
Abstract
The Diabetes mellitus Insulin-Glucose Infusion in Acute Myocardial Infarction (DIGAMI) 2 Quality of Life (QoL) sub-study included 465 patients with type 2 diabetes and acute myocardial infarction (AMI) followed for 2 years. Self-rated health was reported by the rating scale (RS), graded 0 = death to 100 = perfect health. Prospective associations between RS and all-cause mortality, cardiovascular (CV) death and cardiovascular events (CVEs = CV death, non-fatal AMI, stroke) were assessed. Median age was 68 years (range 59–74), 68% male. Patients experiencing CVE (n = 132) or death (n = 71) had lower RS compared with patients free from events: 60 (50–79) versus 70 (55–81) (p < 0.001) and 60 (50–75) versus 70 (51–80) (p = 0.008). The RS score predicted CVE [hazard ratio (HR); 95% confidence interval (CI): 0.87; 0.80–0.95] and all-cause mortality (0.86; 0.76–0.97), and corresponding HRs after adjustment were 0.90; 0.83–0.99 and 0.90; 0.79–1.02, respectively. A low self-rated health is of prognostic importance in patients with type 2 diabetes and AMI and may serve as an easily obtainable indicator of high risk for CVEs supplementing traditional risk factors.
Introduction
Diabetes mellitus is a common disorder with a currently estimated global prevalence of 8.3% and is projected to increase to 9.9% in the coming 20 years. 1 In adults, type 2 diabetes accounts for more than 90% of all diabetes diagnoses. 2 Compared to the general population, type 2 diabetes is associated with a two- to threefold increase in mortality 3 and for patients with already established cardiovascular disease (CVD) even higher. A simple and reliable test to identify persons with the highest risk could allow implementation of early intervention and possibly improve their outcome.
Type 2 diabetes has implications on many aspects of life, and negative effects on health-related quality of life (QoL) are not uncommon. 4,5 Patients diagnosed with CVD generally report worse health-related QoL than patients with type 2 diabetes only, 6 and an incremental effect has been suggested in patients with both diseases. 7,8
The prognostic value of health-related QoL has been established in patients with chronic illnesses such as heart failure 9,10 and kidney disease. 11 Similar associations have also been observed in patients with type 2 diabetes 12,13 and in patients with CVD. 14,15 However, the prognostic importance of QoL assessments in patients with both type 2 diabetes and CVD is less well investigated. The aim of the present investigation, a predefined sub-study of the DIGAMI 2 trial, was to test the hypothesis that self-related health and psychological well-being contribute with prognostic information of patients with type 2 diabetes and acute myocardial infarction (AMI).
Study design and methods
Study population
The present QoL study was a pre-planned sub-study in the DIGAMI 2 population and consisted of 509 patients from 28 centres in the four Nordic countries: Denmark (n = 68), Finland (n = 30), Norway (n = 63) and Sweden (n = 348).
The DIGAMI 2 included 1253 patients with type 2 diabetes and suspected AMI. A detailed description of the study design has been presented elsewhere. 16 In brief, patients were included if they had type 2 diabetes (established or blood glucose > 11.0 mmol/L at admission) and were hospitalised due to a suspected AMI based on chest pain >15 min during the preceding 24 h and/or recent electrocardiogram (ECG) signs (new Q-waves and/or ST-segment deviations in two or more leads). Exclusion criteria were inability to cope with insulin treatment, residence outside the hospital catchment area, and previous participation in DIGAMI 2 or other studies. The patients were randomised to one of the three following glucose-lowering strategies: (1) acute insulin–glucose infusion during at least 24 h followed by multi-dose insulin long-term (n = 474), (2) insulin–glucose infusion acutely followed by standard therapy long-term (n = 473) or (3) control patients given glucose-lowering treatment according to local practice (n = 306). No statistically significant differences in glucose control, cardiovascular event (CVE) rates or mortality were noticed between the treatment groups during the median follow-up period of 2.1 years.
Ethics
All patients gave their written consent to participate in this study, which followed the standards of good clinical practice and had been approved by local ethics review boards. The investigation was carried out in accordance with the Declaration of Helsinki.
Study protocol
QoL questionnaires were administered after randomisation but prior to hospital discharge and before starting insulin. Patients were asked to rate their overall feeling of health by the means of a rating scale (RS) and their psychological well-being by the Psychological General Well-Being (PGWB) index questionnaire. Both forms are self-administered and were filled out by the patients themselves.
The RS is a preference-based measurement tool using a simple technique for assigning a numerical value for a certain health state. 17 It consists of a straight vertical scale [Visual Analogue Scale (VAS)] numbered from 0 to 100, where 0 is death and 100 is perfect health. Patients were asked to mark their current health state on the vertical line in relation to perfect health and death.
The PGWB Index is an epidemiological measure of health-related QoL, developed to provide a frequency and intensity measure of subjective well-being or distress. It focuses on aspects of mental health. 18 It consists of 22 questions divided equally between positive and negative aspects and evaluates six dimensions of well-being: anxiety, depressed mood, vitality, general health, self-control and well-being. Each item is rated on a 6-graded scale and evaluated by the total score of all questions. Highest possible score is 132, and a higher number means a greater feeling of well-being and a lower number means a worse feeling of well-being. After discharge, patients were followed up for CVEs (fatal and non-fatal re-infarction or stroke), CV death and all-cause mortality for up to 3 years.
Definitions and adjudication of events
Events were collected at follow-up visits every 6 months and via hospital records when needed. There was no loss to follow-up. AMI was diagnosed in accordance with the joint recommendations of the European Society of Cardiology (ESC) and American College of Cardiology (ACC). 19 Re-infarction was defined as an event >72 h from the index infarction. Stroke was defined as unequivocal signs of focal and global neurological deficit of sudden onset and duration of exceeding 24 h that were judged to be of vascular origin. Complete mortality data were obtained from death certificates and autopsy reports when available. All events were adjudicated by an independent committee composed of three experienced cardiologists.
Data and statistical analysis
The RS score was included in the analysis if the score was clearly marked with a cross or vertical line across the scale. Patients who used a circle or more than one cross to mark the line were excluded. As specified in the study protocol, the PGWB questionnaires were included in the analyses if ≥60% of questions had been addressed by the patient. In the included questionnaires, missing data were replaced by the whole populations’ mean value for that question before an individual total score was calculated.
Continuous variables are presented as median and interquartile range, and the Wilcoxon–Mann–Whitney rank sum test was used for the comparison between values. Categorical variables are expressed as counts and proportions, and Fisher’s exact test was used for the comparison between categorical data. A two-sided p value < 0.05 was considered statistically significant. Crude and adjusted prospective associations between RS and PGWB scores and CVE, CV death and all-cause mortality were assessed by Cox proportional hazard regression. Potential confounders for the Cox regression analyses were chosen from univariable analyses accepting those with a p value < 0.05. Survival stratified by RS scores above and below median is presented as Kaplan–Meier survival plots. Minitab version 16 and SAS 9.2 were used for analyses.
Results
Patients
A total of 465 of the 509 study participants completed both questionnaires successfully (correctly marked RS score and ≥60% of PGWB questions answered). Their median age was 68 years and 68% were males. Baseline characteristics for the whole group and by gender are shown in Table 1. In general, women were older and had higher cholesterol levels and a more frequent history of hypertension. Men had a higher creatinine clearance and a higher prevalence of previous coronary artery bypass grafting (CABG). Women reported significantly lower RS scores compared to men, while there was no gender difference in the total PGWB score (Table 1); 210 patients had RS scores below median and 255 had RS scores above median (Figure 1). Patients with RS scores below median had a higher prevalence of hypertension (43% vs 54%, p = 0.019), heart failure (24% vs 13%, p = 0.003) and previous CABG (16% vs 10%, p = 0.049), and they also had lower PGWB scores [median (interquartile range): 76 (72–81) vs 79 (76–82), p < 0.001].
Baseline characteristics.
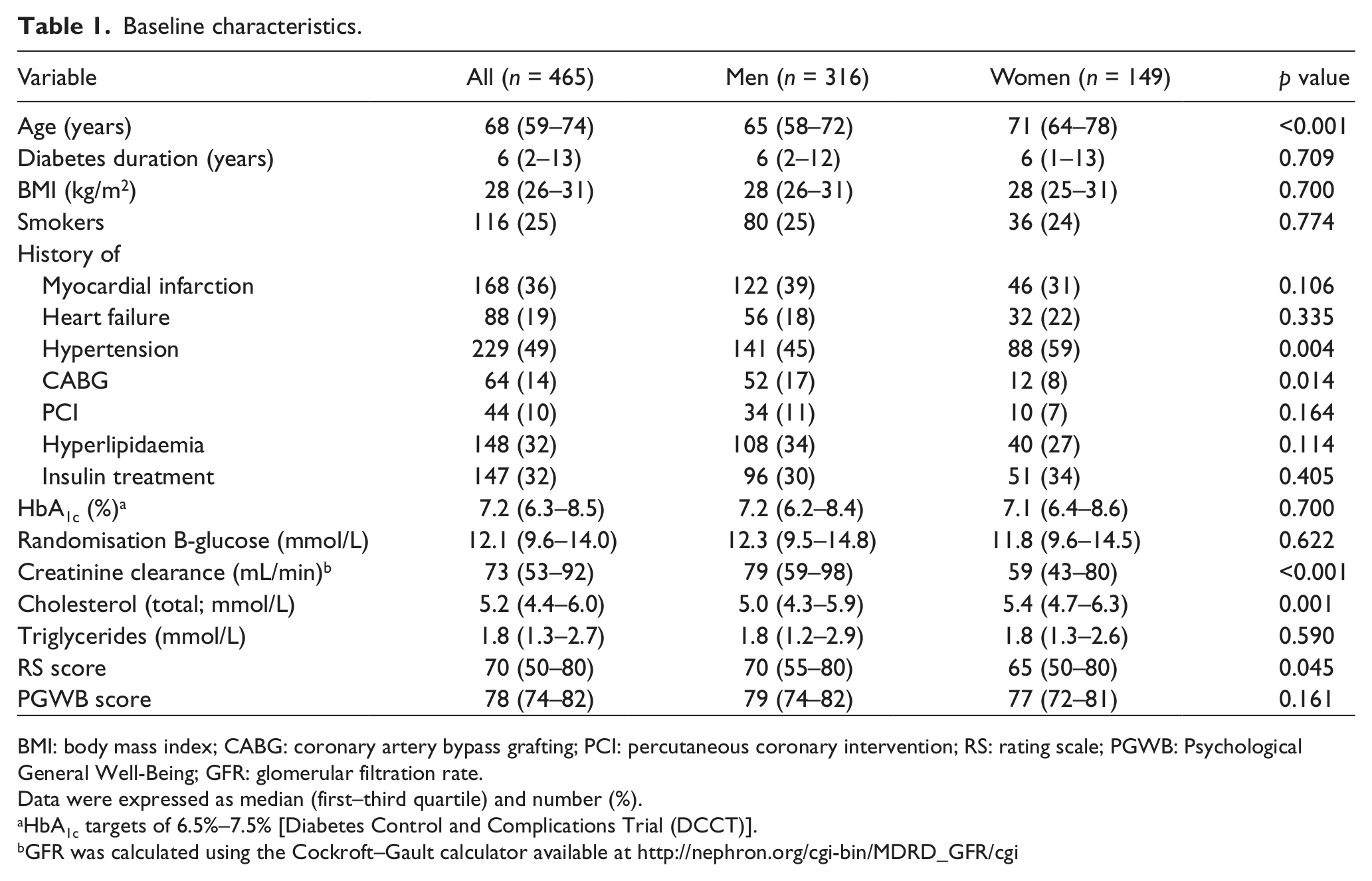
BMI: body mass index; CABG: coronary artery bypass grafting; PCI: percutaneous coronary intervention; RS: rating scale; PGWB: Psychological General Well-Being; GFR: glomerular filtration rate.
Data were expressed as median (first–third quartile) and number (%).
HbA1c targets of 6.5%–7.5% [Diabetes Control and Complications Trial (DCCT)].
GFR was calculated using the Cockroft–Gault calculator available at http://nephron.org/cgi-bin/MDRD_GFR/cgi
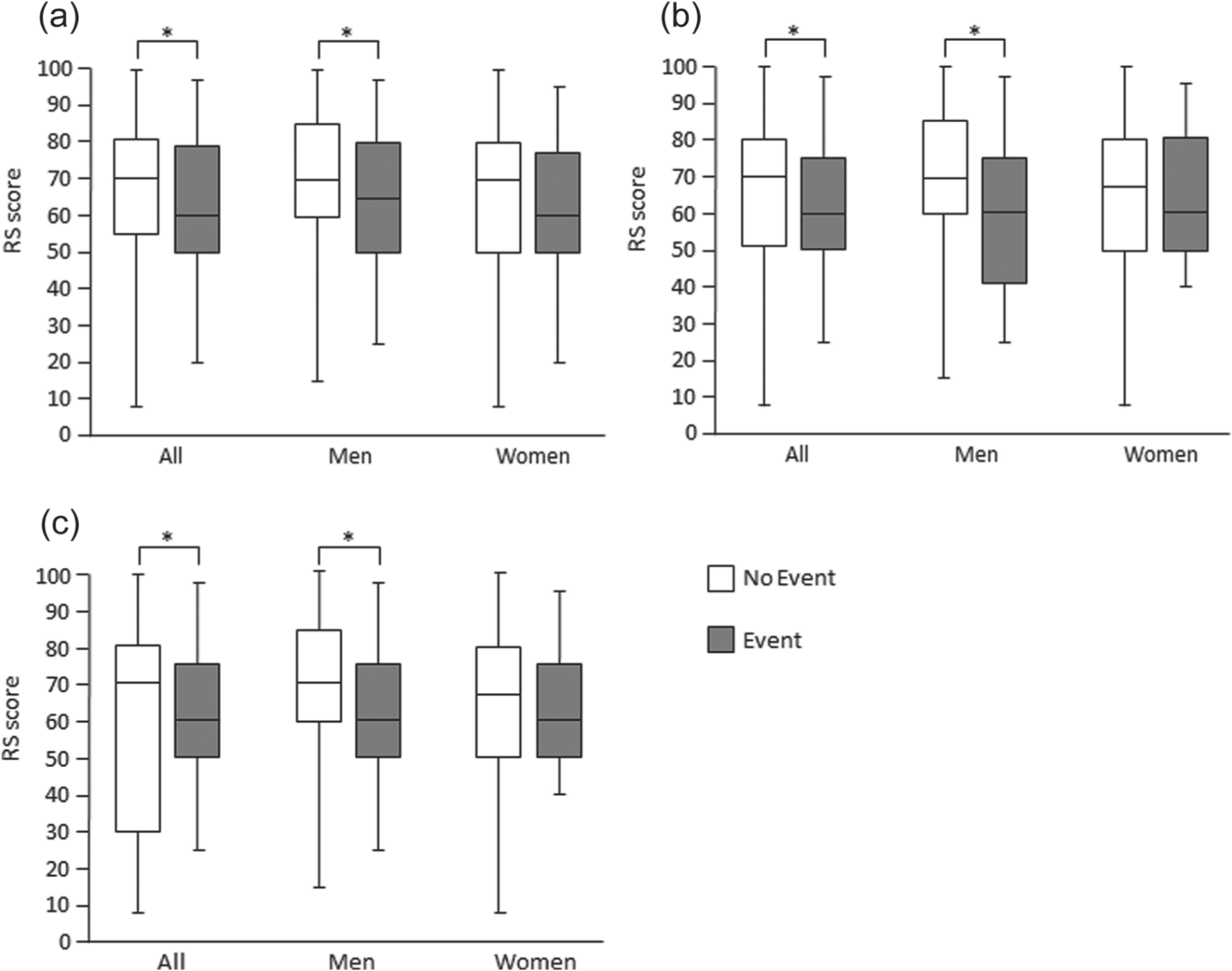
Crude associations between gender, follow-up events and RS scores given as median (first–third quartile): (a) CVEs, (b) all-cause mortality and (c) CV death.
The median duration of follow-up was 2.1 years (interquartile range: 1.0–3.0 years). During the course of the study, 132 (28%) participants experienced CVE and 71 (15%) participants died, and of those 71 participants, 58 died by CV reasons. No differences were noticed in event rates between genders. Of CV deaths, 41% occurred within the first 6 months after the myocardial infarction, corresponding to one-third of the total mortality.
The 44 patients who were excluded from the analysis had similar baseline characteristics as the studied cohort apart from a higher age [median (first–third quartile): 71 years (63–77) vs 68 years (59–74), p = 0.045] and longer diabetes duration [10 years (4–17) vs 6 years (2–13), p = 0.021]. In addition, they had more CVEs and a higher mortality [n = 20 (45%) vs 132 (28%), p = 0.022 and n = 15 (34%) vs 71 (15%), p = 0.001].
Risk predictors
The median RS score was lower among male patients experiencing CV death or all-cause mortality than among their event-free counterparts. No such associations were observed in women (Figure 1).
A number of risk factors were examined in univariable analyses, and those with a p value < 0.05 were selected for the adjusted end point analysis. Age and chronic heart failure were independent predictors of mortality in both genders, while previous myocardial infarction and creatinine clearance predicted mortality in men and a high body mass index (BMI) in women. Previous myocardial infarction and chronic heart failure were predictors of CVEs in both genders, while age and creatinine clearance predicted CVEs only in men.
In the presented cohort of patients, a 10-point decrease in RS score associated with a 13% increased risk of a CVE in the unadjusted analysis and 10% increased risk of a CVE after adjustment for prognostic variables. It was also associated with a 14% increase in death from any cause. Following the adjusted analysis, this association was attenuated in women (Table 2), but the gender-by-RS score interaction was non-significant (p = 0.2). Mortality in relation to RS scores above and below median for the total patient cohort is shown in Figure 2(a) and for gender-specific distribution is shown in Figure 2(b). Separation in survival develops by time and is small, if any, during the first 6 months.
Crude and adjusted prospective associations between RS scores and CVEs, all-cause mortality and CV death given as HR with 95% CI.
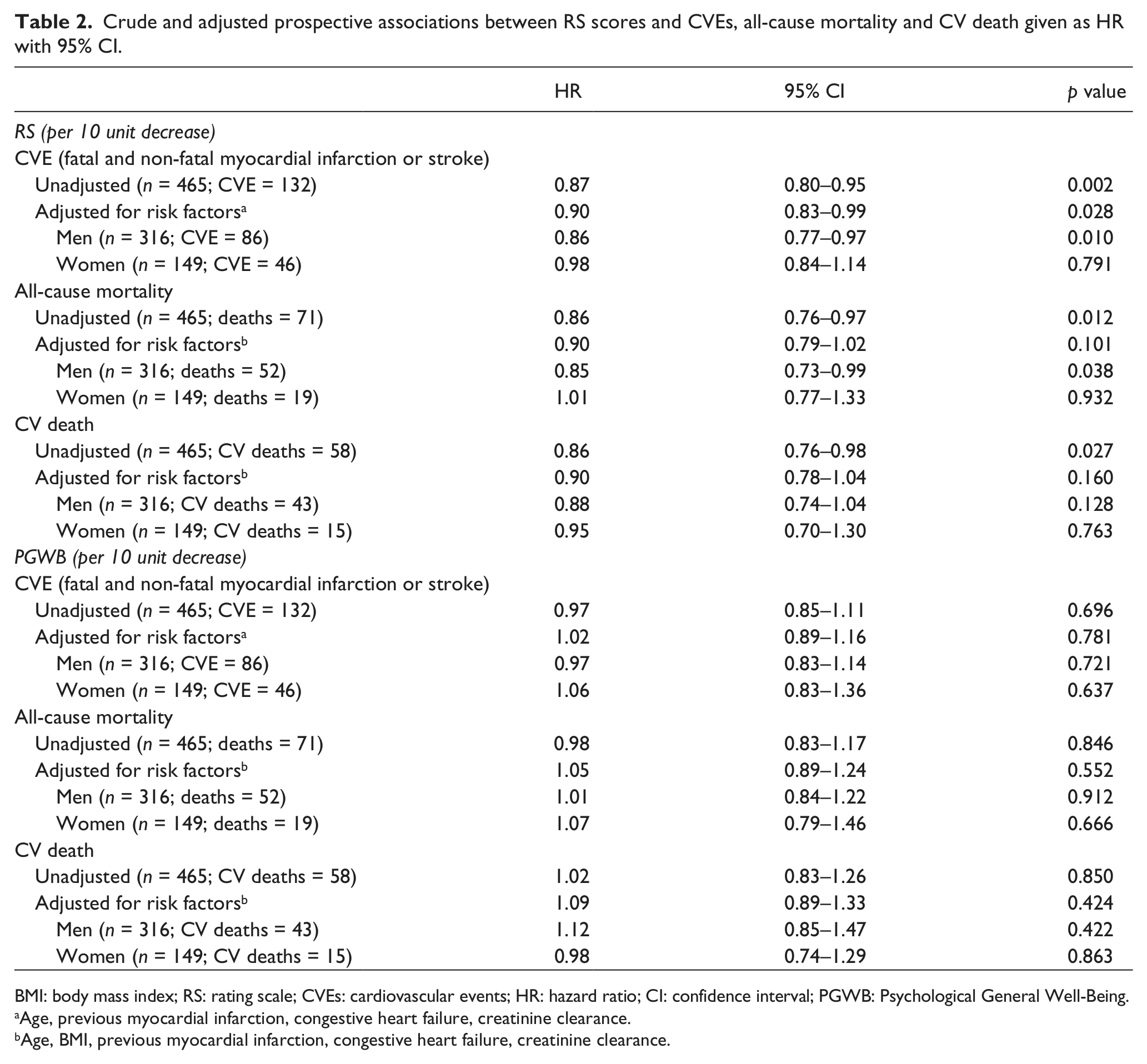
BMI: body mass index; RS: rating scale; CVEs: cardiovascular events; HR: hazard ratio; CI: confidence interval; PGWB: Psychological General Well-Being.
Age, previous myocardial infarction, congestive heart failure, creatinine clearance.
Age, BMI, previous myocardial infarction, congestive heart failure, creatinine clearance.
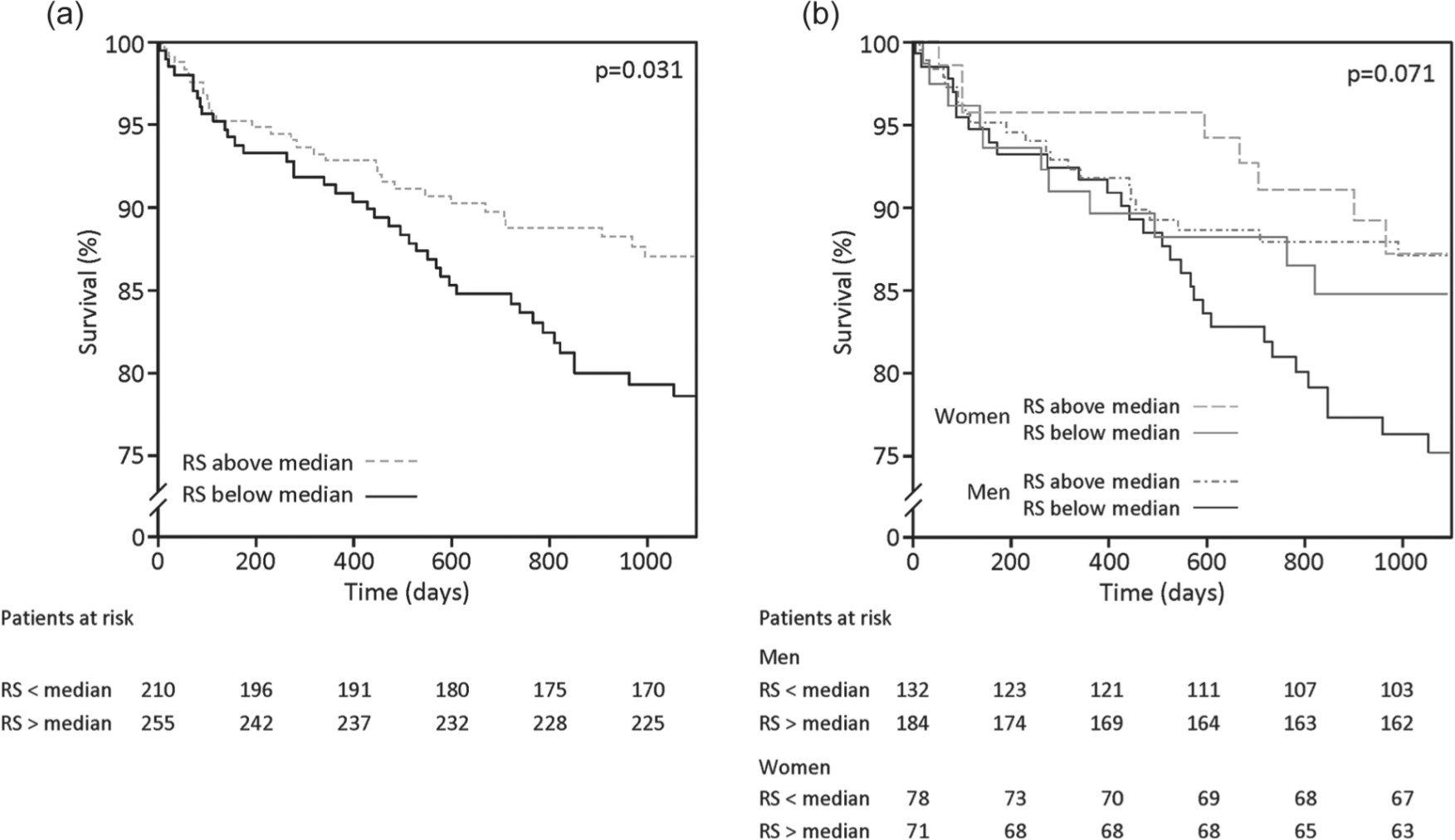
Cumulative survival in relation to RS scores above and below the median (a) for the total patient cohort and (b) by gender.
The PGWB scores were similar in both genders. There were no associations between PGWB and survival (Table 2).
Discussion
Patient self-rated health measured by a single-item RS identified patients with type 2 diabetes and AMI who are at risk of subsequent CVEs or death from any cause. When analysed by gender, this association was apparent only in men. Psychological well-being did not predict outcome.
The combination of a prospective trial design, high adherence to follow-up, uniform treatment prescriptions and a large number of well-defined and adjudicated end points is the major strength in this study. Previously reported data showed that the psychological well-being was good and comparable to the general population of same age and that treatment with glucose-lowering agents was well accepted. 5
Identification of individuals at increased risk of unfavourable outcome is important in clinical practice. Measures such as self-rated health may add information beyond that of conventional risk factors thereby contributing to decision-making. A relation between self-rated health and survival has been described but, to the best of our knowledge, not in patients with type 2 diabetes and myocardial infarction. Health-related QoL may be investigated with generic and/or disease-specific tools, and the choice of instrument should suite the purpose. Disease-specific questionnaires are designed to reflect the effects of treatment, including changes over time, while generic measures investigate broader areas of functioning. 20 For the purpose of this study, investigating the predictive value of self-perceived QoL, generic rather than disease-specific tools were preferred. The RS, a single-item VAS, was selected as a simple, validated tool to quantify general feeling of health. 17 It has been claimed that single-item tools are valid and reliable when assessing health-related QoL, 21,22 but it has also been suggested that they lack precision and depth in the gathering information. 23 However, the simplicity and easy administration of single-item tools make them highly feasible in a clinical setting, not the least when caring for patients with acute illnesses. The PGWB is a validated measure of mental health, which has been tested in patients with type 2 diabetes 24 and considered appropriate for measuring psychological well-being. 25
The predictive power of the RS score appeared successively (see Figure 1). The lack of difference in a short-term perspective may be explained by the high mortality early after the myocardial infarction reflecting risk related to that condition rather than other physical or psychologically oriented factors. 25 In a long-term perspective, a tentative contributing factor may be a decline in medication adherence, described to occur 6–12 months after hospital discharge. 26 This has been related to an unfavourable long-term outcome both in patients with myocardial infarction 26 and in patients with diabetes. 27 In the present cohort, patients with RS scores below median had more co-morbidities and lower psychological well-being measured by the PGWB compared with those with RS scores above median. Thus, one might speculate that patients with a worse perceived health are less compliant to their prescribed therapy, which may have prognostic implications. Since information on prescription adherence was unavailable, this possibility remains hypothetical but of importance to further explore. The low RS score signals a demand of increased attention in all aspects. It is, however, beyond the scope of this study to elaborate on how.
While RS score predicted CVEs and mortality in the total cohort, the gender-specific analyses only confirmed a significant association in men. A general pattern in health-related QoL studies is that women rate their experienced health lower than men. This is seen across different age groups and in a number of clinical conditions. 28,29 A less favourable rating in women seems to be of lower prognostic value in contrast to the impact of an as low-reported health status in men. Men tend to report fewer but more disease-specific symptoms, while women are more likely to take less disease-relevant conditions, among them needs, priorities and social function, into account. 30,31 The lack of associations between PGWB and unfavourable outcomes makes it unlikely that the prospective implications of the RS only related to a compromised psychological status. Moreover, diabetes has been reported to affect physical well-being more than psychological well-being, 24 which may explain the lack of predictive power of PGWB.
Study limitations
The lack of predictive value among female patients may reflect a type 2 statistical error considering the limited number of such patients making further exploration of possible gender differences appropriate. The method chosen for evaluation of self-rated health may be associated with some disadvantages. The RS has a simple design, but it may be difficult to answer one global question ignoring other aspects not relevant to the actual situation. Finally, a positive selection bias cannot be excluded due to the higher event rate observed in the limited group of patients who failed to report a baseline RS score.
Conclusion
The RS identified patients with type 2 diabetes and AMI who are at increased risk of mortality or CVEs beyond that of traditional risk factors. When analysed by gender, this association was apparent in men only, but further studies in larger patient cohorts are needed to verify a true gender-related difference. Introduced in routine clinical practice, the easily applied RS score may improve the identification of patients at risk and subsequent decision-making adding a dimension related to the patient’s perception of the situation.
Footnotes
Acknowledgements
The authors are grateful to Christina Edman-Jönsson, Karolinska Institutet, Stockholm, for excellent study managing.
Conflict of interest
None of the authors have any financial interests, besides research funding, or relationships and affiliations related to the relevance to the subject of this study.
Funding
This study was supported by the Swedish Heart and Lung Foundation, AFA Insurance and by unconditional research grants from Aventis, Sweden and Novo Nordisk, Denmark.