
Abstract
Metabolic syndrome (MetSyn) increases the risk of cerebrovascular disease and stroke; however, its impact on human cerebral circulation remains unclear. Reduced cerebral dilation is also associated with an increased risk of stroke and may occur in MetSyn adults. We hypothesised that MetSyn adults would exhibit reduced cerebral vasodilation to hypoxia and hypercapnia. Middle cerebral artery velocity (MCAv) was insonated with Doppler ultrasound in younger (approximately 35 years) MetSyn and healthy adults. We measured mean arterial blood pressure (MABP), arterial oxygen saturation (SpO2) and end tidal carbon dioxide (P
Introduction
Metabolic syndrome (MetSyn) is a multi-component condition that increases an individual’s relative risk of developing cardiovascular disease,1–3 including stroke. 4 However, the impact of MetSyn on human cerebral vessel function has not been examined.
Proper cerebral blood flow regulation is critical for maintaining the homeostatic environment of the brain. Blunted dilation (cerebrovascular reactivity) to challenges such as hypoxia or hypercapnia is associated with an increased risk of stroke.5–7 Dilation to hypoxia or hypercapnia is clinically important, as these stimuli occur in sleep disordered breathing and acute ischaemic stroke.
Given the elevated incidence 4 and possible severity 8 of stroke in MetSyn, it is important to understand cerebrovascular pathophysiology to reduce the risk, incidence and severity of stroke in this rapidly expanding population. No literature has addressed the key gap in knowledge of whether impaired vascular regulation is present prior to the clinical manifestation of disease. In older adults with atherosclerosis, MetSyn is an independent predictor of impaired cerebral dilation, 9 a finding that is not surprising given the combination of advanced age and presence of disease. In contrast, virtually nothing is known about the onset and progression of cerebrovascular disease in younger adults with MetSyn. Early detection of vascular dysfunction could allow for medical and lifestyle interventions to slow or reverse disease progression and have important benefits for stroke outcomes.
The purpose of this study was to test the hypothesis that younger adults with MetSyn would display blunted cerebral vasodilator responses during hypoxia and hypercapnia compared to healthy controls. We studied younger adults to investigate the influence of MetSyn on cerebrovascular function prior to the onset of clinically overt metabolic and cardiovascular disease.
Methods
Subjects
Nine adults with metabolic syndrome (MetSyn, 37±3 years, two female) and ten healthy adults (32±2 years, four female) participated in this study. Health history and physical activity were assessed by questionnaires. Subjects were not taking any cardiovascular medications and were free of cardiovascular, cerebrovascular, metabolic, pulmonary and neurologic disease. One subject with MetSyn reported sleep-disordered breathing. All subjects were sedentary (<60 minutes of moderate-intensity aerobic exercise per week) and did not use any tobacco. Females had a regular menstrual cycle (oral contraception allowed), were studied during the early follicular phase of their menstrual cycle (day 1–5) and were not pregnant (urine test). Subjects reported to the laboratory after fasting for 10 hours and abstaining from heavy exercise, alcohol, caffeine and NSAIDs for 24 hours.
Adults with MetSyn were categorised based on the NCEP-ATP III definition of MetSyn, as modified by the American Diabetes Association and International Diabetes Federation. 1 Healthy controls were lean, normotensive, normolipidaemic and normoglycaemic. All procedures performed for this project obeyed the Declaration of Helsinki and were approved by the University of Wisconsin-Madison Institutional Review Board. Written informed consent was obtained from each subject.
Measurements
Height and weight were measured and body mass index (BMI) (kg/m2) was calculated. Venous blood was analysed for glucose and lipids for confirmation of MetSyn. Subjects were instrumented for continuous monitoring with a 3-lead electrocardiogram (heart rate, HR), automatic sphygmomanometer (mean arterial blood pressure, MABP) and pulse oximeter (arterial oxygen saturation, SpO2) (Datex-Ohmeda, Helsinki, Finland).
Middle cerebral artery blood velocity (MCAv) was collected using a 2 MHz probe (Neurovision model 500M, Multigon Industries, Inc., Yonkers, New York, USA) placed in the temporal window using standard search criteria.
10
The Doppler probe was held in place by an adjustable headband. Minute ventilation (VE) and inspired oxygen fraction were measured with a metabolic cart (MedGraphics, Ultima PFX, St. Paul, Minnesota, USA). End-tidal carbon dioxide (P
Protocol
Hypoxia and hypercapnia trials were performed in randomised order with the subjects in a semi-recumbent position. Each hypoxia and hypercapnia trial was followed by ten minutes of room air breathing, providing sufficient time for all variables to return to baseline levels.
Isocapnic hypoxia was achieved by subjects breathing through a mouthpiece while nasal air flow was occluded. The mouthpiece was attached to a two-way non-rebreathing valve (2700 Series, Hans Rudolph Inc., Kansas City, Missouri, USA) connected to a gas mixer to control inspired air composition. Following five minutes of room air breathing, inspired oxygen was titrated to maintain five minutes of steady state SpO2 at 90% followed by transition to five minutes of SpO2 at 80%. To isolate the effects of hypoxia, baseline P
Hyperoxic hypercapnia was performed by subjects breathing through a mouthpiece connected to a three-way sliding valve (Model 2870, Hans Rudolph Inc., Kansas City, Missouri, USA) while wearing a nose clip. The mouthpiece was connected to a meteorological balloon filled with a hyperoxic (to isolate the effects of hypercapnia), hypercapnic mix of gas (CO2=3%, O2=40%, N2=57%) to a volume one litre above predicted vital capacity based on age and height. After five minutes of room air breathing, subjects began to rebreathe air from the balloon. Trials were terminated when the subject’s P
Data analysis
Data were recorded using PowerLab suite (ADinstruments, Colorado Springs, Colorado, USA). The last 30 seconds of baseline and steady state data from each hypoxia level were averaged from each trial. For hypercapnia trials, the last 30 seconds of baseline data and the last 10 seconds of hypercapnia were averaged to examine the peak response to the stimulus.
MCAv values were normalised for perfusion pressure and are presented as cardiovascular conductance indices (CVCi = MCAv*100/MABP). Cerebral vasodilation was defined as a positive change of CVCi (ΔCVCi) from baseline, since a change of conductance has a predictable relationship with vasodilation.
12
Vascular reactivity slopes to hypoxia and hypercapnia were calculated as ΔCVCi/ΔSpO2 and ΔCVCi/ΔP
Minitab 15 (State College, Pennsylvania, USA) was used for statistical analysis. Subject characteristics were compared with an unpaired t-test analysis. Hypoxia and hypercapnia data were analysed using a general linear model to perform an analysis of variance (ANOVA). Significance was set at p<0.05 for all statistical tests.
Results
Subject characteristics and sex ratios are summarised in Table 1. Subjects were similar in age and height. By design, adults with MetSyn had significantly higher weight, BMI, waist circumference, blood pressure, and lower high density lipoprotein (HDL) than healthy controls (p<0.05). Insulin concentration was also greater in adults with MetSyn (p<0.05). Plasma triglyceride concentration tended to be higher in adults with MetSyn (p=0.08). Of the adults with MetSyn, eight met the criterion for waist circumference, one for plasma glucose, six for HDL, three for triglycerides, and nine for blood pressure. None of the healthy adults met any of the criteria for MetSyn.
Subject characteristics.
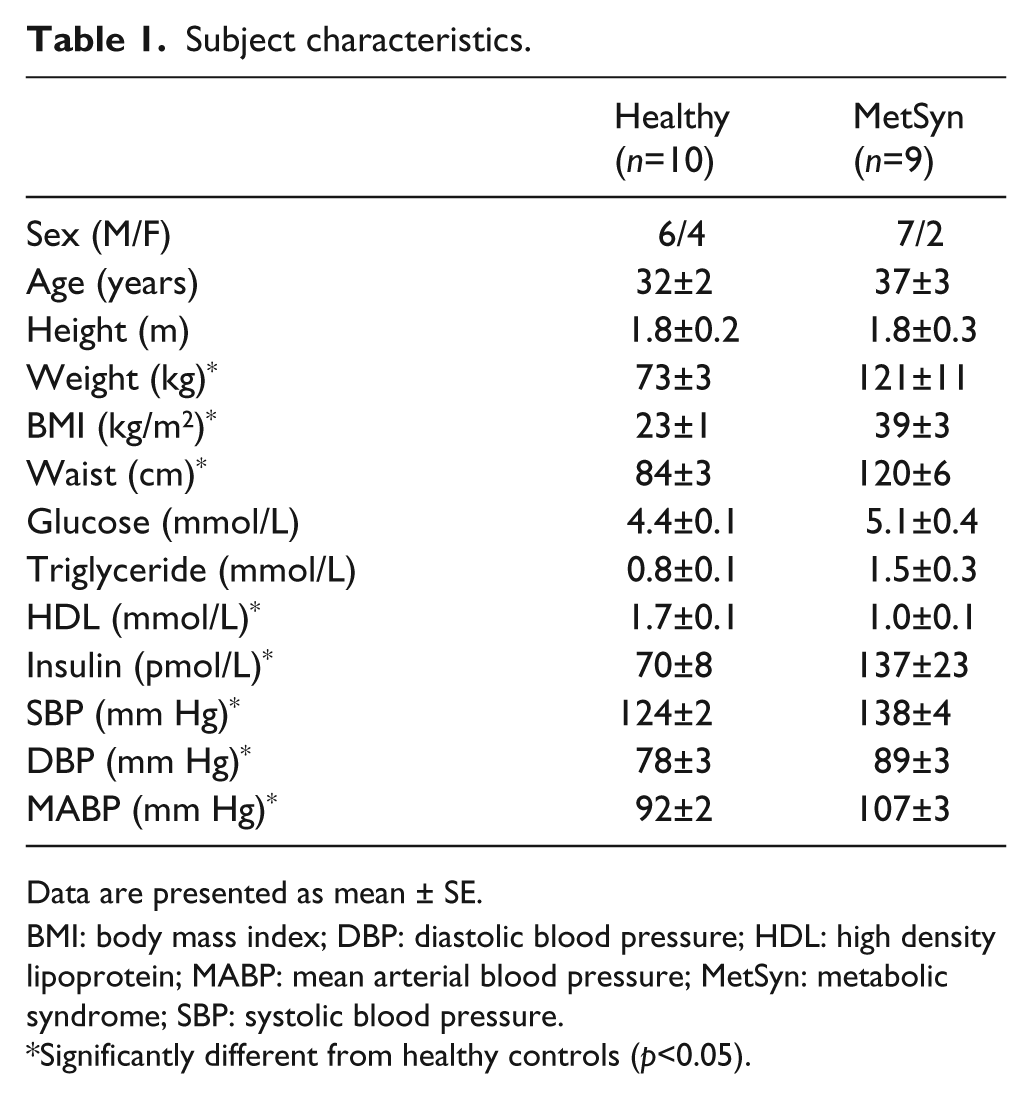
Data are presented as mean ± SE.
BMI: body mass index; DBP: diastolic blood pressure; HDL: high density lipoprotein; MABP: mean arterial blood pressure; MetSyn: metabolic syndrome; SBP: systolic blood pressure.
Significantly different from healthy controls (p<0.05).
Systemic responses to hypoxia
Systemic haemodynamic values are summarised in Table 2. Heart rate increased at 80% SpO2 (p<0.05) and did not differ between groups. MABP was greater in adults with MetSyn (p<0.05) but did not change in either group with hypoxia. By design, SpO2 was reduced with hypoxia (p<0.05) similarly between groups. P
Systemic and cerebral responses to hypoxia and hypercapnia.
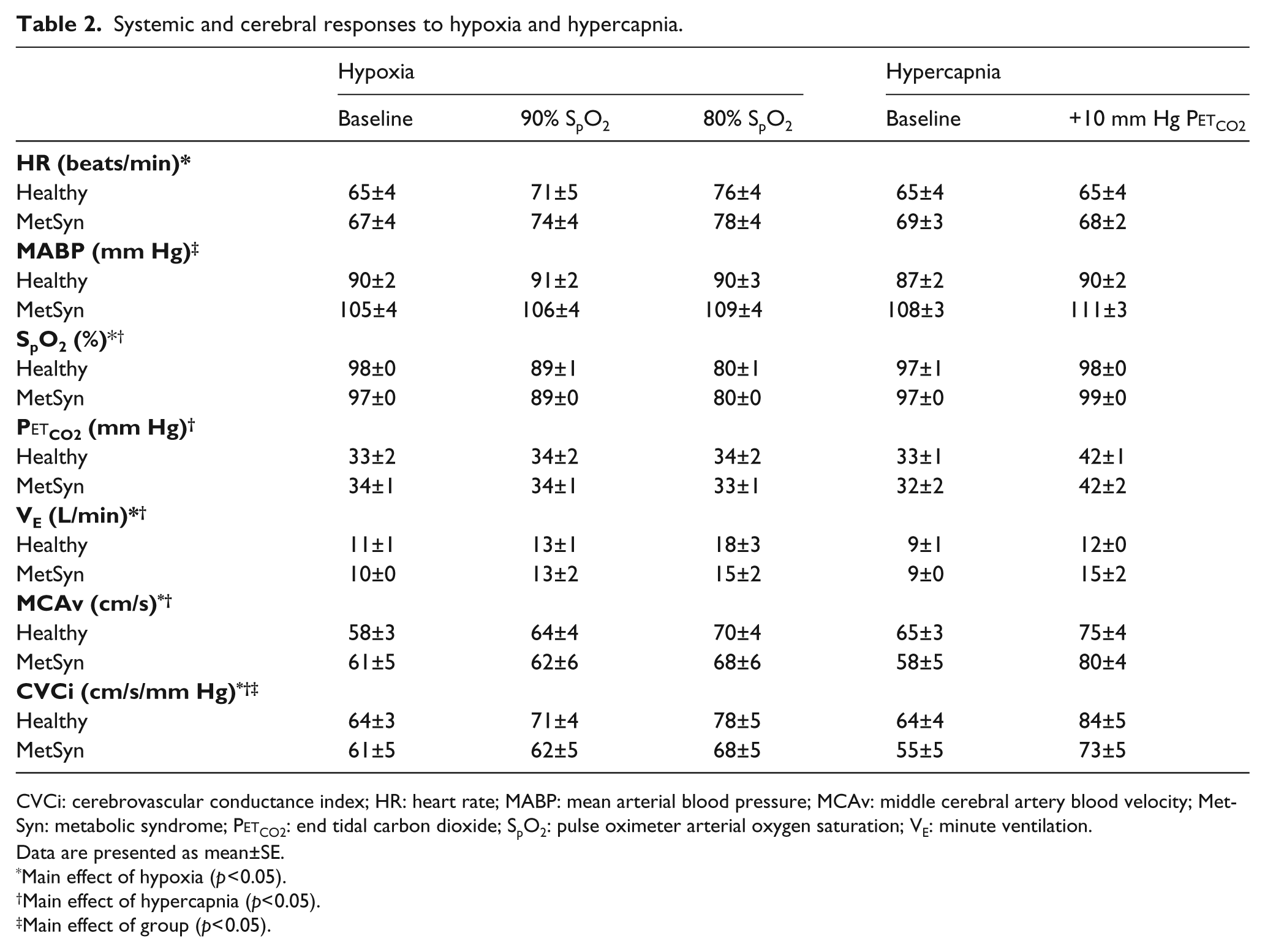
CVCi: cerebrovascular conductance index; HR: heart rate; MABP: mean arterial blood pressure; MCAv: middle cerebral artery blood velocity; MetSyn: metabolic syndrome; P
Data are presented as mean±SE.
Main effect of hypoxia (p<0.05).
Main effect of hypercapnia (p<0.05).
Main effect of group (p<0.05).
Cerebral responses to hypoxia
MCAv and CVCi values are presented in Table 2. MCAv values were similar between groups and condition but CVCi was lower in adults with MetSyn compared to healthy controls (main effect of group, p<0.05, Table 2). There was also a main effect of hypoxia on CVCi (p<0.05). Group mean CVCi–SpO2 relationships are illustrated in Figure 1(A). Absolute ΔCVCi (Figure 1(B)), relative ΔCVCi (%ΔCVCi, data not shown) and hypoxia reactivity (ΔCVCi/ΔSpO2%, Figure 1(C)) were all lower in adults with MetSyn (main effect of group, p<0.05 ). There was a main effect of hypoxia intensity on both ΔCVCi (Figure 1(B), p<0.05) and %ΔCVCi (data not shown). When data are expressed and analysed as ΔMCAv, %ΔMCAv, and ΔMCAv reactivity, conclusions remain the same as CVCi (data not shown). Analysing data as cerebrovascular resistance index (CVRi) absolute change, relative change, and reactivity also yields the same conclusions (data not shown).
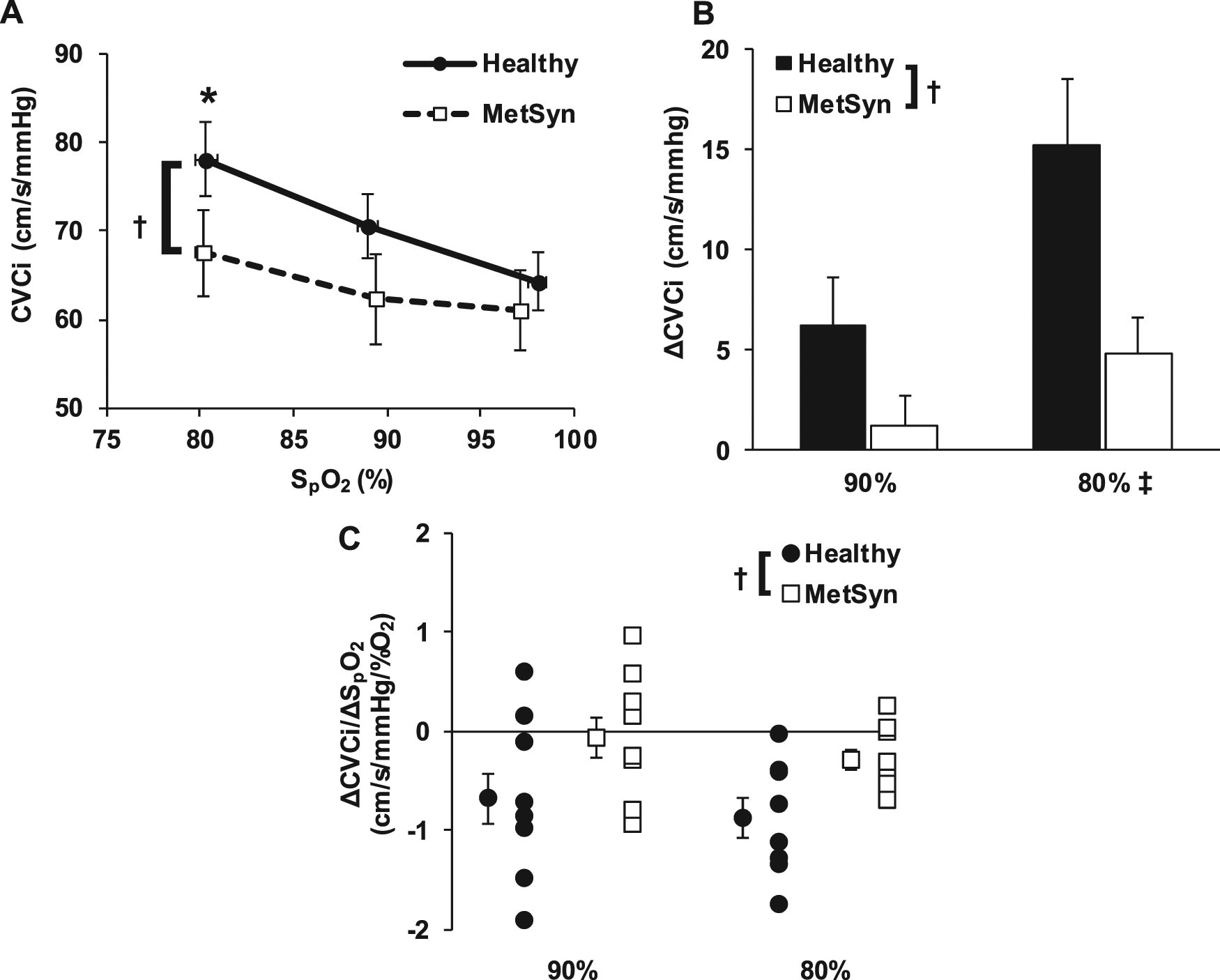
Isocapnic hypoxia. (A) Group mean CVCi – SpO2 values in metabolic syndrome (MetSyn) and healthy adults; (B) Group mean absolute ΔCVCi to 90% and 80% SpO2 ; (C) Individual subject and group mean stimulus-response slopes of CVCi at 90% and 80% SpO2 (a negative value reflects vasodilation).
Systemic responses to hypercapnia
Systemic haemodynamic values are summarised in Table 2. Heart rate did not differ between groups or between baseline and hypercapnia. MABP was greater in adults with MetSyn (p<0.05), but did not change in either group with hypercapnia. Hypercapnia increased P
Cerebral responses to hypercapnia
MCAv and CVCi values are presented in Table 2. MCAv values were similar between groups, but CVCi was lower in adults with MetSyn compared to healthy controls (main effect of group, p<0.05, Table 2). There was a main effect of hypercapnia on both MCAv and CVCi (p<0.05, Table 2). Group mean CVCi–P
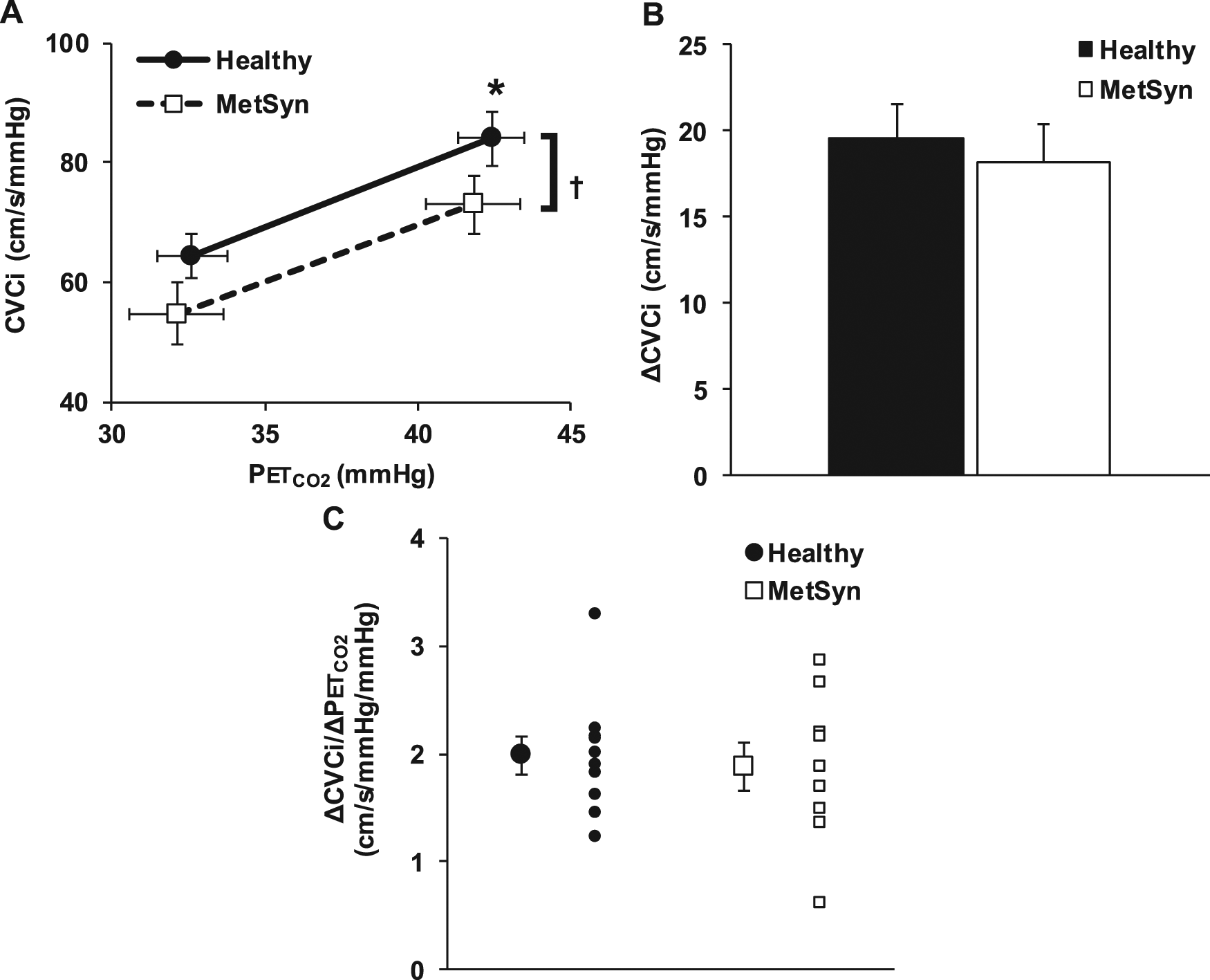
Hyperoxic hypercapnia. (A) Group mean CVCi and P
Discussion
We hypothesised that adults with MetSyn would exhibit reduced cerebrovascular dilation to both hypoxia and hypercapnia. We studied younger adults, removing the confounding influence of primary aging and emphasizing the cumulative impact of MetSyn criteria before onset of clinically overt cerebrovascular disease. Using this approach, our data demonstrate that adults with MetSyn exhibited: (1) impaired cerebrovascular responses to hypoxia and (2) preserved hypercapnia-induced cerebral vasodilation. These findings indicate that younger adults with MetSyn exhibit impaired cerebrovascular function prior to clinical presentation of metabolic or cardiovascular disease, and contribute novel physiologic insight into why adults with MetSyn are at greater risk of cerebrovascular disease and stroke.
Hypoxia
These data demonstrate that adults with MetSyn have blunted cerebral vasodilation to hypoxia whether data was expressed as absolute, relative, or stimulus-response ΔCVCi (Figure 1, main effect of group). Additionally conclusions remain the same if the data is expressed as MCAv or as CVRi. Hyperventilation-induced hypocapnia and concomitant vasoconstriction is a theoretical confounder of cerebrovascular responsiveness to hypoxia. We were careful to maintain P
We postulate that either the threshold for hypoxic dilation is shifted in adults with MetSyn or these adults are closer to maximal hypoxia-mediated vasodilation at baseline, limiting dilator capacity. If their hypoxic dilation threshold is shifted, adults with MetSyn may maximally vasodilate at more severe levels of desaturation (SpO2<80%). However, we did not test more severe levels of hypoxia for subject safety, and because 80% SpO2 encompasses many clinically relevant conditions (i.e. sleep disordered breathing). Dilator capacity would also be severely limited if these adults are close to their maximal hypoxic-mediated vasodilation at baseline. This may be a result of unfavourable inward vascular remodelling, which has been demonstrated in animal models of MetSyn. 8 Regardless of aetiology, adults with Metsyn may be predisposed to cerebral ischaemia when exposed to hypoxic stressors. In turn, this may promote decrements in cognition 14 or vascular function. 15
Hypercapnia
Contrary to our hypothesis, adults with MetSyn demonstrated preserved hypercapnia reactivity regardless of data expression. The relatively young age of our subjects with MetSyn (37±3 yrs) may indicate that they have not had MetSyn long enough for the multi-component disease to impart its full negative effects. Consistent with this concept, MetSyn has been established as an independent predictor of reduced cerebral vasomotor reactivity to CO2 in older patients with atherosclerosis. 9 However, if MetSyn progresses to type II diabetes, then the MetSyn criteria may no longer be as important for stroke risk as atherosclerotic vascular disease. 16 Taken together, these data indicate that as MetSyn progresses to cardiovascular and metabolic disease in humans, hypercapnic reactivity may be lost. Along these lines, the age of our subjects might suggest that younger adults with MetSyn utilise redundant vasodilator signals to achieve normal hypercapnic dilation but it takes years of MetSyn to lose compensatory pathways.
A second explanation is that we may have underestimated or masked any difference in responsiveness to hypercapnia between the groups. We co-administered hyperoxia to prevent arterial oxygen desaturation, which may limit the increase in blood velocity and blood pressure. 17 If hyperoxia prevented a greater increase of velocity in the healthy controls and a blood pressure increase in the adults with MetSyn, then hypercapnia performed under normoxia conditions may result in a significantly reduced ΔCVCi in the adults with MetSyn and alter our conclusions.
Potential vasodilator mechanisms
The mechanistic contributions to hypoxia- and hypercapnia-mediated vasodilation remain obscure as reviews have highlighted the influence of complementary or overlapping mechanisms. 18 Consistent with this concept, significant within-group response variability to hypoxia (Figure 1(C)) and hypercapnia (Figure 2(C)) indicates that, despite tight experimental control, there is not a uniform response to each stimulus within group. When taken in context with animal studies, there appear to be several testable hypotheses regarding potential pathogenic mechanisms of cerebrovascular impairment in MetSyn.
Hypoxia studies performed primarily in healthy humans and animals have provided mixed conclusions. Nitric oxide (NO) has been shown to be both obligatory19,20 and not required.21,22 Similarly, prostaglandins may22,23 or may not 24 be important. Even less is known about how MetSyn may affect hypoxic vasodilator mechanisms. Though isolated middle cerebral arteries from obese Zucker rats (OZR) have reduced hypoxic vasodilation, 25 studies demonstrate both a conservation 23 and an impairment 26 in endothelial NO formation depending on pharmacological stimulus and vessel studied. Reduced prostaglandin contribution 23 and potassium channel dysfunction26,27 in OZR have been more consistent findings.
Hypercapnia-mediated vasodilation in humans also remains inconclusive. Prostaglandins23,24,28,29 and vascular smooth muscle potassium channels26,27 each appear to contribute to vasodilation, while the contribution of NO has been shown to be both essential20,30 and non-obligatory.21,31 It is unclear how MetSyn may affect or alter signalling pathways in humans, but an important idea to test is that younger adults with MetSyn utilise redundant mechanisms to evoke preserved hypercapnic vasodilation.
Experimental considerations
Transcranial Doppler does not measure middle cerebral artery diameter and therefore cannot quantify cerebral blood flow. However, studies suggest that the diameter of the middle cerebral artery is not altered with physiological challenges32,33 meaning that changes in velocity reflect changes in cerebral blood flow with a reasonable degree of accuracy. 34
We propose that the cumulative effect of MetSyn criteria, rather than hypertension alone, is the key detriment negatively impacting cerebral vessel function. Hypertension is a key risk factor for stroke and may be a crucial influence on cerebrovascular dysfunction. 35 This is a matter of debate, however, as hypertension was not associated with decreased cerebral vasomotor reactivity to CO2. 9 To investigate the role of hypertension in impaired vascular regulation in our subjects, we correlated baseline blood pressure to hypoxia and hypercapnia reactivity values and found no relationship (data not shown). Therefore, the combined impact of the MetSyn criteria may prove more detrimental to cerebrovascular function than any individual criterion in subclinical disease.
The utilisation of finger pulse oximeter (SpO2) as our marker of hypoxia is not as strong as using arterial blood gas measurements. However, excellent agreement has been observed between SpO2 and arterial oxygen saturation spanning the range between 70–100%. 36 Also, we have no reason to believe the oxyhaemoglobin dissociation curve is altered in MetSyn adults. Therefore, we assume SpO2 is a valid of a measure of arterial oxygen saturation in both groups and we do not expect that it significantly impacts our results or interpretation.
We relied on self-report of sleep apnea. One subject with MetSyn reported having a continuous positive airway pressure (CPAP) machine, but had a normal desaturation event index without wearing it. This is important as the relationship between metabolic disorders and sleep-disordered breathing is multidirectional, 37 and sleep apnea has been shown to decrease cerebral vasomotor reactivity to hypoxia and hypercapnia. 13 However, when the individual was excluded from data analysis our conclusions were unchanged so the subject was included in all analyses.
Clinical perspectives
Cerebral vasomotor reactivity reflects the ability of distal cerebral arteries to respond to a homeostatic perturbation 38 and is important in stabilising ventilation during sleep-disordered breathing. 29 Reduced hypoxia reactivity has been shown in adults with sleep-disordered breathing. 13 Consistent with these ideas, MetSyn increases the risk of stroke three-fold in men with sleep-disordered breathing. 39 This study adds to the current body of literature by suggesting a portion of the increased risk of sleep-disordered breathing in adults with MetSyn is due to impaired vasodilation to a clinically relevant level of hypoxaemia. Adults with MetSyn may experience more severe nightly ischaemic episodes, which could lead to higher susceptibility to chronic decrements in cognitive 14 and vascular function. 15 In turn, this may promote respiratory instability and sleep disordered breathing.
There is evidence suggesting an association between MetSyn and cognitive dysfunction,40,41 although the impact on cerebral vascular responsiveness was not assessed. Taken together with our data, impaired cerebral vasodilation is one potential link between MetSyn and poor cognitive outcomes.
It is known that MetSyn increases the risk of stroke two-fold. 3 The current study provides additional insight into cerebrovascular disease onset at a point where stroke or cerebrovascular disease may not manifest for decades, as the average age of stroke is approximately 68 years of age. 42 Considering these stroke statistics, our novel findings open a 20–30 year treatment window for therapeutic interventions to prevent or reverse cerebrovascular disease in relatively younger adults with MetSyn.
Conclusion
These findings provide novel insight into the cerebrovascular function of adults with MetSyn who clearly demonstrate a failure to appropriately respond to reductions in cerebral oxygen delivery. The negative effects of MetSyn on cerebral vasculature appear specific to hypoxia in these relatively young adults. The results of this study provide researchers and clinicians with fundamental physiologic insight necessary to pursue interventions to improve cerebrovascular function in relatively young adults with MetSyn to reduce the risk and severity of cerebrovascular disease.
Footnotes
Acknowledgements
We are grateful for the participation of the subjects. We are also thankful to additional personnel at the University of Wisconsin for technical support: Jacqueline K Limberg, David F Pegelow, Edward J McKenna and Lee A Linstroth.
Funding
This work was supported by the American Heart Association (11PRE7390038, JWH); and NIH (HL105820, WGS).
Conflicts of interest statement
The authors declare that there is no conflict of interest.