
Abstract

Introduction
Prevalence of diabetes and impaired glucose tolerance (IGT) is rapidly increasing, and the World Health Organization (WHO) estimates a current worldwide prevalence of 346 million patients with diabetes mellitus (DM). 1 The International Diabetes Federation’s global estimates for 2011 suggest that 52 million Europeans aged 20–79 years have diabetes and this number will increase to over 64 million by 2030. 2 This alarming trend implies a vertiginous increase in health-care costs, as confirmed by an average expenditure of 75 billion Euros in 2011, which will increase to 90 billion by 2030. Among the constellation of diabetes-related co-morbidities, cardiovascular disease (CVD) carries the largest burden for DM patients. 3 Population-based studies showed that almost 50% of the total mortality in people with DM is due to CVD, while other DM-related complications accounts only for 15%. 3 In a recent meta-analysis of 29 clinical trials that included at least 1000 patients with DM, two factors were noted to identify a higher risk cohort within the diabetic population: the presence of CVD and the presence of proteinuria. 4 CVD increased the rate of all-cause death nearly threefold and the rate of CV death nearly fivefold in subjects with DM. Such epidemiological analyses support the notion that DM and heart disease represent a common and serious combination. There is a strong biological relation between hyperglycaemia, insulin resistance and vascular disease. 5 In patients with DM, high glucose levels trigger endothelial inflammation, mitochondrial oxidative stress and impaired availability of nitric oxide, a key guarantor of vascular health. This leads to the development of coronary atherosclerotic lesions as well as microvascular dysfunction, leading to nephropathy and retinopathy. 5 More importantly, the detrimental effects of glucose already occur with glycaemic levels below the threshold for the diagnosis of DM. This is explained by the concept of ‘glycaemic continuum’ across the spectrum of pre-diabetes, diabetes and CV risk. 6 Early dysglycaemia caused by obesity-related insulin resistance or impaired insulin secretion is responsible for functional and structural alterations of the vessel wall culminating in diabetic vascular complications. 5 In this perspective, rapid and effective interventions are in high demand to fight DM-related CVD burden over the next decades.
The new ESC/EASD guidelines
The need to raise awareness about diabetes and its consequences on cardiovascular health led to the design of ad hoc guidelines by the European Society of Cardiology (ESC), in collaboration with the European Association for the Study of Diabetes (EASD). 7 This document, published in 2007, provided for the first time a systematic approach to diagnose and treat the combination of DM and CVD. 7 The evidence-based strategy promoted by ESC/EASD guidelines led to a consistent improvement in CV outcome in DM subjects, thus strengthening the importance of appropriate diagnostic and therapeutic algorithms to achieve the best care for patients in an individualized setting. The 2007 guidelines have been now updated in 2013, and the new ESC/EASD document has been released on 30 August and published simultaneously with the ESC Congress, held in Amsterdam. 8
The high number of clinical trials as well as basic and clinical science articles over the last 5 years makes it timely and necessary to update the previous guidelines. The emphasis of these guidelines is to provide information on the current state of the art in how to prevent and manage the diverse problems associated with the effects of diabetes on the heart and the vasculature in a holistic manner.
Diagnosis of diabetes
The first issue addressed by the new guidelines is the identification of DM subjects. Type 2 DM (T2DM) is a silent disease, and half of the 552 million individuals with diabetes in 2013 will be unaware of their diagnosis. Moreover, another 300 million individuals show early features of altered glucose homeostasis, leading to a future risk of developing T2DM. Despite advances in diagnosis and treatment, the guidelines state that we are still far from the identification of a reliable hyperglycaemic marker for the detection of DM. Glycated haemoglobin (HbA1c) has been now introduced as a diagnostic test in combination with fasting plasma glucose (FPG). HbA1c is indeed a simple marker that accurately reflects a condition of chronic hyperglycaemia or altered glucose homeostasis. However, there remain concerns regarding its sensitivity in predicting DM. The main clinical question is ‘can we rule out diabetes in patients with a normal HbA1c?’ In the absence of coronary artery disease (CAD), the new guidelines suggest that a negative HbA1c may exclude diabetes in low-risk patients but not in high-risk patients. In this latter group, oral glucose tolerance test (OGTT) should be considered. However, it remains unclear how global cardiovascular risk affects alterations of glucose homeostasis. Moreover, most of our patients are considered at ‘intermediate CV risk’, and the advantages of using OGTT when HbA1c is normal remain elusive. In this regard, the FINnish Diabetes Risk Score (FINDRISK) may guide diagnostic approaches in non-diabetic patients. FINDRISK, which includes age, anthropometric parameters, medication use and history of previous hyperglycaemia, is available in almost all European countries and predicts diabetes with 85% accuracy. In the general population and in people with assumed glucose abnormalities (based on history), a FINDRISK score > 11 may help clinicians to select people suitable for an appropriate screening including HbA1c and eventually OGTT. Despite these concerns, the new guidelines deserve the credit to have simplified the diagnosis of diabetes by introducing HbA1c. On the other hand, OGTT remains a key diagnostic step to unmask subtle diabetes in patients with and without CAD and has important prognostic implications. 8 This relies on the data from important international surveys, clearly demonstrating that dysglycaemia is more common than normoglycaemia in CVD patients admitted to hospital 9 and that the OGTT was able to detect glucometabolic alterations in 55%–60% of patients with overt CVD. 9 Early detection of glucose perturbations by OGTT in patients with CAD offers an opportunity to prevent the development of DM by means of lifestyle programmes and or by pharmacological agents such as metformin, acarbose and rosiglitazone. 9 Moreover, it allows the initiation of glucose-lowering therapy in patients with newly detected DM at an early phase of the disorder. The Euro Heart Survey on Diabetes and the Heart 10 reported that early institution of glucose-lowering therapy is beneficial in patients with CAD and newly detected T2DM. Figure 1 shows a putative algorithm for diagnosis and management of CAD in asymptomatic patients with DM and vice versa. The estimation of long-term risk of developing DM also encourages lifestyle modifications, which remain a milestone for the maintenance of insulin sensitivity and glucose homeostasis (class I, level A). In this regard, seven recent prospective studies have shown that lifestyle counselling (diet plus physical activity) significantly prevents diabetes occurrence during follow-up. 8
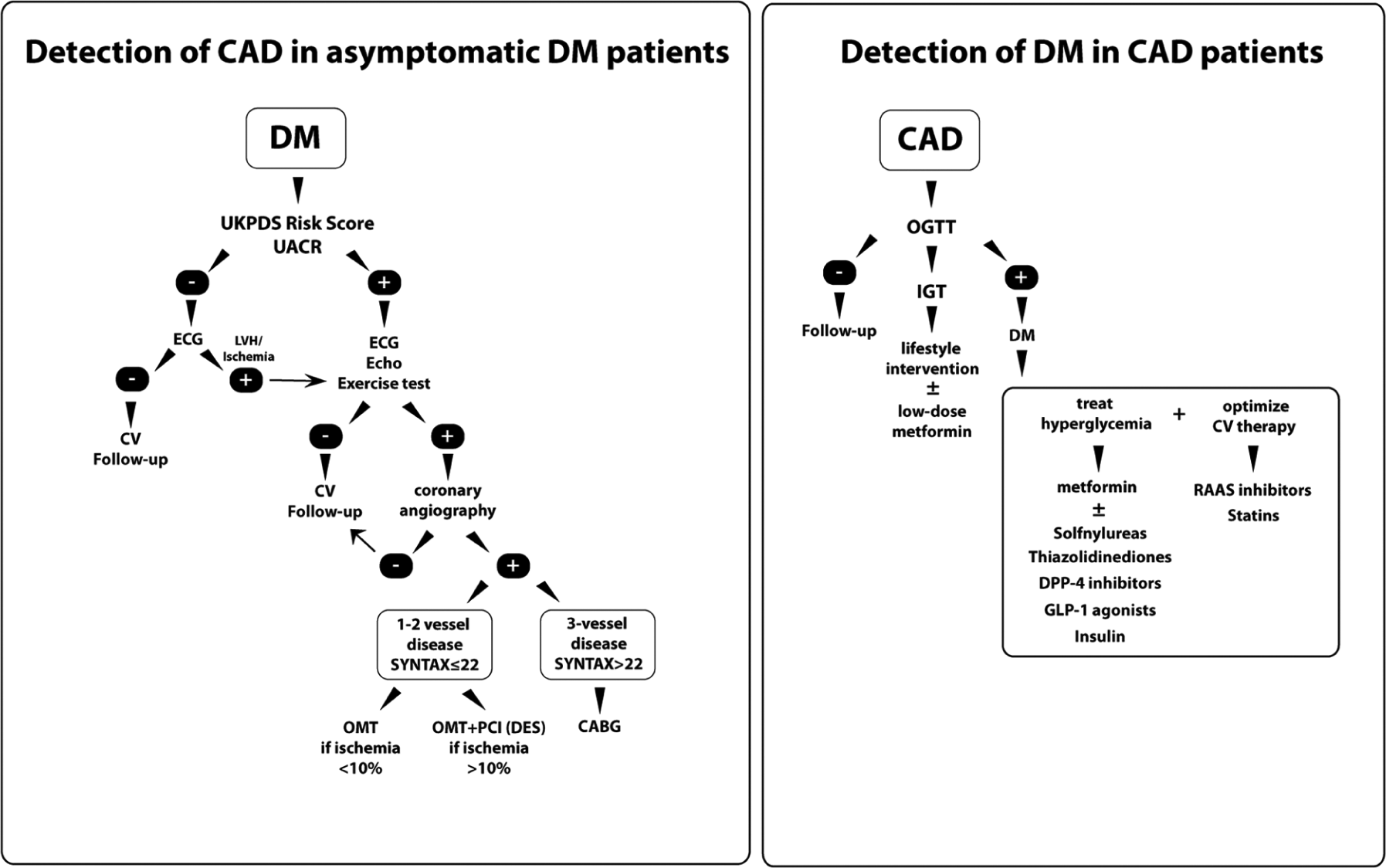
Algorithms for diagnosis and management of CAD in asymptomatic patients with diabetes (left panel) and diagnosis and management of diabetes in patients with CAD (right panel).
Estimation of cardiovascular risk
An important evidence gap is the lack of significant diagnostic tools for CV risk in the diabetes population. This uncertainty remains in the current guidelines since it is not clear how to stratify CV risk within the diabetic population and what are the implications for future management (Figure 2). Despite diabetes is being associated with a significant atherosclerotic burden, the role of vascular imaging in this setting remains poorly defined. Coronary artery calcium imaging has been found superior to established risk factors for predicting silent myocardial ischaemia and short-term outcome in a small cohort of high-risk DM subjects. 11 This is a rather expensive tool that may not be sustainable in developing countries. Moreover, the benefits of myocardial revascularization in asymptomatic patients remain to be determined (Figure 2). 8 The issue with the emerging biomarkers is that they hardly perform beyond traditional cardiovascular risk scores. The Atherosclerotic Risk in Communities (ARIC) study prospectively evaluated whether adding C-reactive protein or 18 other novel risk factors individually to a basic risk model would improve prediction of incident CAD in middle-aged men and women. 12 Unfortunately, none of these risk markers predicted CVD regardless of the risk score. Besides these disappointing results, current guidelines confirm that albuminuria remains the most powerful predictor of incident CV events and heart failure in T2DM patients and recommend to estimate urinary albumin excretion rate when performing risk stratification in DM subjects (class I, level B). Albuminuria predicts CVD beyond the United Kingdom Prospective Diabetes Study (UKPDS) risk engine, and their combination provides a reliable estimation of CAD risk in asymptomatic DM patients (Figure 1). However, CVD remains undiagnosed in a consistent proportion of DM patients, and more sensitive CV biomarkers are required (Figure 2).
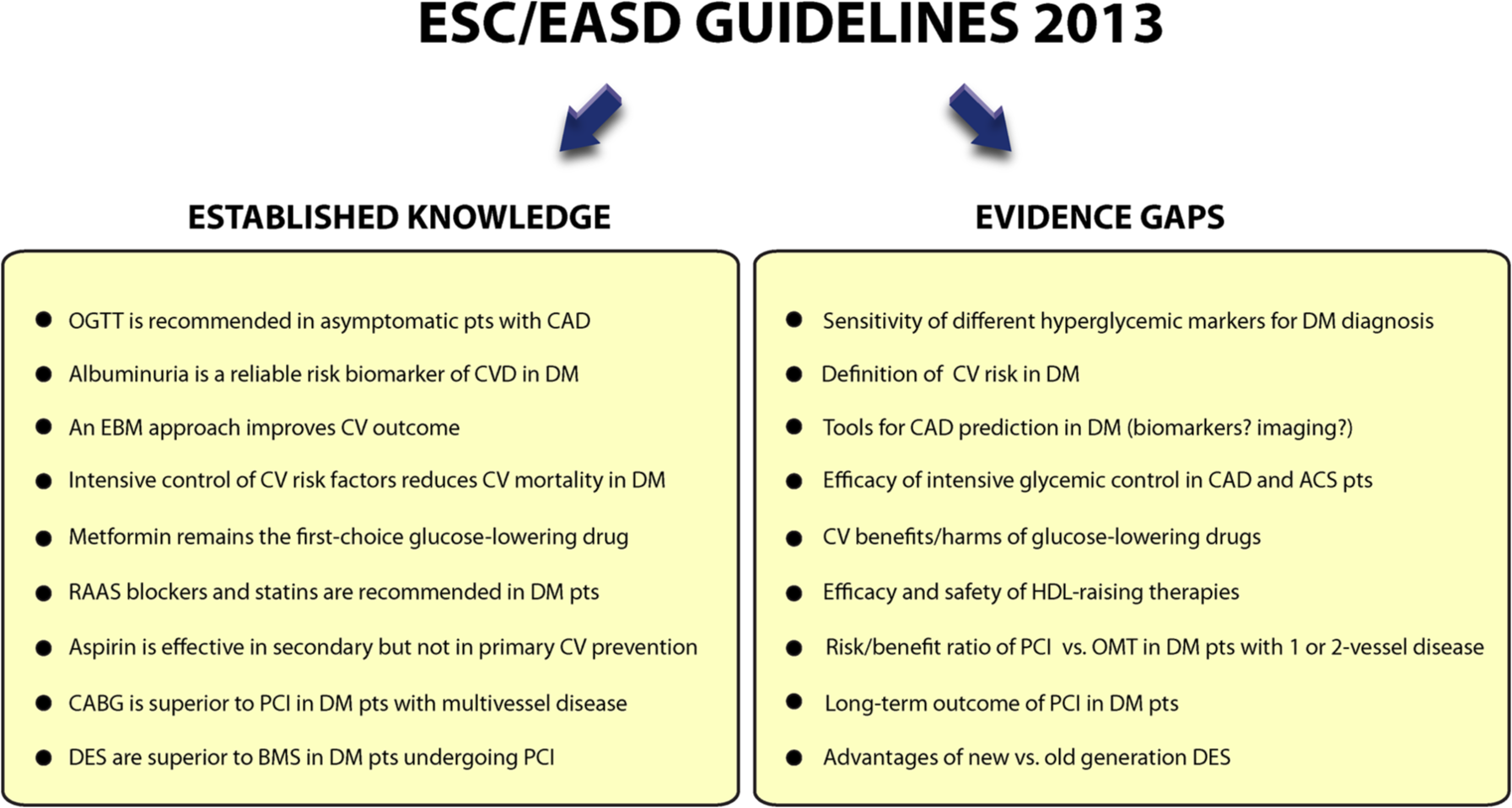
Established knowledge and evidence gaps on the management of diabetes and cardiovascular disease.
Glycaemic control and cardiovascular outcome
Major changes have been made to recommendations on glucose control. Intensified glucose lowering significantly reduces the frequency and severity of microvascular complications both in T1DM and T2DM, as shown in the Diabetes Control and Complications Trial (DCCT) and the UKPDS study, respectively. 8 Despite some controversy, the overall risk of macrovascular disease does seem to be affected by restoration of a euglycaemic state, as shown by recent randomized controlled trials. Indeed, research published since 2007 clearly demonstrates that glucose control has a modest effect on existing macrovascular complications and the effect takes a long time to become established. A meta-analysis of cardiovascular outcomes based on Veterans’ Administration Diabetes Trial (VADT), Action to Control Cardiovascular Risk in Diabetes (ACCORD) and Action in Diabetes and Vascular Disease (ADVANCE) suggested that an HbA1c reduction of 1% was associated with a 15% relative risk reduction in non-fatal myocardial infarction (MI) but without benefits on stroke or all-cause mortality. 13 In the ACCORD trial, hypoglycaemia increased CV mortality in patients with a long duration of diabetes (9 years). 8 Accordingly, the Outcome Reduction with Initial Glargine Intervention (ORIGIN) trial failed to show that early institution of insulin-based regimens reduces macrovascular complications. 14 In line with these findings, the new guidelines do not recommend very tight glucose control if the ambition is to reduce macrovascular complications. Moreover, in older patients with long-standing diabetes and cardiovascular complications, glycaemic control should be modest because of a concrete risk of hypoglycaemia and other side effects. Intensive glycaemic control to achieve an HbA1c target < 7% is effective but should be applied in an individualized manner taking into account DM duration and the presence of CVD and other co-morbidities. While 2007 guidelines emphasized the importance of tight glycaemic control in diabetic subjects, new ESC/EASD recommendations suggest that more caution should be paid when it comes to long-term hypoglycaemic strategies. By contrast, based on Diabetes Control and Complications Trial (DCCT)/Epidemiology of Diabetes Interventions and Complications (EDIC) and UKPDS, glycaemic control should be more aggressive in young patients free from CVD with a recent diagnosis of diabetes.
Glucose-lowering drugs
Among different glucose-lowering drugs, metformin remains the first choice due to its good safety profile and a modest benefit on the risk of MI (Figures 1 and 2). 8 However, this latter aspect is debatable since the CV benefits of metformin have been derived from a secondary end point of the UKPDS, and when administered in combination with a sulphonylurea may increase morbidity and mortality. Sulphonylureas in the absence of metformin also reduced MI and death in the UKPDS trial but were associated with increased body weight and hypoglycaemia. The efficacy of glitazones on CV outcomes is dependent on the secondary composite end point of the PROactive trial where pioglitazone significantly reduced all-cause mortality, fatal MI and stroke. Analysis of a secondary end point when the primary end point is non-significant is controversial, and this combined with the demise of rosiglitazone due to possible CV side effects has left a cloud over this class of drugs. Despite promising results on intermediate vascular end points and inflammation, incretin therapies with glucagon-like peptide-1 (GLP-1) agonists and dipeptidyl peptidase-4 (DPP-4) inhibitors do not seem to improve CV outcomes on top of conventional anti-diabetic treatment, as recently shown in Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus–Thrombolysis in Myocardial Infarction 53 (SAVOR TIMI-53) and Erbitux in First-Line Treatment of Recurrent or Metastatic Head and Neck Cancer (EXTREME) trials, which were published after the appearance of the current ESC/EASD guidelines. 15 The good news is that these compounds have no significant adverse effects and do not affect mortality. Hence, the major evidence gap is that long-term CVD outcomes of most glucose-lowering treatments are unknown and that none of these drugs have shown a definite CV benefit (Figure 2).
Treatment of cardiovascular risk factors
Established CV therapies such as statins and anti-hypertensive agents significantly improve the outcome of T2DM. In the STENO-2 trial, a multifactorial intervention was associated with a lower risk of death from CV causes [hazard ratio (HR) = 0.43; 95% confidence interval (CI) = 0.19–0.94; p = 0.04] and CV events (HR = 0.41; 95% CI = 0.25–0.67; p < 0.001). 16 Current ESC/EASD guidelines strongly recommend the use of statins both in T1DM and T2DM patients, regardless of CVD (class I, level A). By contrast, high-density lipoprotein (HDL) raising therapies are not recommended (class I, level III). 8 This latter statement is the result of new evidence demonstrating that increasing HDL levels may not be beneficial in DM patients. Accordingly, translational studies suggest that the protective effect of HDL cholesterol is lost in DM subjects with CAD. 17 Indeed, HDL isolated from DM patients displays a clear pro-apoptotic and pro-inflammatory phenotype. 17 Hence, raising HDL may have detrimental effects on long-term outcomes. While low-density lipoprotein (LDL)-lowering strategies remain a milestone of CV therapy in diabetes, the benefits of treating HDL and triglycerides remain elusive. Recent evidence suggests that alternative lipid-lowering strategies may be beneficial in the future. AMG145, a monoclonal antibody against proprotein convertase subtilisin/kexin type 9 (PCSK9), is emerging as a promising approach in subjects with hypercholesterolaemia receiving statin therapy, offering an additional, complementary benefit beyond robust LDL cholesterol reduction. 18
On the other hand, high priority is given to blood pressure control, and renin–angiotensin–aldosterone system (RAAS) blockers are strongly encouraged in DM patients with proteinuria or microalbuminuria (class I, level A). A new blood pressure target of <140/85 mmHg has been introduced for patients with diabetes and <130/80 mmHg in patients who also have kidney disease. Data accumulated during the last 5 years demonstrate that some patients showed an increased mortality risk when blood pressure is reduced too much. Hence, the approach to blood pressure has been individualized. The guidelines also confirm that aspirin is not recommended in DM patients without CVD or organ damage (low cardiovascular risk), whereas antiplatelet therapy should be personalized in high-risk diabetics. 8 Stratification of CV risk as low, intermediate and high in diabetic patients does not make much sense since a diagnosis of diabetes already implies a high risk of cardiovascular events overtime. For this reason, risk engines that accumulate risk factors and produce different risk categories may only partially route management of diabetic patients but should not be considered a fundamental step. Stratification of CV risk in diabetes may have dangerous implications since those patients classified as ‘low or intermediate risk’ will be likely ‘undertreated’. Along the same line, high-risk diabetics without CAD should receive the same treatment of diabetics with CAD. This is not the case because most of guidelines recommendations encourage treatment strategies based on the presence of CAD. For instance, aspirin treatment is recommended in secondary but not in primary prevention. However, many high-risk diabetics without CAD may benefit from an antiplatelet strategy, but risk thresholds for certain treatments remain undefined given the low number of subjects enrolled in clinical trials.
Myocardial revascularization strategies
The efficacy of different myocardial revascularization strategies in DM patients has been further delineated during the last 5 years. This is an important issue since a quarter of myocardial revascularization procedures are performed in the DM population. Revascularization in these patients is challenged by a more diffuse atherosclerotic involvement of epicardial vessels, a higher propensity to develop restenosis after percutaneous coronary intervention (PCI) and saphenous graft occlusion after coronary artery bypass grafting (CABG). 8 A meta-analysis of 10 randomized controlled trials comparing CABG versus PCI suggests a distinct survival advantage for CABG in DM patients. 19 Five-year mortality was 20% with PCI and 12% with CABG [odds ratio (OR) = 0.7; 95% CI = 0.6–0.9]. In the Future REvascularization Evaluation in patients with Diabetes mellitus: Optimal management of Multivessel disease (FREEDOM) trial, 1900 patients with advanced CAD were randomized to treatment with CABG or PCI with sirolimus- or paclitaxel-eluting stents. 20 After a median of 3.8 years, the primary outcome occurred more frequently in the PCI group with a 5-year rate of 26.6% compared with 18.7% in the CABG group (p < 0.005). Based on these findings, the current ESC/EASD guidelines recommend CABG in patients with multivessel disease or complex SYNTAX score (>22, class I, level A). 8 However, there remain important gaps in the management of stable CAD in diabetic patients: (1) It is still unclear whether optimal medical treatment should be preferred to elective PCI in asymptomatic diabetic patients with evidence of CAD and areas of ischaemia < 10%. (2) Long-term outcome in PCI-treated DM patients with less severe coronary anatomy (SYNTAX score ≤ 22) remains to be determined. In this regard, no randomized studies have been conducted to assess the efficacy of CABG versus PCI in diabetic patients with one- or two-vessel disease. (3) Despite a clear benefit of drug-eluting stents (DES) as compared with bar metal stents (BMS), the advances in the development of new-generation DES did not result into a further improvement of cardiovascular outcome and mortality in diabetics (Figure 2).
Conclusion
In summary, the recent ESC/EASD guidelines on the management of diabetes, pre-diabetes and CVD deliver a number of evidence-based recommendations designed to assist clinicians and other health-care providers in preventing, diagnosing and treating CVD in patients with DM.
While several aspects have been clarified and are considered established knowledge, consistent evidence gaps remain due to a small number of randomized studies or heterogeneity of the populations studied (Figure 2). During the next decade, efforts in clinical and translational research should address important clinical issues such as the identification of reliable biomarkers for CV risk stratification, the definition and management of high-risk patients and very high-risk patients, the effectiveness of intensive glycaemic control in diabetics with stable and acute CAD as well as the benefit of new glucose-lowering drugs in the prevention of cardiovascular outcome.
Footnotes
Declaration of conflicting interests
F.P. has no disclosures regarding this article.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.