
Abstract
The single nucleotide polymorphisms (SNPs) in the gene of breast cancer suppressor protein (BRCA1)–associated protein (BRAP) are significantly associated with coronary artery disease, but the molecular mechanisms are not understood. We examined the associations of the SNPs (rs11066001 and rs3782886) in BRAP with metabolic syndrome (MetS), which is a strong predictor of cardiovascular disease, and potential associations between these SNPs and factors related to inflammation. There were significant associations of both the SNPs with MetS [rs11066001, odds ratio (OR) 0.70, 95% confidence interval (CI) 0.51–0.96, p = 0.028; rs3782886, OR 0.69, 95% CI 0.50–0.94, p = 0.020] under a dominant model after age and gender adjustment. Both SNPs were significantly associated with waist circumference, plasma glucose, glycated haemoglobin, triglycerides and nonesterified fatty acid. Our data provide evidence that the SNPs (rs11066001 and rs3782886) in BRAP decrease the risk of MetS, and associations of the SNPs with various components of MetS are different. Moreover, there are significant associations of both the SNPs with nonesterified fatty acid that could be involved in the inflammatory activity of electronegative low-density lipoprotein.
Keywords
Introduction
The metabolic syndrome (MetS) is a cluster of cardiovascular risk factor and metabolic abnormalities that include abdominal obesity, elevated triglycerides, reduced high-density lipoprotein (HDL) cholesterol, raised blood pressure and elevated plasma glucose. 1 The MetS is highly prevalent,2,3 and the presence of the syndrome is a strong predictor of cardiovascular disease.4–7 In addition, individuals with the MetS are at significantly increased risk of incident type 2 diabetes mellitus that is an important risk factor for cardiovascular disease.8,9 It deserves more clinical attention that detecting MetS in asymptomatic individuals as a multiplex risk factor for cardiovascular disease.10,11
Breast cancer suppressor protein (BRCA1)–associated protein (BRAP) was observed in macrophages and smooth muscle cells in atherosclerotic lesions 12 and could influence nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) as a central mediator of inflammation.12,13 The single nucleotide polymorphisms (SNPs) in BRAP were significantly associated with coronary artery disease in Asian populations.12,14 Hsu et al. 15 reported that the SNP (rs11066001) in BRAP has a synergistic effect with diabetes in the Chinese population.
Plasma nonesterified fatty acid (NEFA) concentrations are elevated in obese adults and are related to reductions in insulin sensitivity.16,17 Fatty acid metabolism is disturbed and NEFA is increased in type 2 diabetic participants.18,19 Some studies indicate that NEFA could be involved in the inflammatory activity of electronegative low-density lipoprotein (LDL) cholesterol. 20 However, whether BRAP is associated with NEFA and MetS has not been studied in the Chinese population.
We have previously conducted a prospective study of blood pressure in Chinese children and adolescents, namely, the Beijing Child Blood Pressure Study (BBS), in 1987. This study is an on-going, population-based, follow-up study of blood pressure. We investigated the associations between the SNPs (rs11066001 and rs3782886) in BRAP with MetS and different components of MetS, and also potential associations between these SNPs and factors related with inflammation in the cohort. The present study attempts to provide an analysis of epidemiological and genetic data towards the possible mechanism of the role of BRAP in cardiovascular diseases.
Methods
Study population
BBS is an on-going, population-based, prospective, follow-up study of blood pressure in Beijing children and young adults. The baseline study in 1987 included 5916 children and adolescents, aged 3–18 years. Baseline data included weight, height, heart rate, blood pressure and left subscapularis skinfold. In 2005, 412 adult participants of the study underwent clinical examinations, which included electrocardiogram, echocardiography, fundus examination and biochemical detection. The latest follow-up study was conducted from 2010 to 2011, with 1190 subjects attending anthropometric measurement and medical examination. Participants were asked to complete questionnaires that included questions about smoking habits, drinking habits, whether suffer from coronary heart disease or stroke and physical activities. In addition, venipuncture blood samples were collected. We obtained written informed consent from all participants. The BBS study was approved by the ethics committees of the Capital Institute of Paediatrics.
Measurement of anthropometric parameters and biochemical analyses
Anthropometric measurement included weight, height, waist circumference and fat mass percentage by a body composition analyzer (TBF-300A, TANITA Inc., Tokyo, Japan). All instruments were validated following the standard methods of the manufacturers. 21 Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters. Waist circumference was measured midway between the lowest rib and the superior border of the iliac crest at the end of normal expiration with an inelastic measuring tape to the nearest 0.1 cm. Abdominal obesity was diagnosed by waist circumference (90 cm for male, 85 cm for female).
Total cholesterol, triglycerides, HDL, LDL, fasting plasma glucose (FPG), 2-hour oral glucose tolerance test glucose level (OGTT), glycated haemoglobin (HbA1C) and NEFA were analyzed by an automatic biochemical analyzer (Hitachi 7020, Hitachi Ltd, Tokyo, Japan) using a kit assay (SEKISUI Medical technology Ltd, Tokyo, Japan).
Measurement of blood pressure
Blood pressure was measured by auscultation using a standard clinical sphygmomanometer. Measurements were taken on the right arm in a sitting position with the elbow at the level of the right atrium, using an appropriately sized cuff. Systolic blood pressure (SBP) was determined by the onset of the ‘tapping’ Korotkoff sounds (K1) and diastolic blood pressure (DBP) was determined by the fourth Korotkoff sound (K4). Three consecutive measurements were taken and the mean of the three readings was used for analysis. Hypertension was defined as participants having current or past anti-hypertensive medication, SBP ≥ 140 mmHg, or DBP ≥ 90 mmHg.
Genotyping
The SNPs (rs11066001 and rs3782886) in BRAP were selected to investigate for the following: (a) they were significantly associated with myocardial infarction, (b) they were likely to be present only in Asian populations according to HapMap data (http://hapmap.ncbi.nlm.nih.gov/) and (c) the transcriptional regulatory activities of these SNPs were demonstrated.
Genomic DNA was extracted from peripheral blood white cells using QIAamp® DNA Blood Mini Kit, according to the instructions of the manufacturer (QIAGEN Inc., Valencia, CA, USA). SNPs were genotyped by TaqMan 22 Allelic Discrimination Assays with the GeneAmp 7900 Sequence Detection System (Applied Biosystems, Foster City, CA, USA). TaqMan probes were used for genotyping rs11066001 (C_31115184_10) and rs3782886 (C_25810215_10). Genotyping call rates for both SNPs were greater than 98%. In order to validate the accuracy of genotyping, we sent 30 samples to direct sequencing and observed 100% concordance between the two genotyping methods.
Statistical analysis
Continuous variables were presented as mean ± standard deviation (SD) or geometric mean ± quartile deviation, and categorical variables were presented as percentages. Hardy–Weinberg equilibrium was assessed using the chi-square test. For the dominant model, we divided the population into two groups according to the different genotypes (for rs11066001, the group with CT and CC compared with the group with TT; for rs3782886, the group with AG and GG compared with the group with AA). Analysis of covariance (ANCOVA) was used to calculate mean differences in waist circumference, FPG, OGTT, HbA1C, NEFA and LDL according to genotypes with age and gender adjustment. Odds ratios (ORs) for MetS were calculated by a multiple logistic regression with genotypes, age and gender as the independent variables. ANCOVA was also used to calculate mean differences in SBP and DBP according to genotypes, with age, gender and BMI as covariates. Data were analyzed using SPSS statistical software (version 13.0; SPSS Inc., Chicago, IL, USA). p < 0.05 was used to indicate statistically significant differences. Power calculation was performed using Quanto software (http://hydra.usc.edu/gxe/).
Results
A total of 1190 participants were recruited in the latest follow-up study and had DNA samples available. The characteristics of the study participants are summarized in Table 1. The participants with MetS were 299. The clinical identification of participants with the features of MetS was based on the modified criteria proposed by the National Cholesterol Education Program–Adult Treatment Panel III (NCEP-ATPIII). 23 Criteria for clinical diagnosis of the MetS are provided in supplementary Table 1.
Basic characteristics of participants in this study.

HDL: high-density lipoprotein; LDL: low-density lipoprotein cholesterol; FPG: fasting plasma glucose; OGTT: 2-hour oral glucose tolerance test glucose level; NEFA: nonesterified fatty acid; SD: standard deviation.
Values are means (SDs), geometric mean (quartile deviation) or percentages of subjects, as appropriate.
We genotyped the SNPs (rs11066001 and rs3782886) in BRAP in the cohort and the SNPs were tested to be in Hardy–Weinberg equilibrium (p = 0.08 and 0.10, respectively). Associations of the SNPs with various components of MetS are shown in Tables 2 and 3. There were significant associations of rs11066001 and rs3782886 with waist circumference (p = 0.020 and 0.007, respectively) and abdominal obesity (rs11066001, OR 0.72, 95% confidence interval (CI) 0.54–0.96, p = 0.024; rs3782886, OR 0.69, 95% CI 0.52–0.91, p = 0.010) under a dominant model after age and gender adjustment. Associations of SNPs in BRAP with glucose metabolism and triglycerides are shown in Table 2. Both SNPs are significantly associated with FPG, OGTT, glycated haemoglobin and triglycerides. However, there was no statistically significant difference between the two SNPs and HDL.
Associations of rs11066001 and rs3782886 with clinical parameters.

FPG: fasting plasma glucose; GTT: 2-hour oral glucose tolerance test glucose level; HDL: high-density lipoprotein; SBP: systolic blood pressure; DBP: diastolic blood pressure; NEFA: nonesterified fatty acid; BMI: body mass index; SD: standard deviation.
Under dominant model: Population are divided into two groups according to the different genotypes (for rs11066001, the group with CT and CC compared with the group with TT; for rs3782886, the group with AG and GG compared with the group with AA).
Adjusted for age and gender.
Adjusted for age, gender and BMI. Waist circumference, FPG, GTT, glycated haemoglobin, HDL, SBP, DBP and NEFA are expressed as means (SDs). Triglycerides are geometric mean (quartile deviation).
Associations of rs11066001 and rs3782886 with hypertension, abdominal obesity and metabolic syndrome.
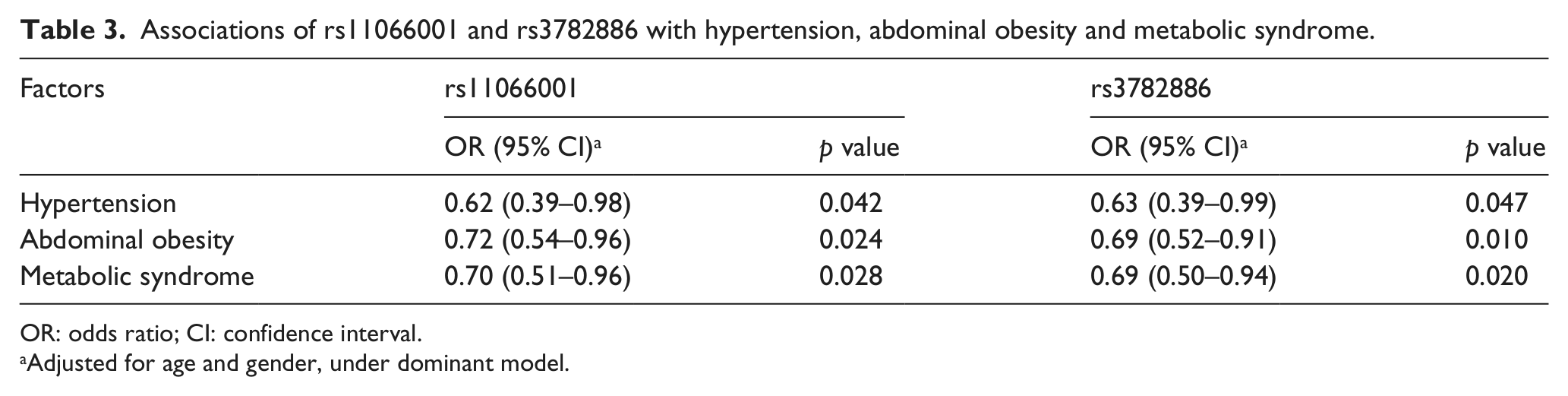
OR: odds ratio; CI: confidence interval.
Adjusted for age and gender, under dominant model.
Table 2 also shows associations of SNPs in BRAP with NEFA. Adjusted for age and gender, there were significant associations of rs11066001 and rs3782886 with NEFA (p = 0.010 and p = 0.011, respectively) under a dominant model.
Associations of the SNPs with MetS are shown in Table 3. Adjusted for age and gender, there were significant associations of rs11066001 and rs3782886 with MetS (rs11066001, OR 0.70, 95% CI 0.51–0.96, p = 0.028; rs3782886, OR 0.69, 95% CI 0.50–0.94, p = 0.020) under a dominant model.
Discussion
In this study, we examined the SNPs (rs11066001 and rs3782886) in BRAP in the Chinese young adult population. Our results indicate that both SNPs decrease the risk of MetS (Table 3). Associations of the SNPs in BRAP with various components of MetS were different. Moreover, there were significant associations of both SNPs with NEFA (Table 2).
However, there was no statistically significant difference between the two SNPs in BRAP and HDL (Table 2). With the assumed effect size (regression coefficient) of −0.004 and −0.009 for allele frequencies of 0.167 and 0.144, the power for the rs11066001 and rs3782886 was 0.056 and 0.076, respectively. This could be attributable to the small sample size in our study. Studies with greater sample sizes are needed to examine the SNPs with HDL to clarify the associations.
Associations of the SNPs (rs11066001 and rs3782886) in BRAP with SBP, DBP and hypertension are shown in Tables 2 and 3. It is not clear why the mean SBP or DBP of samples with heterozygous genotype is lowest in whole samples. A replicated study is necessary in other populations.
MetS was identified as a multiplex risk factor for cardiovascular disease by the NCEP-ATPIII. 1 The presence of MetS increases the risk of cardiovascular events4–7 and type 2 diabetes mellitus8,9 and hence deserves more clinical attention. The etiology of MetS is related to defects in several homeostatic regulatory systems, and the molecular mechanism is not clear.
Earlier studies showed that the expression of BRAP was observed in macrophages and smooth muscle cells in atherosclerotic lesions, 12 and BRAP activated inflammatory cascades by regulating NF-κb. 24 BRAP is located on chromosome 12q24 in humans. According to HapMap data, the SNPs (rs11066001 and rs3782886) in BRAP are likely to be present only in Asian populations. rs11066001 (lies in intron 3) and rs3782886 (lies in exon 5) do not cause amino acid substitutions, but reduce the transcriptional activity of the gene. 12 rs11066001 is in very strong linkage disequilibrium (LD) with rs3782886, but these SNPs lie in different domains of BRAP, and the effects of these SNPs to reduce the transcriptional activity of the gene are different. 12 Therefore, we examined both the SNPs in our study. Novel studies reported that the SNP (rs11065987) in BRAP is associated with MetS in European Americans and African Americans. 25 Replicated studies should be carried out in other populations.
Some studies reported that the SNPs (rs11066001 and rs3782886) in BRAP were significantly associated with coronary artery disease in Asian populations.12,14 However, the mechanism of the role of BRAP in cardiovascular disease is not clear. In the current study, the associations between the SNPs (rs11066001 and rs3782886) in BRAP and MetS and different components of MetS were found in the Chinese Han population, and the results showed first that the SNPs are associated with NEFA that could be involved in the inflammatory activity of electronegative LDL. 20 Our results suggest that BRAP is involved in MetS, and the contributions to various components of MetS are different.
Ozaki et al. 12 also computed associations between the SNPs in BRAP and diabetes, hypertension and hyperlipidaemia, which are components of the MetS. They found no significance between these parameters in the Taiwanese population. Taiwanese and our study population are both of Asian descent and have similar genetic background, and thus the inconsistent results between the two populations could be attributed to the differences in study population enrolment, sample size and gene–gene/environment interactions.
In conclusion, we demonstrate for the first time that the SNPs (rs11066001 and rs3782886) in BRAP are associated with MetS, which is considered as a risk factor for cardiovascular disease, and NEFA, which is related to inflammatory activity of electronegative LDL in Chinese Han population. These novel findings provide important evidence that BRAP possibly mediates the process of MetS involved in cardiovascular disease.
Footnotes
Acknowledgements
We gratefully acknowledge the contributions of data collection team and the individuals who participated as both children and adults in this prospective study. We thank the laboratory of human genetics of the Beijing Hypertension League Institute for providing the genotyping facilities for this work. We also thank Ping Yang (Department of Epidemiology, Capital Institute of Paediatrics, Beijing, China) for the excellent work of blood samples collection.
Conflict of interest
The authors have no conflicts of interest.
Funding
This study was supported by the National ‘Twelfth Five-Year’ Plan for Science & Technology Support Programme (grant no. 2012BAI03B03), the Beijing Natural Science Foundation (grant no. 7112018), the Beijing Key Science and Technology Programme (grant no. D111100000611002), the National Natural Science Foundation of China (grant no. 81172746) and the Beijing Training Project for the Leading Talents in S & T (grant no. 2011LJ07).