
Abstract
Telmisartan partially activates the peroxisome proliferator-activated receptor γ (PPARγ), which may ameliorate the accumulation of visceral adipose tissues and sensitise insulin action. Nineteen patients with essential hypertension and metabolic syndrome were randomly assigned to receive 40 mg of telmisartan (TELMI group) once daily or 80 mg of valsartan (VAL group) once daily for 24 weeks. The visceral fat area (VFA) measured by computed tomography (CT) was significantly reduced from 150.4±15.5 to 127.7±16.7 cm2 in the TELMI group (p=0.049). Although VFA was also reduced in the VAL group from 169.8±14.8 to 155.3±14.8 cm2, the change was not significant (p=0.173). There were no significant changes in body weight, body mass index (BMI), waist circumference, subdermal fat area (SFA), fasting plasma glucose, and homeostasis model assessment of insulin resistance (HOMA-IR) in comparison to the baseline and follow-up data in both groups. In conclusion, telmisartan may have a benefit in the reduction of visceral adipose tissues in comparison to valsartan.
Introduction
Metabolic syndrome is a cluster of common cardiovascular risk factors including hypertension, atherogenic dyslipidaemia, insulin resistance and visceral fat obesity. 1 Metabolic and vascular abnormalities associated with metabolic syndrome are inevitably linked to the dysregulation of secretion of various adipokines from accumulated visceral adipose tissues. Metabolic syndrome is present in about 10–25% of individuals in industrialised countries.2,3 The increasing availability of high-calorie, low-fibre foods and the adoption of sedentary lifestyles are leading to an increased prevalence of the metabolic syndrome in developing countries as well as in industrialised countries. 4
Telmisartan is an angiotensin II type1 receptor blocker (ARB) originally developed for the treatment of essential hypertension. It was also reported to partially activate the peroxisome proliferator-activated receptor γ (PPARγ), which may improve insulin sensitivity and dysregulation of adipokine secretion.5–7 Telmisartan improved insulin sensitivity in diet-induced obese mice without weight gain. 8 This evidence may suggest that activation of PPARγ by telmisartan has additional benefits in the treatment of individuals with metabolic syndrome and hypertension.
In the current randomised controlled study, patients with essential hypertension and metabolic syndrome were treated with either telmisartan or valsartan for 24 weeks. The clinical outcomes were evaluated after treatment by assessing visceral fat area (VFA) and subdermal fat area (SFA) measured by abdominal computed tomography (CT).
Methods
Patients and study design
This was a prospective, randomised, controlled open-label clinical trial at Okayama University Hospital. Patients that fulfilled the criteria of hypertension and metabolic syndrome were eligible and included in the study. Essential hypertension was defined by office systolic blood pressure ≥140 mm Hg and/or diastolic blood pressure ≥90 mm Hg, and metabolic syndrome was defined according to the Japan Society for the Study of Obesity (JASSO) criteria as a waist circumference (≥85 cm in men and ≥90 cm in women), plus any two of the following three factors: (1) hypertriglyceridaemia (≥150 mg/dl) or low high-density lipoprotein (HDL) cholesterol (<40 mg/dl); (2) elevated blood pressure: systolic blood pressure of 130 mm Hg or greater or diastolic blood pressure of 85 mm Hg or greater, or both; (3) high fasting glucose: serum glucose concentration of 110 mg/dl or greater.
Study protocol
Nineteen patients with essential hypertension (9 men and 10 women) at Okayama University Hospital were enrolled from 2008 to 2010. They were randomly assigned by the Internet Data and Information Center for Medical Research (INDICE) central entry system of the University Hospital Medical Information Network (UMIN) to receive either 40 mg of telmisartan (TELMI group) once daily or 80 mg of valsartan (VAL group) once daily for 24 weeks. Additional antihypertensive agents other than angiotensin-converting enzyme (ACE) inhibitors and other ARBs were initiated if the target blood pressure of <130/80 mm Hg was not achieved. Furthermore, thiazolidinediones and insulin were not used throughout the study.
Clinical efficacy and outcomes
The primary outcomes were body weight, body mass index (BMI), waist circumference, and the area of VFA and SFA, which were assessed at the level of the umbilicus with CT. Secondary outcomes were blood pressure both in the office and at home, the albumin/creatinine ratio (ACR), fasting plasma glucose and serum cholesterol level. The homeostasis model assessment of insulin resistance (HOMA-IR) = (fasting insulin (µU/ml) × fasting glucose (mg/dl)/405]) was also calculated as an indicator of insulin resistance.
Statistics
All data are presented as the mean ± standard error of the mean (SEM) unless otherwise noted. Differences between paired variables were analysed by the Wilcoxon test. Statistical analysis was carried out using PASW Statistics 18 (SPSS Inc., Chicago, IL, USA). A p value less than 0.05 was considered to be statistically significant.
Results
Nine of the 19 patients were assigned to the TELMI group and 10 to the VAL group, and all patients were available for analysis. Baseline clinical characteristics did not differ between the two groups: the TELMI group included three males and six females with a mean age of 61.4 ± 4.58 years, and the VAL group included six males and four females with a mean age of 50.4 ± 4.75 years. Both telmisartan and valsartan were well-tolerated without any major adverse events. The systolic blood pressure at home significantly decreased in both groups after 24 weeks of treatment, and there were no differences between the two groups (Table 1). The VFA determined by abdominal CT was significantly reduced from 150.4 ± 15.5 to 127.7 ± 16.7 cm2 in the TELMI group (p = 0.049). Although the VFA also decreased in the VAL group from 169.8 ± 14.8 to 155.3 ± 14.8 cm2, the change was not significant (p = 0.173). ACR was significantly reduced in the VAL group from 73.4 ± 24.8 to 30.6 ± 14.3 mg/gCr (p = 0.005) but not in the TELMI group (25.4 ± 4.1 to 18.5 ± 5.3 mg/gCr). There were no significant changes in the body weight, BMI, waist circumference, SFA, fasting plasma glucose, HOMA-IR and serum cholesterol in comparison to the baseline and follow-up data (Table 1).
Baseline metabolic parameters and their changes after 24 weeks of treatment with telmisartan and valsartan.
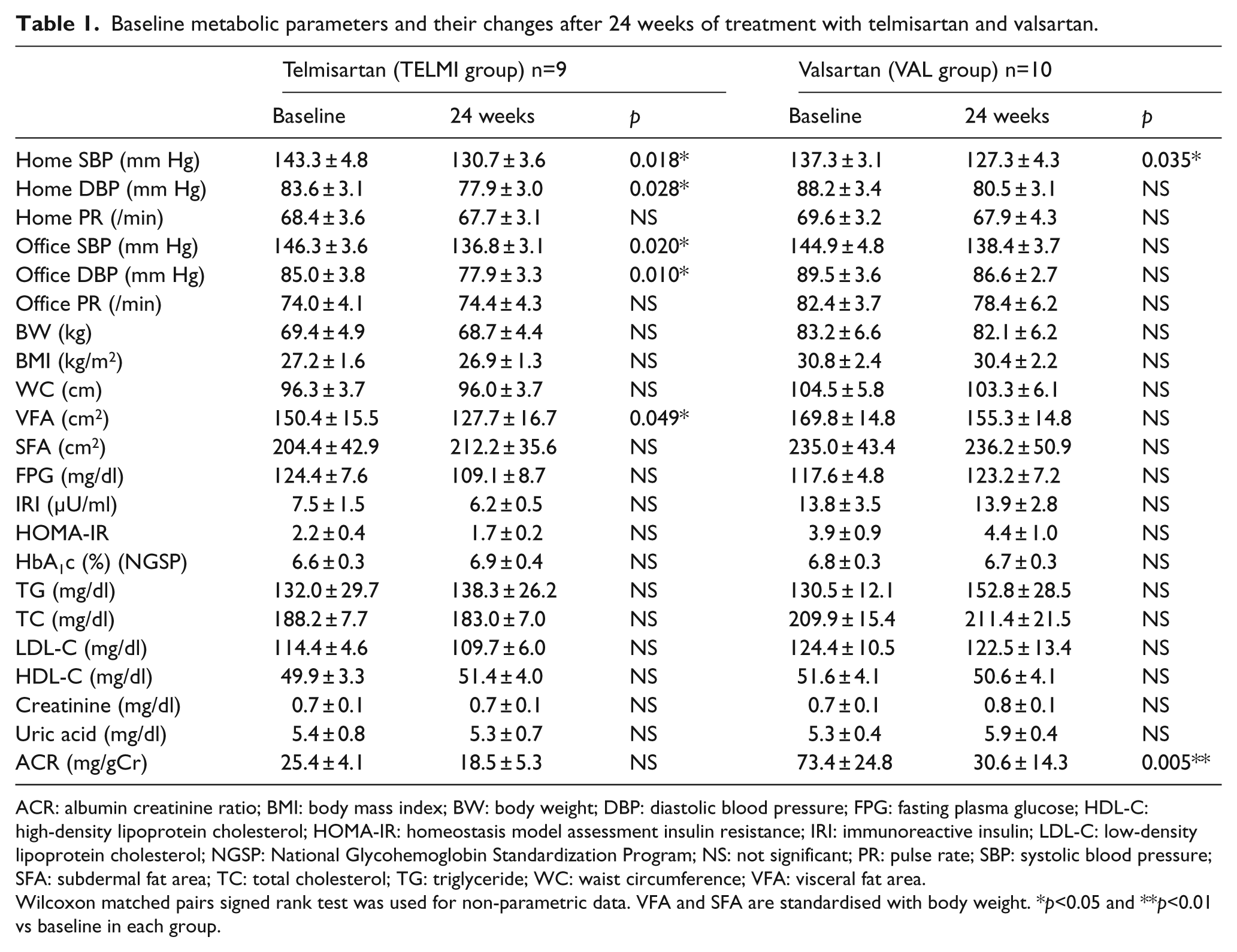
ACR: albumin creatinine ratio; BMI: body mass index; BW: body weight; DBP: diastolic blood pressure; FPG: fasting plasma glucose; HDL-C: high-density lipoprotein cholesterol; HOMA-IR: homeostasis model assessment insulin resistance; IRI: immunoreactive insulin; LDL-C: low-density lipoprotein cholesterol; NGSP: National Glycohemoglobin Standardization Program; NS: not significant; PR: pulse rate; SBP: systolic blood pressure; SFA: subdermal fat area; TC: total cholesterol; TG: triglyceride; WC: waist circumference; VFA: visceral fat area.
Wilcoxon matched pairs signed rank test was used for non-parametric data. VFA and SFA are standardised with body weight. *p<0.05 and **p<0.01 vs baseline in each group.
Discussion
Telmisartan is a partial PPARγ agonist. Many animal studies have demonstrated the beneficial effects on obesity, accumulation of visceral adipose tissues, insulin sensitivity and fatty liver. Telmisartan prevents obesity by increasing the expression of uncoupling protein-1 (UCP-1) in diet-induced obese (DIO) mice 9 and Sugimoto et al. reported telmisartan may increase energy expenditure by increasing fatty acid oxidation in skeletal muscle. 10 By focusing on inflammation in adipose tissues, telmisartan improves insulin resistance by inhibiting T-cell infiltration 11 and modulating adipose tissue macrophage polarisation to the anti-inflammatory M2 state in DIO mice. 12 Telmisartan attenuates the progression of steatohepatitis by suppressing macrophage infiltration in the liver, skeletal muscle and adipose tissue. 13 By comparison with valsartan in animal experiments, telmisartan increases energy expenditure, efficiently reduces adipocyte size and protects against obesity and steatohepatitis.14,15
Clinical trials also demonstrated beneficial effects of telmisartan beyond blood pressure control; telmisartan decreases the accumulation of visceral adipose tissue, and improves insulin sensitivity.16,17 Comparing telmisartan and losartan, telmisartan significantly reduces VFA and HOMA-IR, and increases serum adiponectin levels. 18
The current study found that the administration of telmisartan led to a reduction of visceral adipose tissue mass, suggesting a beneficial impact of telmisartan on the accumulation or remodeling of visceral adipose tissues. However, the study failed to demonstrate improvements in fasting plasma glucose, HOMA-IR and lipid profiles in either the TELMI and VAL groups. Another study also reported no differences in cardiovascular, metabolic, and inflammatory parameters in patients with uncomplicated hypertension treated with telmisartan and valsartan for 12 weeks. 19 The metabolic benefits beyond blood pressure as a partial PPARγ agonist may not be apparent because the population size of the current randomised and controlled study was small. Furthermore, a longer duration of study or the use of higher drug doses might be associated with greater differences between the telmisartan and valsartan treatment groups. Future clinical studies comparing ARBs with PPARγ agonist activities, such as azilsartan, 20 are equired to demonstrate the benefits of this new class of ARBs.
There are limitations to the current study. First, this study was an open label trial, thus it is possible that the results may have been influenced by the unconscious bias of the investigators, who were unblinded and aware of who received which intervention. Second, the TELMI and VAL groups did not appear to be well-matched for some study variables at baseline including body weight, BMI and ACR, although the differences were not statistically significant. However, the randomisation protocol did not completely balance the two treatment groups for all variables at baseline and this could have affected the outcome of the study. Third, the statistical analysis was not adjusted for multiple comparisons and the differential effects of telmisartan and valsartan on the study variables had only borderline statistical significance.
In conclusion, the results of the current study imply that telmisartan may have a clinical benefit in the reduction of visceral adipose tissues in comparison to valsartan. Further study is recommended to confirm the beneficial effect of telmisartan on VFA reduction in individuals with metabolic syndrome and hypertension.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
The authors declare no conflicts of interest relevant to this article.