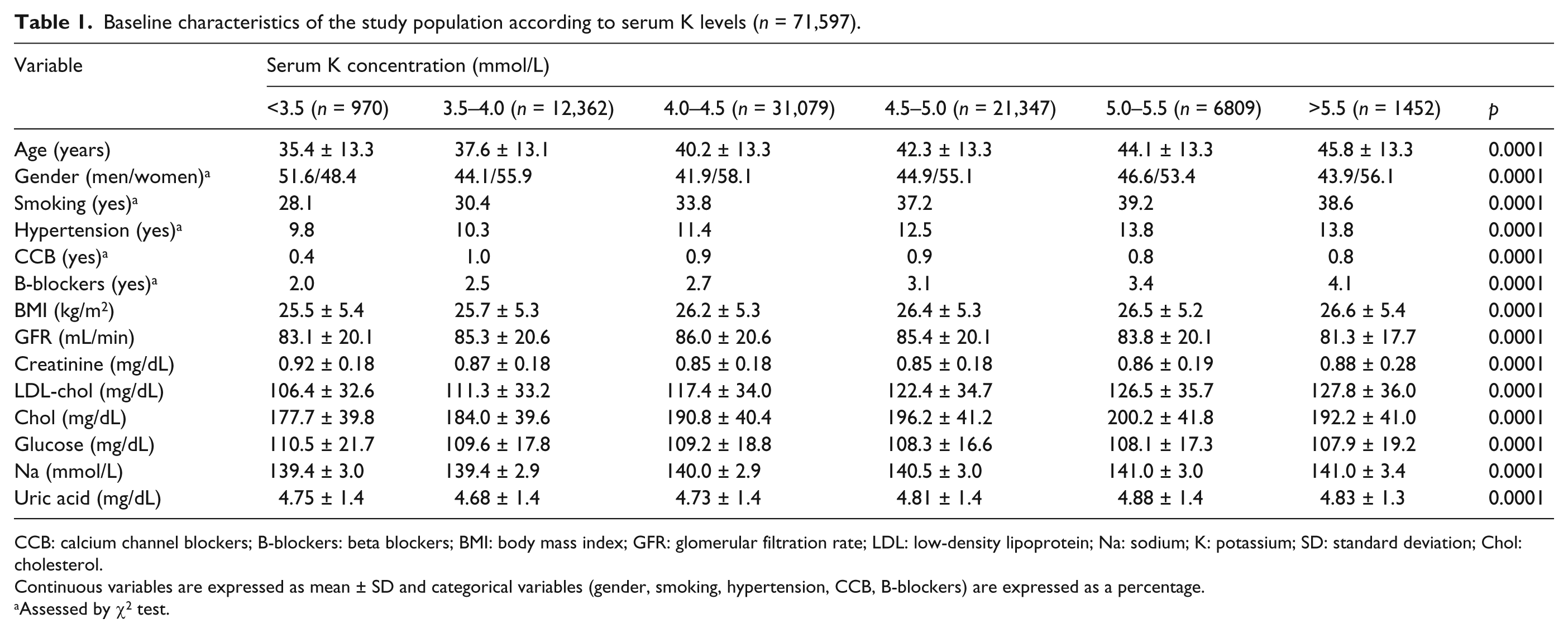
CCB: calcium channel blockers; B-blockers: beta blockers; BMI: body mass index; GFR: glomerular filtration rate; LDL: low-density lipoprotein; Na: sodium; K: potassium; SD: standard deviation; Chol: cholesterol.
Continuous variables are expressed as mean ± SD and categorical variables (gender, smoking, hypertension, CCB, B-blockers) are expressed as a percentage.
Assessed by χ2 test.
Logistic regression analysis revealed a strong positive association between baseline serum potassium and newly diagnosed dysglycaemia; the OR was 1.17 (the 95% CI = 1.129–1.212; p = 0.0001) for every 1 mmol/L increase in serum potassium. However, after adjustment for age, gender, BMI, HTN, smoking status and baseline levels of low-density lipoprotein (LDL) and total cholesterol, creatinine, sodium and uric acid, there was an inversion of this positive association, and the adjusted OR was 0.950 (the 95% CI = 0.906–0.997; p = 0.038) for every 1 mmol/L increase in serum potassium. For overt type 2 diabetes, logistic regression revealed an OR of 0.920 (the 95% CI = 0.861–0.984; p = 0.015) and adjusted OR of 0.861 (the 95% CI = 0.793–0.934; p = 0.001). The incidence of dysglycaemia correlated positively with age, gender, BMI, HTN, smoking, cholesterol and uric acid and negatively with GFR and blood sodium level (Table 2).
Independent risk factors for incidence of combined outcome (dysglycaemia and diabetes) by logistic regression analysis.
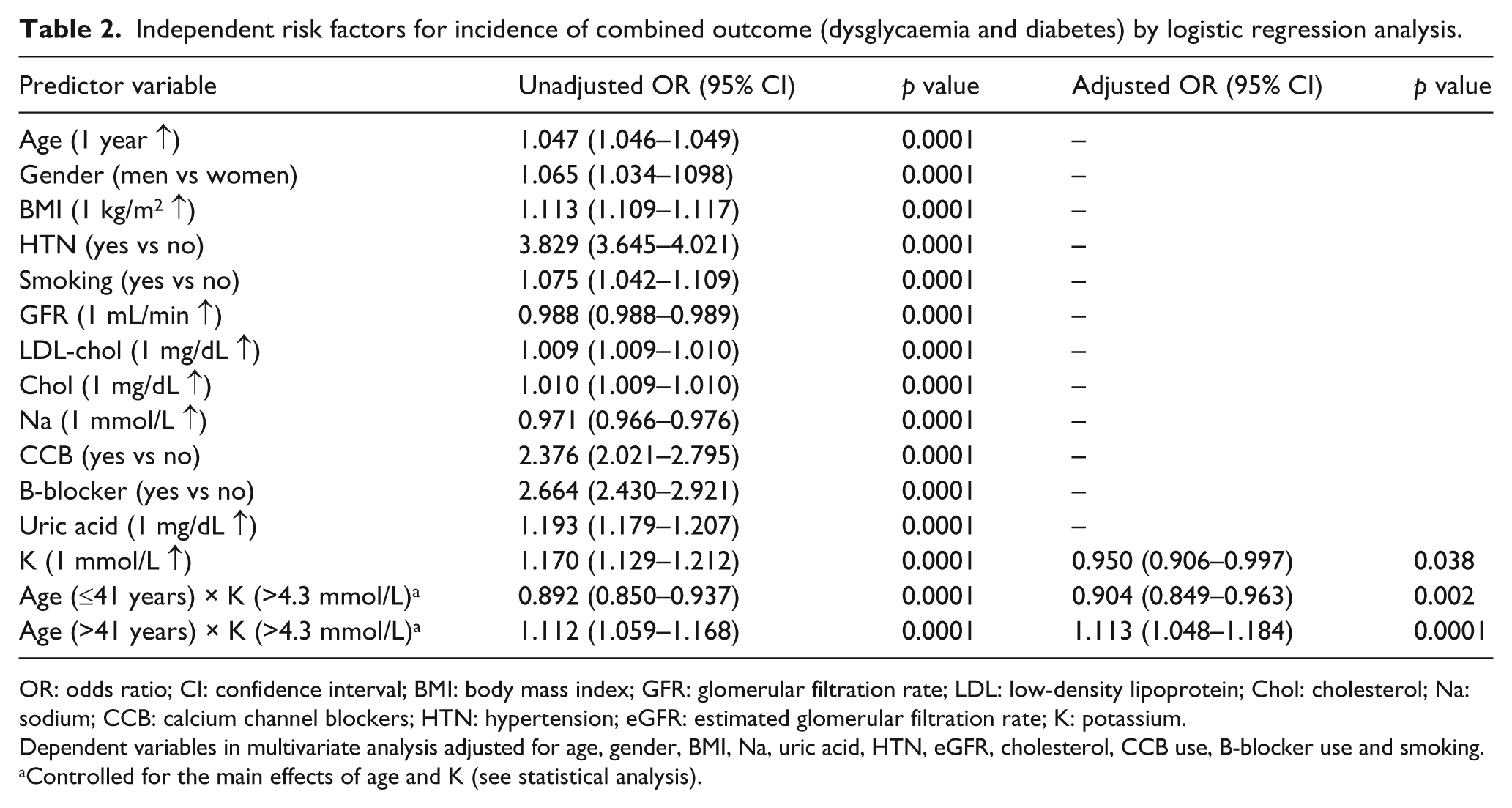
OR: odds ratio; CI: confidence interval; BMI: body mass index; GFR: glomerular filtration rate; LDL: low-density lipoprotein; Chol: cholesterol; Na: sodium; CCB: calcium channel blockers; HTN: hypertension; eGFR: estimated glomerular filtration rate; K: potassium.
Dependent variables in multivariate analysis adjusted for age, gender, BMI, Na, uric acid, HTN, eGFR, cholesterol, CCB use, B-blocker use and smoking.
Controlled for the main effects of age and K (see statistical analysis).
Potential confounders of the association between serum potassium and dysglycaemia were analysed separately. Statistical analysis revealed positive correlation between serum potassium and age, BMI, male gender, smoking, HTN, cholesterol blood level and uric acid (Table 1). Thus, we hypothesized that these confounders could mask the association between blood potassium and the development of dysglycaemia. And indeed, before adjustment, the correlation between serum potassium and the incidence of dysglycaemia seemed positive. A major confounding effect was demonstrated for age, as adjustment for age even as a single confounder was responsible for shift from positive correlation to a negative one with OR of 0.941 (the 95% CI within 0.907–0.978 range; p = 0.002), while after adjustment for all other parameters but age, positive correlation persisted with OR of 1.054 (the 95% CI with 1.005–1.104 range; p = 0.029).
In order to find out what were the mechanisms underlying such a significant confounding effect of age on the association between serum potassium and the study outcome, we separately analysed the relationship between potassium and age. We found a statistically significant linear association between the two variables, in both univariate and multivariate analyses (with β = 0.150 and p = 0.001, and β = 0.097 and p = 0.001, respectively). Patients with lower potassium levels were found to be significantly younger than their counterparts with higher blood potassium (Table 1).
The ROC curves allowed us to define a cut-off value for serum potassium (4.3 mmol/L) with a sensitivity of 58% and specificity of 51% [area under the curve (AUC) = 0.518 (95% CI = 0.514–0.522); p < 0.001] and for age (41 years) with sensitivity of 64% and specificity of 62% [AUC = 0.672 (95% CI = 0.668–0.676); p < 0.001] in predicting of incidence of dysglycaemia. Furthermore, we have studied the prognostic value of serum potassium in the two age-stratified groups of the study participants: the patients older versus younger than 41 years. A statistically significant interaction emerged between age and high-normal level of serum potassium (more than 4.3 mmol/L) in patients with younger age (below 41 years): crude and adjusted ORs for predicting of newly diagnosed dysglycaemia for the product termed K × age were 0.892 with a 95% CI of 0.850–0.957 (p < 0.001) and 0.904 with a 95% CI of 0.849–0.963 (p = 0.002), respectively (Table 2). Interaction analysis between age and high-normal levels of K showed the opposite effect in predicting ORs of incidence of newly diagnosed dysglycaemia in patients over the age of 41 years (Table 2): crude and adjusted ORs for the product termed K × age were 1.112 with a 95% CI of 1.059–1.168 (p < 0.001) and 1.113 with a 95% CI of 1.048–1.104 (p < 0.001), respectively. Figure 2 shows the cubic splines illustrating the associations between serum K and incidence of dysglycaemia in our population. Decreased incidence of dysglycaemia was demonstrated in younger patients (under the age of 41 years) with high-normal serum K levels after multivariate adjustments (Figure 2(a)), whereas the trajectory was reversed in older patient group (age over 41 years) (Figure 2(b)).
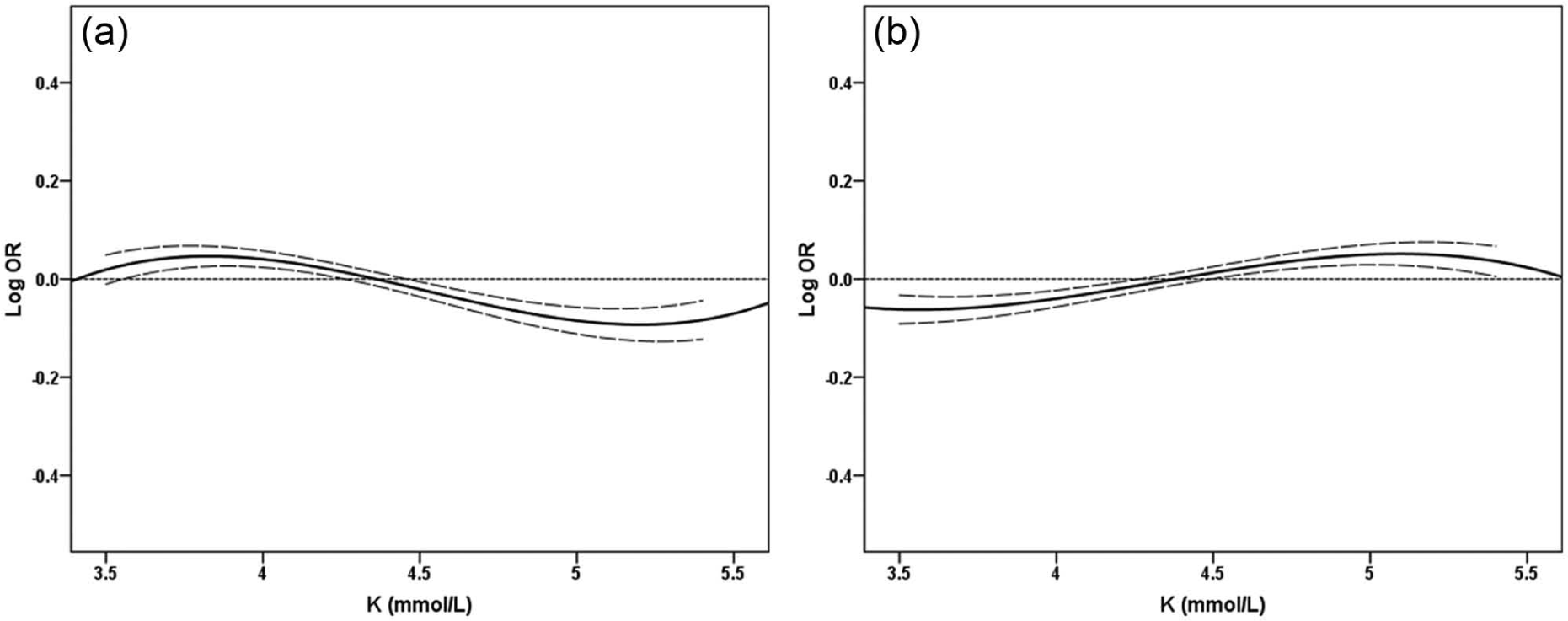
(a) Multivariable-adjusted spline curves of incidence of dysglycaemia in younger population (under the age of 41 years), presented as log ORs (solid lines) and 95% CI (dashed lines) associated with baseline levels of serum potassium in logistic regression models. (b) Multivariable-adjusted spline curves of incidence of dysglycaemia in older population (age over 41 years), presented as log ORs (solid lines) and 95% CI (dashed lines) associated with baseline levels of serum potassium in logistic regression models. The models are plotted as restricted cubic splines with four knots. Multivariable models were adjusted for age, gender, BMI, HTN, smoking status and baseline levels of LDL and total cholesterol, creatinine, sodium and uric acid.
Discussion
This study demonstrated an association between serum potassium, within the normal range, and the incidence of dysglycaemia or overt type 2 diabetes in a large Israeli cohort. The finding of inverse association between serum potassium and the incidence of diabetes concurs with previous studies performed on American, Japanese and German populations.11–13 The aetiology of the relationship between low serum potassium and the development of type 2 diabetes has not been fully elucidated. A decrease in serum potassium has been shown to mediate thiazide-induced type 2 diabetes, 3 but more recent studies have shown that low serum potassium predicts the incidence of type 2 diabetes also in patients who do not consume diuretics. The Atherosclerosis Risk in Communities (ARIC) investigation shows an inverse association between serum potassium and the risk of developing type 2 diabetes in a cohort of American patients. 11 Similar to our investigation, the Cooperative Health Research in the Region of Augsburg (KORA)-F4 study focused on early signs of type 2 diabetes, in a population of European adults. 13 They reported serum potassium to be independently associated with pre-diabetes and newly diagnosed type 2 diabetes in hypertensive adults, albeit no such correlation within the non-hypertensive population. Our results were obtained on a large community-based cohort of 71,597 Israeli adults, 12% were hypertensive at baseline. This low rate of HTN is consequent to the exclusion from this study of individuals consuming ACE inhibitors, ARBs and diuretics.
The inverse association between serum potassium and the risk of dysglycaemia was only demonstrated in patients younger than 41 years, while no such relationship was demonstrated in patients older than 41 years. Thus, the interaction between potassium and age as contributors for the development of dysglycaemia and the positive correlation between age and potassium blood level are another major findings in our study.
The link existing between serum potassium and age was either unnoticed or disregarded in most clinical trials. In ARIC study performed on a cohort aged 45–65 years, the age range was apparently too narrow for observing the association between age and serum potassium. By contrast, in the Japanese cohort of 6640 males, 12 with a fairly broad age range of 25–74 years, elevation in serum potassium levels was, indeed, found to be associated with the advancing age.
The reasons for such an interaction between age and serum potassium are not yet clear. Serum potassium concentrations are a collective result of a wide range of genetic and environmental factors. Potassium intake is one of the factors that affect potassium blood level. It strongly depends on the subject’s habits, ethnicity, diet and so on. Survey data from the Third National Health and Nutrition Examination Survey (NHANES III, United States) estimated the median intake of potassium of the American population. 15 This survey demonstrated that irrespective of the sex of the participants, their mean potassium consumption increases with age up to the age group of 31–50 years. Thereafter, following the age of 50 years, the daily potassium consumption gradually and significantly decreases. An Israeli survey 16 showed similar pattern in Israeli men up to the age of 60 years and in Israeli women up to the age of 50 years. Thus, some of the association between potassium blood level and age may be attributed to potassium intake in the young, and as demonstrated in the Coronary Artery Risk Development in Young Adults (CARDIA) study, 17 low potassium intake may serve as a risk factor for the development of diabetes. Different parameters, such as decrease in aldosterone level 18 and age-associated deterioration of renal function, 19 may govern potassium blood level in patients older than 41 years.
The mean serum potassium level observed in this study was the same as that in the ARIC study, 4.4 mmol/L. 11 Furthermore, the mean BMI was essentially the same: 26 kg/m2 in the current cohort, compared to 27 kg/m2 in the ARIC cohort. 11 Nevertheless, though we have no nutritional data specific to the current cohort, the diet, which is typically consumed in Israel, is rich in potassium compared to the American or European diet. The last Israel survey by the Center for Disease Control 16 reveals estimated intake of 57–64 mmol potassium per day, similar to estimated daily potassium consumption in other Mediterranean countries such as Spain, Portugal and Naples (Italy) (66, 68 and 60 mmol, respectively) and different from its estimated consumption in the United States and Canada (23–52 and 43 mmol, respectively) as described in the INTERSALT trial. 20 The incidence rates of dysglycaemia and overt type 2 diabetes were 41% and 7%, respectively, over an average follow-up period of 5.3 years. The 1.3% annual incidence of type 2 diabetes is the same as that of the entire adult population registered in the CHS database. While the incidence of dysglycaemia in this study seems very high, the rate reflects the low cut-off (FG of 5.5 mmol/L) that was selected. The aim was to diagnose the first signs of the outcome, thus ensuring that potassium blood level would be analysed as a risk factor and not as an early sign of type 2 diabetes. As expected, the mean FG level was low, 6.15 mmol/L. One should remember that although patients are routinely instructed to take blood glucose level in a fasting state, we cannot make sure that in this retrospective study, all of the blood tests were indeed taken in a fasting state, a fact that might also contribute to some increase in the incidence of dysglycaemia.
The high incidence of dysglycaemia also reflects the fact that this study only included individuals who underwent blood tests. They all visited their family physician and were referred for blood tests. Almost 50% of the potential population did not undergo blood tests during the recruitment period; they may have been healthier, with a lower prevalence of dysglycaemia, type 2 diabetes or other diseases. In addition, more of them were male, reflected by the 44% proportion of men in the study cohort. While the slightly greater proportion of women than men in the adult Israeli population 21 may explain some of this difference, the higher proportion of women than men who visit physicians 22 apparently has greater influence. Thus, selection bias is a limitation of this study. Although selection bias was consequent to the retrospective study design, the study cohort is representative of the population at risk, a population that tends to do more blood tests. The identification of serum potassium as a new risk factor for the development of type 2 diabetes in this population is of major importance.
In conclusion, this study better characterizes the association between serum potassium, in the normal range, and new diagnoses of type 2 diabetes in a large community-based Israeli cohort. Opposite association in patients under and over 41 years may reflect different pathophysiologic relationship. When low serum potassium may serve as an independent predictor of type 2 diabetes in the young, the ageing kidney and decreased aldosterone level among other parameters may influence the relationship in the older population.
Footnotes
Acknowledgements
Dr Doenyas-Barak was responsible for the general design, for data and results analysis and interpretation and for the preparation of the manuscript. Dr Beberashvili was responsible for the statistical analysis and for review of the manuscript, and Prof. Vinker was responsible for database collection and for review of the manuscript. Dr Doenyas-Barak is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of conflicting interests
No potential conflicts of interest relevant to this article were reported for any of the authors.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.