
Abstract
We studied the impact of diabetes mellitus (DM) on the radial artery (RA) in 30 patients with DM and 30 non-diabetic patients undergoing coronary artery bypass grafting with autologous RA. RAs were recorded as normal if there was no cellular or stromal tissue between the endothelium and the internal elastic lamina. The RA was normal in 26.7% of diabetic and 76.7% of non-diabetic patients (p = 0.000298). Intimal thickness index and intima:media ratio were higher in the former than in the latter (p < 0.05; p < 0.05), with no significant difference in luminal narrowing (p > 0.05). Electron microscopy scores were lower in the non-diabetic group (p < 0.001); endothelial nitric oxide synthase (eNOS) protein expression and optical density were higher (p < 0.001). Von Willebrand factor and endothelin-1 messenger RNA (mRNA) levels were higher in the DM patients (p < 0.001). The quality of the RA in patients with DM was thus inferior to that in non-diabetic patients. Care should be taken when selecting RA as a conduit in patients with DM.
Keywords
Introduction
The radial artery (RA) has become a popular conduit for coronary artery bypass grafting (CABG), particularly as part of an ‘all arterial’ grafting strategy. It has been shown that RA has good early and mid-term patency, 1 and may have superior long-term patency.2,3
Coronary artery disease is more common in individuals with diabetes mellitus (DM) than in those without, and a large population of the former needs CABG. Although DM is considered a risk factor for RA disease, the incidence of the disease in the diabetic RA has not been widely investigated, and the effects on its molecular biology are even less clear. In this study, we compared RA pathology between CABG patients with DM and non-diabetic patients using haematoxylin and eosin (H&E) staining and transmission electron microscopy (TEM). We also sought to investigate whether DM has any negative effects on RA endothelial function in diabetic patients by determining the expression of endothelial nitric oxide synthase (eNOS), and endothelin-1 (ET-1) and Von Willebrand factor (vWF) messenger RNA (mRNA).
Methods
Patient characteristics
Approval for this study was obtained from the Institutional Review Board of Nanjing First Hospital affiliated to Nanjing Medical University, with additional patient consent waived. From June 2009 to December 2010, 30 patients with DM undergoing CABG were enrolled. Their age ranged from 47 to 72 years (mean ± standard deviation = 61.2 ± 7.8). There were 18 men and 12 women. A total of 30 control participants without DM undergoing CABG were also recruited. The study population characteristics are summarized in Table 1.
Clinical characteristic of 60 patients undergoing coronary artery bypass grafting.
DM: diabetes mellitus; BMI: body mass index.
RA harvesting and sampling protocol
Contraindications to RA harvesting in this study were as follows 4 : (a) inadequacy of the ulnar collateral circulation to the hand, (b) diffusion atherosclerosis and medial calcification, (c) obvious stenosis, (d) small inner size (<2 mm in diameter), (e) anomalies such as high bifurcation of the brachial artery or hypoplasia of the radial or ulnar artery on Doppler ultrasound examination, (f) previous RA cannulation, (g) prior surgery on the forearm leading to periarterial fibrosis, (h) need for haemodialysis or fistulation of the RA and (i) stenosis of the subclavian artery.
The non-dominant arm was generally used for RA harvesting. All RAs were harvested using a ‘no touch’ technique along with its pedicle. The unused RA segments were collected and transferred immediately to the laboratory for examination.
H&E analysis of intimal thickening and atherosclerosis
RAs were harvested from 60 patients (30 with DM and 30 without DM). RA segments of length 5–6 mm were processed and embedded in paraffin blocks. Sections of thickness 5 µm were cut and stained with H&E. A pathologist blinded to the clinical data examined the slides with a digital microscope (Olympus BX51; Olympus, Tokyo, Japan). Three parameters 5 were used to evaluate the degree of intimal thickening and atherosclerosis: (a) percentage of luminal narrowing (LN), (b) intimal thickness index (ITI) and (c) intima:media ratio (IMR). The severity of disease was calculated from the most severely diseased section using the following formulas: LN = 100 × intimal area/internal elastic lamina area, ITI = intimal area/medial area and IMR = width of intima at maximal intimal thickness/width of media at maximal intimal thickness. Intimal thickening and medial thickness were measured using Image Pro-Plus software (Version 6.0 for Windows™, Media Cybernetics, Inc.) and the values were expressed in micrometers.
TEM of RA
RA samples of length 5 mm were immersed and fixed in 2.5% glutaraldehyde solution for more than 24 h, then washed in phosphate buffer (pH = 7.4), post fixed in 1% osmium tetroxide and dehydrated in increasing concentrations of acetone. Ultrathin sections of thickness about 60 nm were collected in copper grids, and stained with uranylacetate and lead citrate. In total, 10 samples were chosen randomly from each group for examination under an H-7650 transmission electron microscope (Hitachi High-Technologies, Tokyo, Japan). The histopathologist was blinded to the clinical data. A semi-quantitative method of scoring 6 was applied to the slides, each of which was evaluated for three different morphologic changes as follows: (a) structure of endothelial cells, (b) degree of tissue oedema and (c) morphologic changes of mitochondria in endothelial cells. Morphologic changes of the tissue samples were scored according to following criteria 6 : (a) structure of endothelial cells: 0, ultrastructurally in normal thickness; 1, endothelial cells which have a decrease in their thickness; 2, presence of discontinuities in the endothelial wall and 3, presence of completely damaged endothelial layer. (b) degree of tissue oedema: 0, no oedema in the wall of the arteries; 1, oedema in the endothelial layer; 2, oedema in the endothelium and subendothelium and 3, oedema in the endothelium, subendothelium, tunica media and tunica adventitia. (c) morphologic changes of mitochondria in endothelial cells: 0, normal; 1, mild degree of swelling (mitochondrion with prominent cristae); 2, swollen mitochondrion (cloudy swelling) and 3, amorphous material deposition in the mitochondrion. Four different areas on each slide were evaluated and scored. Four average scores (endothelial score, oedema score and mitochondrial score and the sum of the three) were obtained for every sample. Mean scores were calculated for each group.
Determination of eNOS expression by Western blot analysis
Ten RA samples were chosen randomly from each group. The vessels were washed with phosphate buffer solution, ground into fine powder on ice and suspended in lysis buffer containing a protease inhibitor cocktail. The tissue was homogenized and centrifuged at 12,000 rpm for 30 min at 4°C, and the protein concentration in the supernatant was measured using the bicinchoninic acid (BCA) protein assay. Equal amounts of protein (60 μg) were boiled for 5 min, resolved on 8% sodium dodecyl sulphate polyacrylamide gel electrophoresis (SDS-PAGE), transferred to nitrocellulose membrane and probed with diluted anti-eNOS antibody (1:200) (SC654; Santa Cruz Biotechnology, Santa Cruz, CA, USA). The nitrocellulose membrane was blocked in 5% non-fat dry milk overnight at 4°C. The blots were subsequently incubated with horseradish peroxidase conjugated secondary antibody (1:4000) (Santa Cruz Biotechnology). Bound antibody was detected by electrochemiluminescence. The experiments were repeated thrice.
Measurement of vWF and ET-1 mRNA by quantitative reverse transcription polymerase chain reaction
Total RNA was extracted from RAs using TRIzol reagent (Invitrogen, Carlsbad, CA, USA). mRNA levels were measured by real-time reverse transcription polymerase chain reaction (RT)-PCR using Platinum SYBR Green qPCR SuperMix-UDG (Invitrogen, Carlsbad, CA, USA) according to the manufacturer’s instructions. The following primer sequences are listed in Table 2. vWF and ET-1 mRNA levels in each sample were normalized to that of β-actin mRNA. The quantitative end point for real-time PCR (RT-PCR) is the threshold cycle (CT). The method 7 was applied to compare gene expression between two samples: ΔCT = (CT gene of interest − CT internal control). The amplification was monitored on an ABI Prism 7500 real-time PCR apparatus (Applied Biosystems, Foster City, CA, USA). The RT-PCR conditions were as follows: 95°C, 2 min (95°C 15 s) and annealing temperature 52°C, 30 s.
Primers used for real-time reverse transcription PCR.
vWF: von Willebrand factor; PCR: polymerase chain reaction; ET-1: endothelin-1.
Statistical analysis
SPSS 13.0 software was used for statistical analysis of the data. Continuous and interval-related data were expressed as the mean ± standard deviation. The U-test and Student’s t-test were used. A p value less than 0.05 was considered significant in the final model. Two-tailed probability was applied to all statistical tests.
Results
H&E analysis
RAs were recorded as normal if there was no cellular or stromal tissue between the endothelium and the internal elastic lamina. 8 RAs were considered abnormal when they exhibited intimal thickening, endothelial denudation or atherosclerotic lesions (Figure 1). Comparative morphometric analysis revealed significant differences in ITI and IMR between the RAs from diabetic patients and the non- diabetic samples (0.89 ± 0.26 vs 0.30 ± 0.27, t = 8.62, p < 0.05; 0.89 ± 0.22 vs 0.39 ± 0.20, t = 9.21, p < 0.05) (Table 3). However, there was no significant difference in LN between the two groups (t = 0.06, p > 0.05) (Table 3).
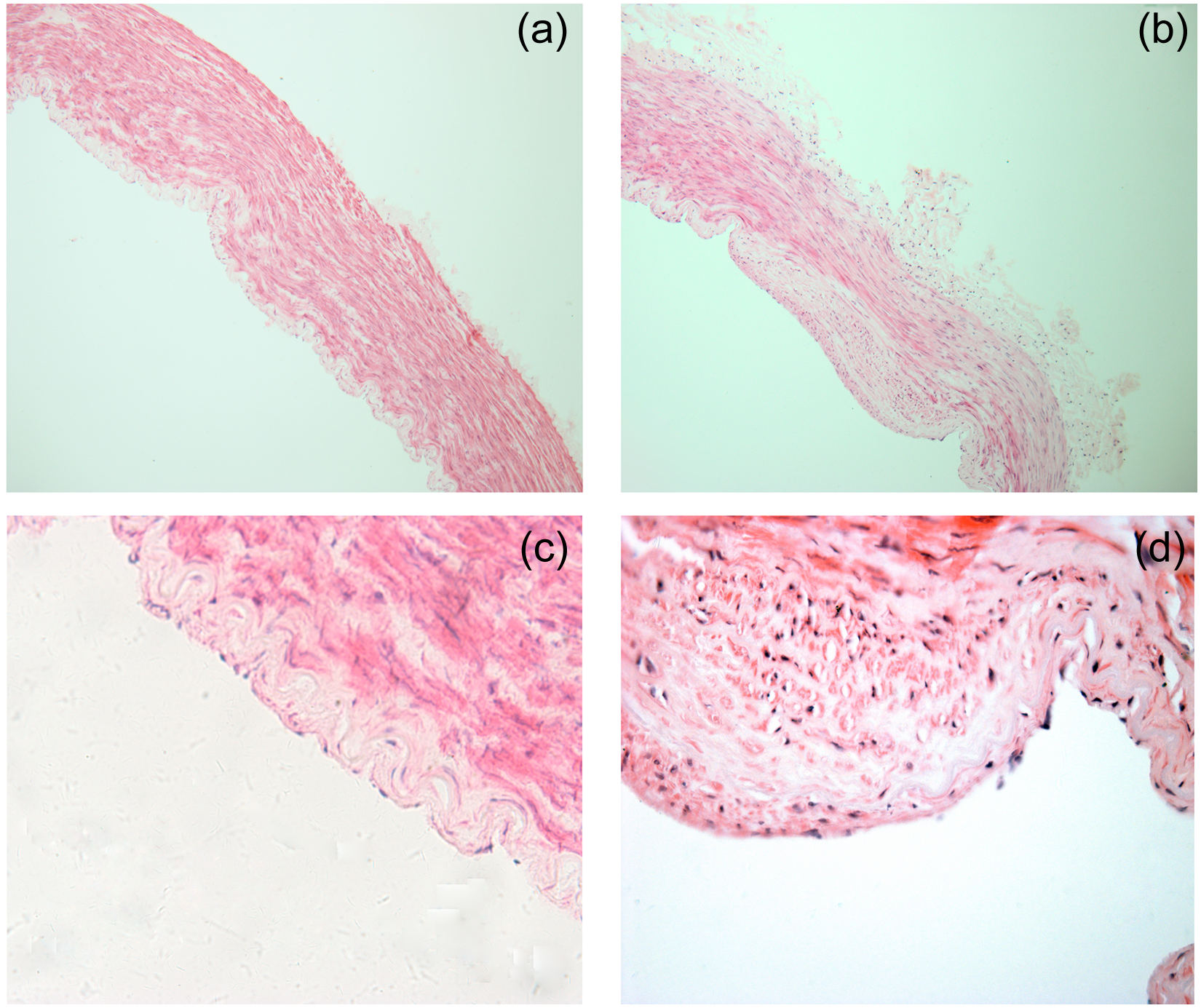
(a and c) The intima of RA in the non-diabetic patient was intact and thin with flattened endothelial cells aligned along the axis of the artery. (Haematoxylin–eosin; (a): original magnification, ×100; (c): original magnification, ×400). (b and d) The intima of RA in the diabetic patient exhibited intimal thickening, and foam cells are present. (Haematoxylin–eosin; (b): original magnification, ×100; (d): original magnification, ×400).
Comparison of indices of severity of intimal hyperplasia in the radial artery.
DM: diabetes mellitus; LN: luminal narrowing; ITI: intimal thickness index; IMR: intima:media ratio.
TEM
In the non-DM group, endothelial cells were arranged towards the intima and were elliptical in shape, with a round nucleus and sparse homogeneous chromatin. Vascular smooth muscle cells (SMCs) were arranged towards the tunica media and were spindle shaped, with a long, thin, elliptical nucleus and sparse homogeneous chromatin. Myofilaments could be visualized in the cytoplasm of SMCs.
Endothelial and subendothelial oedema was significantly greater in the DM group than in the non-DM group. Discontinuities were seen in the endothelial layer of the DM segments. Swelling was present in all cytoplasmic mitochondria. Foam cells and a tendency for SMCs to move to the intima were seen in DM RA segments (Figure 2).
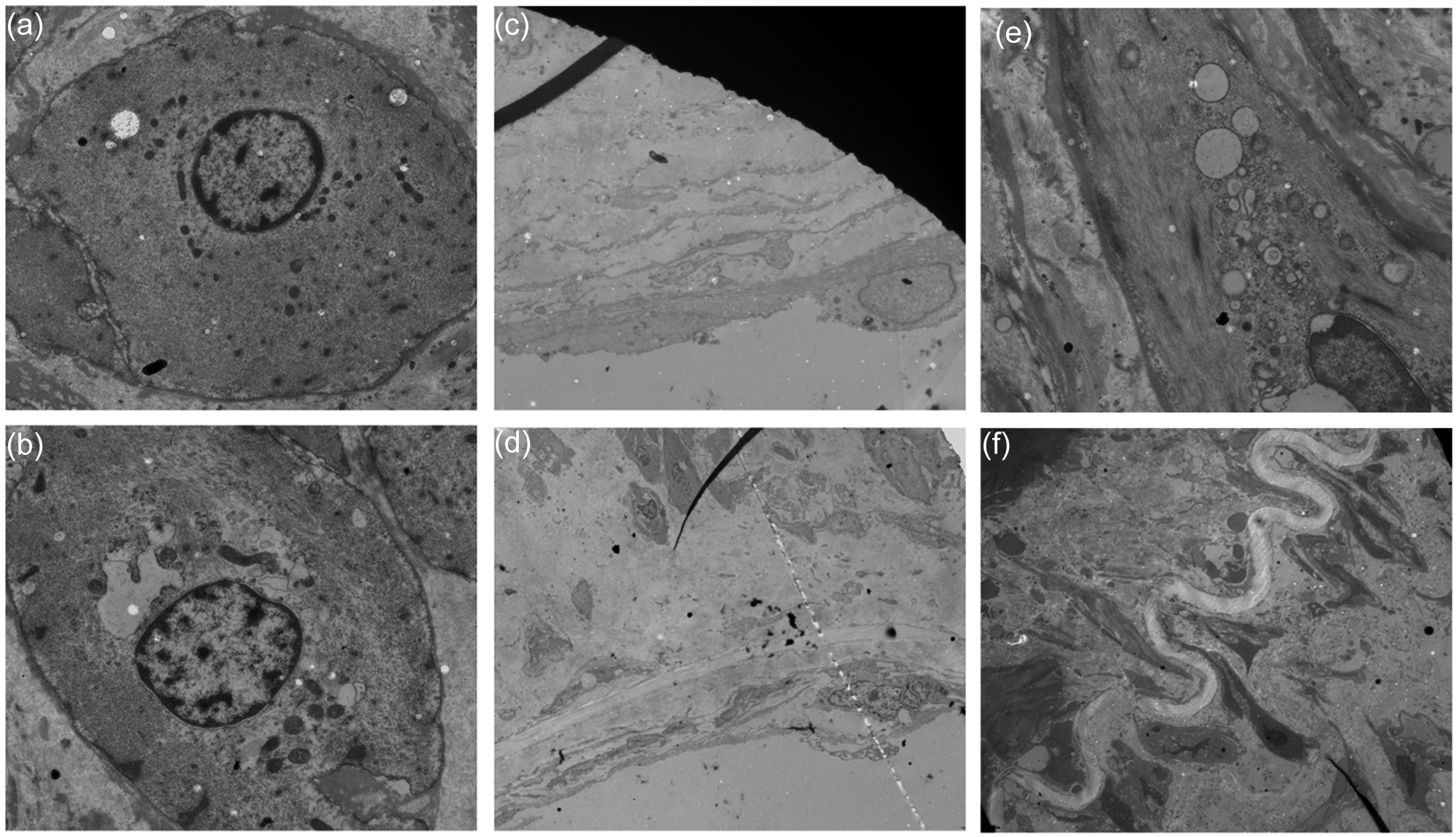
(a) Non-diabetic patients: The vascular SMCs arranged towards tunica media with spindle shape, with its nucleus elliptic, long and thin. The chromatin of SMC was sparse and homogeneous. Myofilaments could be visualized in the cytoplasm of SMC (original magnification ×700). (b) Diabetic patients: swelling was present in the cytoplasmic mitochondria (original magnification ×700). (c) Non-diabetic patients: endothelial cells arranged towards intima with elliptical shape, with its nucleus round in shape and its chromatin sparse and homogenous (original magnification ×700). (d) Diabetic patients: endothelial oedema and cytoplasmic mitochondrial swelling were present (original magnification ×700). (e) Diabetic patients: lipid is present in the cytoplasm of vascular SMC (original magnification ×1000). (f) Diabetic patients: the tendency of SMCs moving to intima could be visualized (original magnification ×1000).
The results of semi-quantitative electron microscope evaluation are shown in Table 4. Total scores were lower in the non-diabetic group than in the diabetic RAs (1.38 ± 0.2 vs 4.53 ± 0.3, t = 27.63, p < 0.001).
Mean electron microscopy scores.
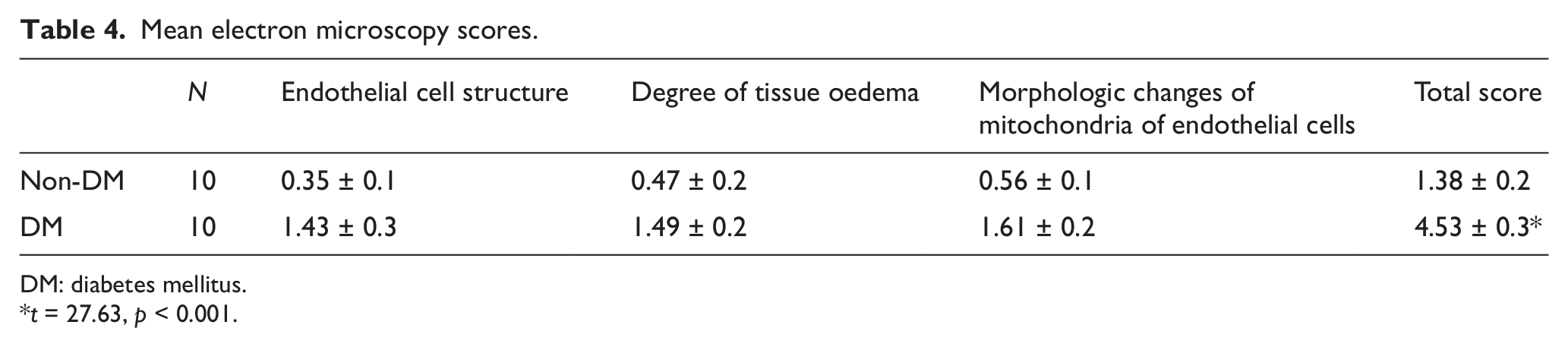
DM: diabetes mellitus.
t = 27.63, p < 0.001.
Western blot analysis
Western blot analysis showed that eNOS expression was higher in the non-DM group than in the DM group (Figure 3(a) and (b)). The relative integral optical density of eNOS protein was significantly higher in non-DM patients than in DM patients (1.33 ± 0.25 vs 0.54 ± 0.10, t = 9.82, p < 0.001) (Figure 3).
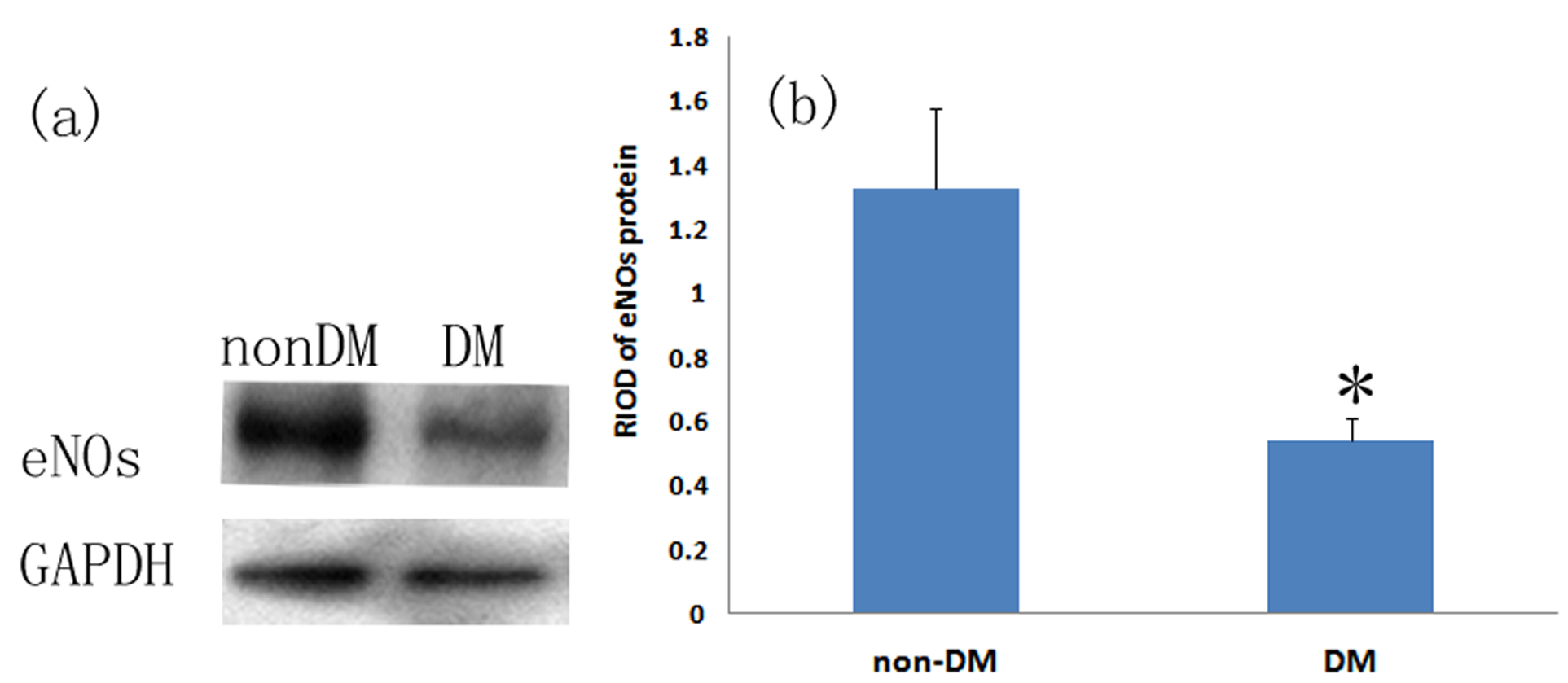
(a) Determination of eNOS expression in diabetic and non-diabetic RA by Western blot analysis. (b) Relative integral optical density of eNOS protein in diabetic and non-diabetic RA. Non-DM, n = 10; DM, n = 10. *t = 9.82, p < 0.05 vs non-DM group.
Semi-quantitative RT-PCR
For the vWF gene, the difference in ΔCT between DM and non-DM samples was significant (t = 5.14, p = 0.006807). The difference was also significant for the ET-1 gene (t = 9.81, p = 0.000780). Expression of both vWF and elongation factor-1 (EF-1) mRNA was notably higher in the DM group than in the non-DM group (Figure 4).
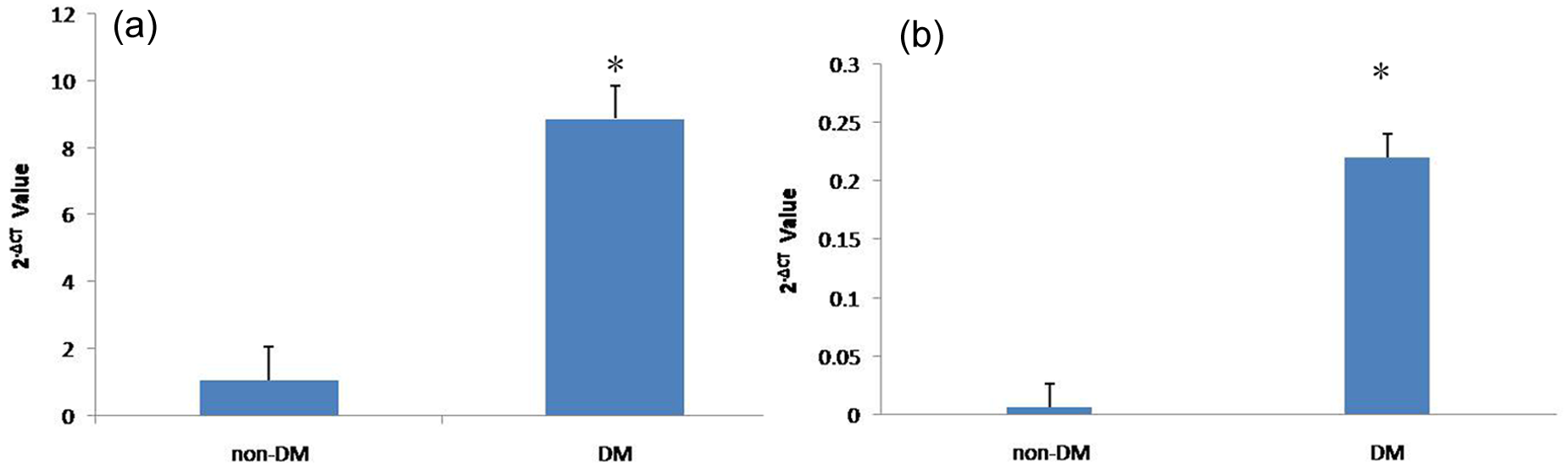
(a) vWF mRNA expression normalized to β-actin mRNA in radial artery from diabetic and non-diabetic patients. Expression of vWF mRNA was notably higher in diabetic patients than in non-diabetic patients. *pΔCT < 0.05 versus non-DM group. (b) ET-1 mRNA expression normalized to β-actin mRNA in radial artery diabetic and non-diabetic patients. Expression of ET-1 mRNA was notably higher in diabetic patients than in non-diabetic patients. *pΔCT < 0.05 versus non-DM group.
Discussion
Use of the RA as a conduit in CABG was introduced in the early 1970s. 9 It was soon abandoned because of early graft occlusion, 10 but is now used widely following the study of Acar et al., 11 which showed that RA remained patent after 15 years. The patency rate of RA conduits at 5 years is approximately 85% 1 supporting its long-term use in CABG.
DM increases the risk of developing coronary artery disease by two-fold to six-fold. 12 There are many reports8,13,14 on CABG conduit options and the subsequent clinical course for diabetic patients. However, little is known about the status of the RA in patients with DM.
In the present study, two arterial abnormalities were found: intimal hyperplasia and atherosclerosis. Atherosclerosis is caused by excessive lipoprotein in the plasma that accumulates preferentially in the hyperplastic intima. 15 Severe intimal hyperplasia was seen in most of the RA samples removed from diabetic patients undergoing CABG. The propensity of the RA to develop intimal hyperplasia and atherosclerosis was evaluated by three means: LN, ITI and IMR. LN is a measure of the severity of intimal thickening, ITI compares intimal disease between different vascular beds8,16,17 and IMR is used to compare the same artery between different patients. 8 Chowdhury et al. 18 considered early graft occlusion to be attributable to intimal hyperplasia, and several investigators have indicated that age, smoking and DM are all correlated with intimal hyperplasia and atherosclerosis in the RA. In our study, diabetic and non-diabetic patients were matched with regard to age and smoking history. About 26.7% (8/30) of RAs from diabetic patients were found to be normal in structure, compared with 76.7% (23/30) of those from non-diabetic patients (µ = 3.62, p = 0.000298), indicating that intimal hyperplasia and atherosclerosis occur more commonly in individuals with DM. Mean IMR and ITI were statistically significantly greater in the diabetic patients than in the non-diabetic patients. It is suggested that disease of the RA is more severe and common in DM. Preoperative Doppler ultrasonography performed to exclude obvious stenosis showed no obvious difference in LN.
When the integrity of the endothelium is compromised, the exposed subendothelial structures attract platelet adhesion and aggregation to form thromboses with subsequent inflammatory and immune responses, resulting in intimal hyperplasia and atherosclerosis, and causing vascular stenosis and occlusion. Thus, the integrity of the endothelium is important for the clinical outcome of patients. Van Son et al. 19 reported that discontinuities and greater numbers of SMCs in the internal elastic lamina of the RA stimulated early and progressive intimal hyperplasia. In our study, discontinuities were more common in the endothelium of diabetic RAs. This may indicate a higher rate of graft failure or occlusion in patients with DM.
The endothelium plays an important role in vascular tone, regulating the production of vasodilator molecules such as nitric oxide (NO) and vasoconstrictors. 20 Endogenous NO as a vascular relaxant factor released from endothelial cells plays a principal role in the relaxation of vascular smooth muscle and the dilation of blood vessels. eNOS is the only rate-limiting enzyme in the NO synthesis pathway, determining the level of NO expression. Broeders et al. 21 confirmed that eNOS expression in the arterial conduit had an impact on the long-term patency. Semi-quantitative electron microscopy shows higher total scores in the diabetic RAs, which suggests endothelial cell damage was more severe in diabetic patients. In the present study, the abnormalities of intima and media including subintimal oedema, swollen mitochondria and perinuclear oedema, which were shown in DM group with TEM may impair the vasoreactivity of arterial conduits and in turn affect the long-term outcomes of patients. In order to better understand the damage to the vasoreactivity of RAs, the expressions of eNOS, ET-1 and vWF, signs of vascular endothelial cell injury, were examined. By Western blot, eNOS protein expression was found to be higher in the non-diabetic group than in the diabetic group. This indicates that, in patients with DM, the endothelium of the RA might not be able to produce sufficient NO to prevent leukocyte adhesion, maintain the endothelium in a quiescent and anti-inflammatory state 20 and stop vasospasm as a major vasorelaxant in the human vasculature. 22
vWF is a glycoprotein that is synthesized in the vascular endothelial cells and binds to coagulation factor VIII. 23 In the blood, it mediates platelet adhesion and aggregation to initiate thrombosis, and an increase of vWF is considered a sign of vascular endothelial cell injury. ET-1 is a powerful endogenous vasoconstrictor that influences the contraction of blood vessels and the proliferation of vascular SMCs. Both of these are balanced by the production of NO. 24 In addition, Choudhary et al. 14 demonstrated that the RA of diabetic patients is more prone to spasm in response to endogenous vasoconstrictors such as ET-1. Although the levels of ET-1 and vWF associated with endothelial dysfunction are increased in patients with DM, 25 it was unknown whether the same situation occurred in the RA of diabetic patients. In the present study, the high expression of ET-1 and vWF mRNA in the RA of diabetic patients implies that levels of EF-1 and vWF might be increased in RA plasma, leading to a higher incidence of postoperative RA spasm and occlusion. We hypothesize that the decreased relaxant ability of the RA in diabetic patients, accompanied by the increased propensity to contractility, may lead to postoperative RA spasm with poor long-term patency. The results are consistent with our previous findings. 4
In conclusion, we have confirmed that, in CABG patients with DM, RA conduits exhibit pre-existing disease, with intimal hyperplasia, endothelial cell injury and endothelial dysfunction that might be responsible for graft occlusion and spasm. Greater care should be taken when selecting RA as an arterial graft in DM patients. It is also necessary and important to strictly control blood glucose levels in CABG patients receiving an RA graft.
Study limitations
The principal limitation of this study is the small sample size. Another limitation is that intimal hyperplasia and atherosclerosis are both segmental diseases, so the extent of disease in one section of the RA may not necessarily represent the condition of the entire vessel. 18
Footnotes
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by a grant from the Chinese Natural Science Fund (81070180).