
Abstract
Metabolic syndrome (MetS) is an inflammatory state associated with high coronary disease risk. Inflammation and adaptive immunity modulate atherosclerosis and plaque instability. We examined early changes in anti-oxidized low-density lipoprotein (LDL) (anti-oxLDL) autoantibodies (Abs) in patients with MetS after an acute coronary syndrome (ACS). Patients of both genders (n=116) with MetS were prospectively included after an acute myocardial infarction (MI) or hospitalization due to unstable angina. Anti-oxLDL Abs (IgG class) were assayed at baseline, three and six weeks after ACS. The severity of coronary disease was evaluated by the Gensini score. We observed a decrease in anti-oxLDL Abs titers (p<0.002 vs. baseline), mainly in males (p=0.01), in those under 65 y (p=0.03), and in subjects with Gensini score above median (p=0.04). In conclusion, early decrease in circulating anti-oxLDL Abs is associated with coronary disease severity among subjects with MetS.
Keywords
Introduction
The initial steps of atherosclerosis involve endothelial dysfunction and subsequent deposition of oxidized low-density lipoprotein (oxLDL) in the arterial wall, thus triggering a cascade of events that include chemotaxis, adhesion, phagocytosis and the release of cytokines.1–3 Classical risk factors for atherosclerotic disease exert their atherogenic actions in part by promoting, facilitating, or permitting the oxidation of low-density lipoprotein (LDL). 4 The residues from oxidized particles are highly immunogenic, and stimulate B- lymphocyte cells to produce a broad spectrum of autoantibodies (Abs) to different epitopes of the modified LDL.5,6 Further evidences of immune complexes formation in the circulation and in the vascular wall by oxLDL and respective Abs have been detected in several animal models and in humans with atherosclerosis.7,8 The precise role of anti-oxLDL Abs is still under debate, with a broad spectrum of actions being described, from a protective role on atherosclerosis to harmful effects on disease progression or plaque destabilization.9–12
Patients with unstable angina were reported to have lower titers of anti-oxLDL Abs than those with stable coronary artery disease, and these titers were inversely related to markers of inflammation.13,14 In addition, increased titers of anti-oxLDL Abs and on several markers of inflammation are common features of metabolic syndrome (MetS).15,16
Thus, we decided to evaluate the early changes in the anti-oxLDL Abs titers among subjects with MetS after an acute coronary syndrome (ACS) and their relationship with the severity of coronary disease.
Material and methods
Patients and study design
Subjects aged 30 to 75 years, of both sexes (n = 116) and hospitalized due to an ACS (acute myocardial infarction (MI) or unstable angina pectoris)17,18 were consecutively included in the study if they had MetS according to the National Cholesterol Education Program / Adult Treatment Panel III.19,20 Exclusion criteria were heart failure class III or IV, 21 moderate or severe renal or hepatic disease and other active inflammatory or infectious disease. Patients with any form of revascularization (surgical or percutaneous intervention), planned after hospital discharge, were also excluded. The project was approved by the ethics committee of the university and all participants provided written informed consent prior to study initiation.
This is an extension of a previous study 13 with participants prospectively evaluated at hospital discharge (baseline), three and six weeks thereafter. Titers of anti-oxLDL Abs, as well as the analysis of coronary angiograms, were made in a blinded fashion. Patients received optimal care to attain the usual therapeutic goals. For all patients, a dietician provided specific counseling based on the Therapeutic Lifestyle Changes recommended by the National Cholesterol Education Program / Adult Treatment Panel III. 19
Twelve-hour fasting samples were obtained at baseline, three and six weeks after hospitalization. Serum total cholesterol, high-density lipoprotein cholesterol (HDL-C) and triglycerides were determined enzymatically (Opera Bayer, Germany) with LDL-cholesterol (LDL-C) estimated by the Friedewald equation. 22 Glucose was assessed by enzymatic method and glycated hemoglobin (HbA1c) was measured using high-perfomance liquid chromatography. Concentrations of apolipoproteins (Apo) were determined by nephelometry (Array 360 Beckmann, Germany).
High-sensitivity C-reactive protein (hsCRP) was measured by nephelometry (R100 Analyser, Behringer, Germany), and plasma peroxidation was evaluated by the thiobarbituric acid-reactive substances (TBARS) assay. 23
We determined the antibodies to copper-oxidized LDL, using our own established enzyme-linked immunosorbent assay (ELISA) method as previously described.24,25 To increase the precision in quantifying anti-oxLDL Abs, IgG (10 mg/ml; purified human IgG, Pierce Protein Research Products, Thermo Scientific, Rockford, IL, USA) and a buffer blank (phosphate-buffered saline) were used as controls to compensate intra-plate variation. Inter-plate imprecision was minimized by processing all the samples in the same time period. To minimize false-positive results due to cross-reactivity with antigen naïve epitopes, antibody titers were expressed as the reactivity index (RI), calculated as RI=(ODsample – ODsample blank) / (ODIgG – ODIgG blank), where IgG was used as a control. Samples were run in triplicate and the variation within the triplicates did not exceed 5% of the mean.
Coronary angiography was performed in all patients before hospital discharge. The extension and severity of coronary atherosclerosis was examined by an invasive cardiologist using the Gensini score, which depends on the degree of luminal narrowing and the importance of the site of coronary stenosis, as previously described. 26
Statistical analyses
Categorical variables are presented as number (%) and compared by Pearson’s χ2 test. Numerical data are reported as means and standard deviation (SD) or median values and interquartile range (IQR). Continuous variables at baseline were compared using either the Student’s t-test for parametric data or the Mann-Whitney test in case of non-Gaussian distribution. Analyses of variance (ANOVA) with repeated measures, or Wilcoxon and Mann-Whitney tests were used for comparisons of short-term effects within and between genders. Spearman’s correlation coefficients were tested. A p-value of less than 0.05 was considered significant. All analyses were performed using the Statistical Package for the Social Sciences (SPSS) software (17.0) for Windows.
Results
The mean (SD) hospital stay due to the ACS was 6.6 ± 3.3 days. Demographic, clinical parameters and pharmacologic therapy at baseline are presented in Table 1.
Characteristics of study population at baseline.
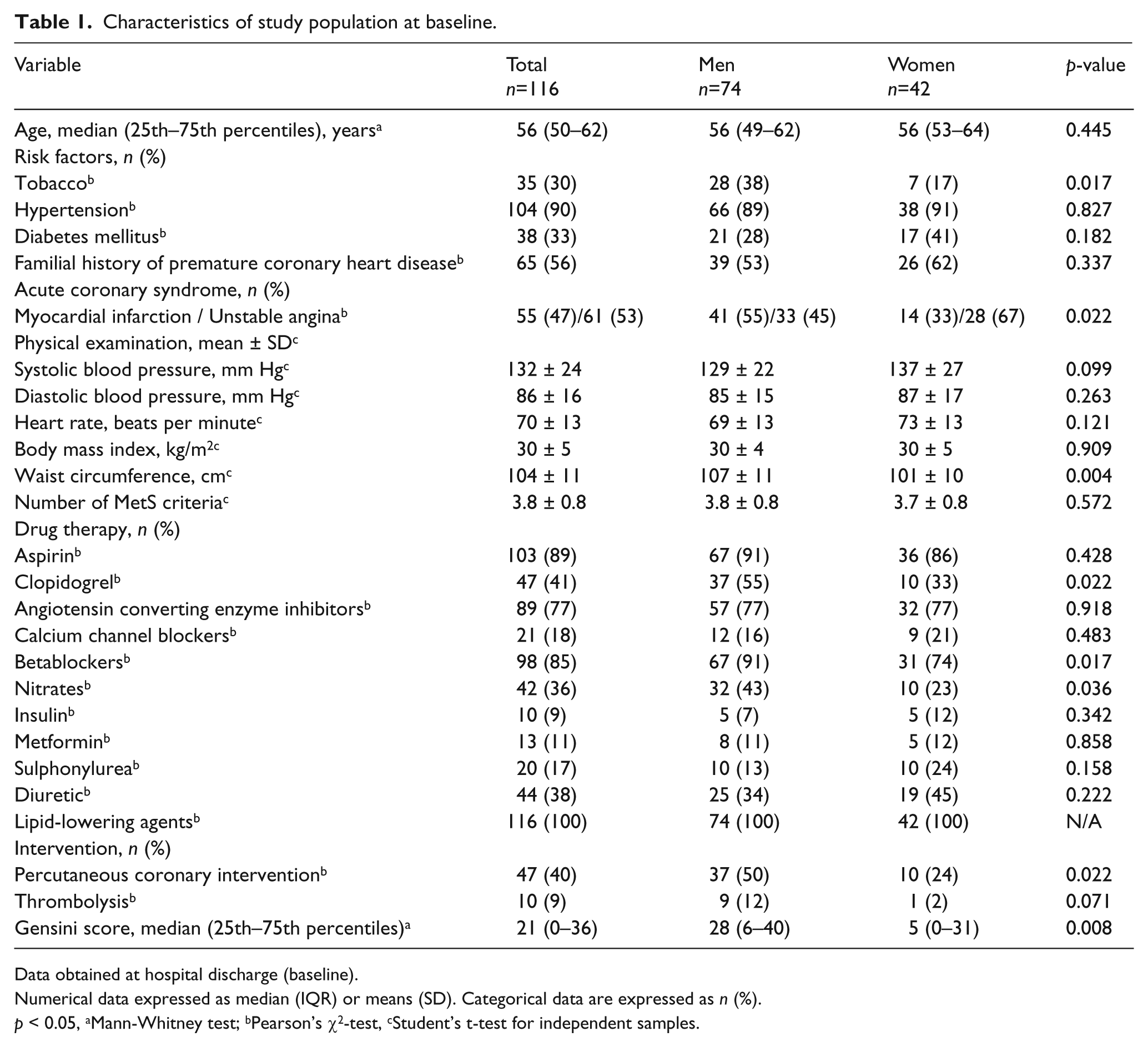
Data obtained at hospital discharge (baseline).
Numerical data expressed as median (IQR) or means (SD). Categorical data are expressed as n (%).
p < 0.05, aMann-Whitney test; bPearson’s χ2-test, cStudent’s t-test for independent samples.
Drug therapy was unchanged throughout the study, and all patients were under effective lipid-lowering therapy. Males corresponded to 64% of the sample, and MI was more common among them (55% vs. 33%; p = 0.022). We did not observe differences in age between men and women and the prevalence of risk factors, except that prevalence of smoking habit in males was higher than in females (p = 0.017). Body mass index was similar in both genders (30 ± 4 vs. 30 ± 5 kg/m2, p = 0.909) and, as expected, male subjects presented a higher waist circumference (107 ± 11 vs. 101 ± 10 cm; p = 0.004) than females. The number of components of MetS did not differ between genders at baseline.
Percutaneous interventions were performed in 47 (50%) of the patients, whereas 10 (9%) individuals received thrombolysis. In addition, a higher proportion of men were on clopidogrel, betablockers or nitrates, when compared with women.
The extension of coronary disease measured by the Gensini score showed median values (25th–75th percentiles) of 21 (0–36), with higher values in males than in female counterparts (28 (6–40) vs. 5 (0–31), p = 0.008). The percentage of men presenting Gensini score above the median was 59.5% vs. 31% in women (p = 0.013).
Systolic blood pressure levels slightly increased six weeks after the ACS compared with baseline (p = 0.028), without gender differences. Diastolic blood pressure did not change over the study.
Baseline laboratory variables were comparable between genders, except for HDL-C and Apo A, which were higher in women, and triglycerides, which were higher in men (Table 2).
Laboratory parameters of the study population at baseline and six weeks after an acute coronary syndrome.
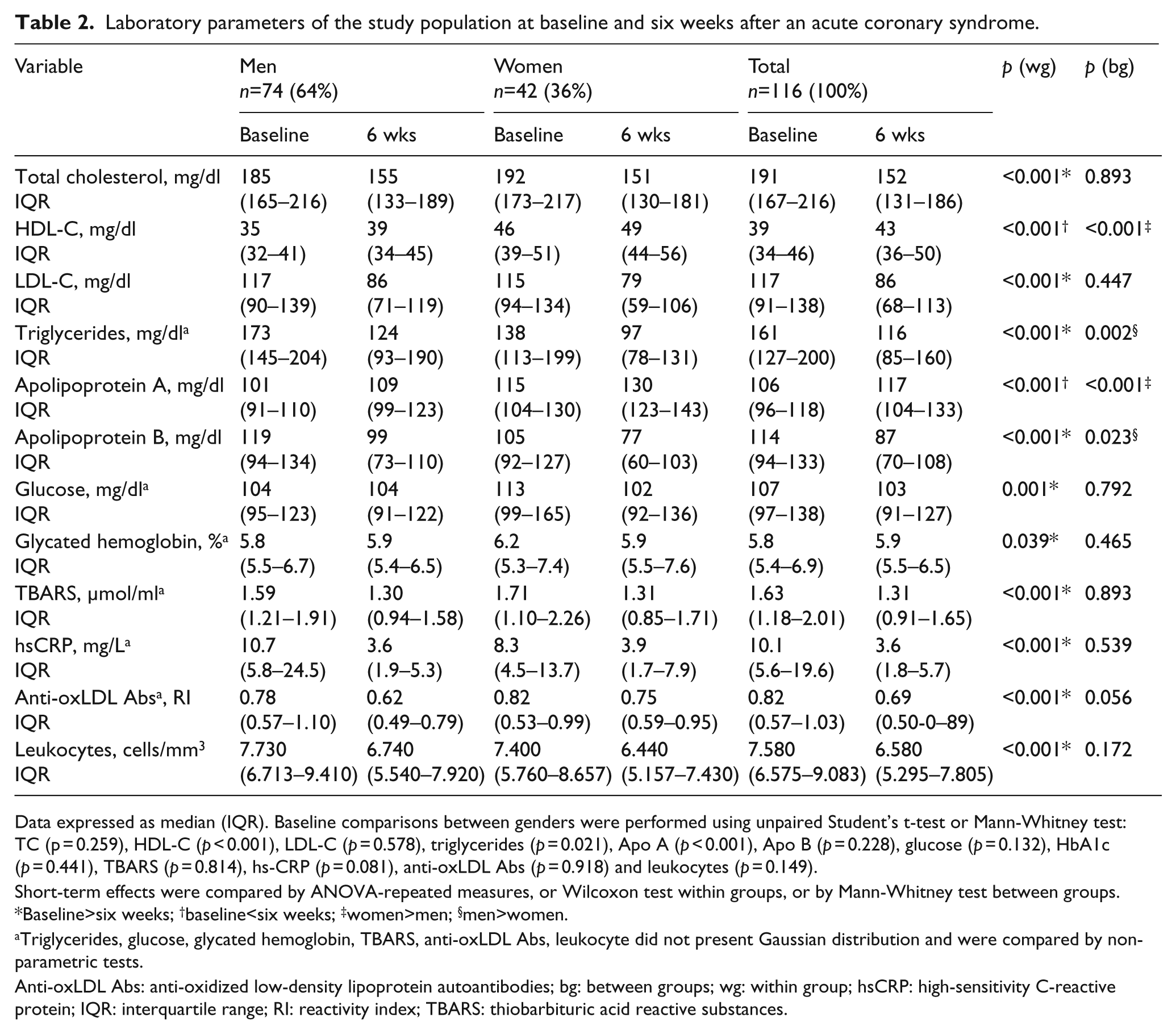
Data expressed as median (IQR). Baseline comparisons between genders were performed using unpaired Student’s t-test or Mann-Whitney test: TC (p = 0.259), HDL-C (p < 0.001), LDL-C (p = 0.578), triglycerides (p = 0.021), Apo A (p < 0.001), Apo B (p = 0.228), glucose (p = 0.132), HbA1c (p = 0.441), TBARS (p = 0.814), hs-CRP (p = 0.081), anti-oxLDL Abs (p = 0.918) and leukocytes (p = 0.149).
Short-term effects were compared by ANOVA-repeated measures, or Wilcoxon test within groups, or by Mann-Whitney test between groups. *Baseline>six weeks; †baseline<six weeks; ‡women>men; §men>women.
Triglycerides, glucose, glycated hemoglobin, TBARS, anti-oxLDL Abs, leukocyte did not present Gaussian distribution and were compared by non-parametric tests.
Anti-oxLDL Abs: anti-oxidized low-density lipoprotein autoantibodies; bg: between groups; wg: within group; hsCRP: high-sensitivity C-reactive protein; IQR: interquartile range; RI: reactivity index; TBARS: thiobarbituric acid reactive substances.
Total cholesterol, LDL-C, Apo B, glucose, glycated hemoglobin, TBARS, hs-CRP and leukocytes decreased six weeks after the ACS (p < 0.04) compared with baseline, without gender differences; triglyceride levels were also reduced at short-term follow-up, and men presented higher levels than women. HDL-C and Apo A levels increased six weeks after the ACS (p < 0.001) and were higher in women than in men (p < 0.001). The titers of anti-oxLDL Abs decreased three weeks after the ACS, and further at week six (0.87 ± 0.04 vs. 0.76 ± 0.03 vs. 0.73 ± 0.03; p = 0.002) compared to baseline in these subjects with MetS (Figure 1).
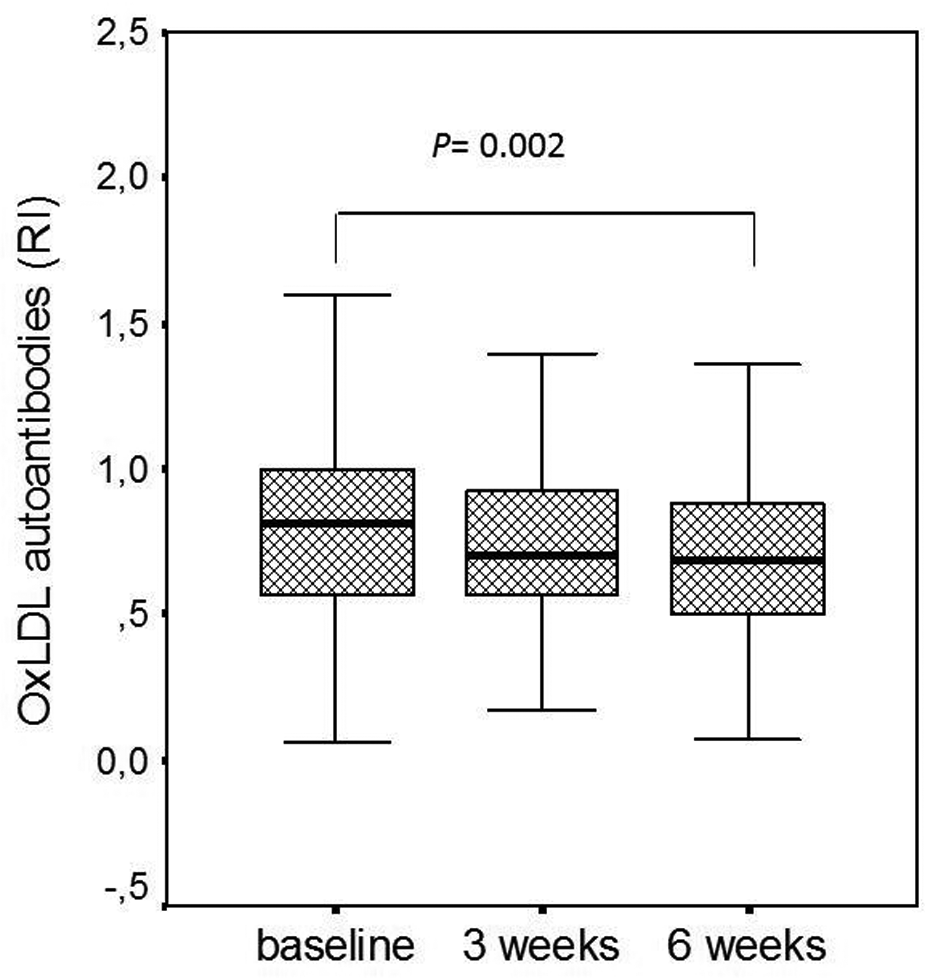
Box-plots showing medians, interquartiles and 95% confidence interval for oxLDL autoantibodies (RI) at baseline, three and six weeks after an ACS in patients with MetS. Anti-OxLDL Abs at week six were lower than baseline titers (p=0.022).
We did not observe differences in the titers of oxLDL autoantibodies across the number of components of MetS; we also tested for correlations between the Δ% of oxLDL autoantibodies and variables of lipid and glucose metabolism, as well as anatomic markers of atherosclerosis. No correlations were observed with any of these parameters (data not shown).
When categorized by gender, age (above or below 65 y) and severity of coronary heart disease (Gensini score above or below median), anti-oxLDL Abs progressively declined in males (p = 0.012), in subjects under 65 years (p = 0.032) and in those with Gensini score above median (p = 0.04) (Figure 2A–C).
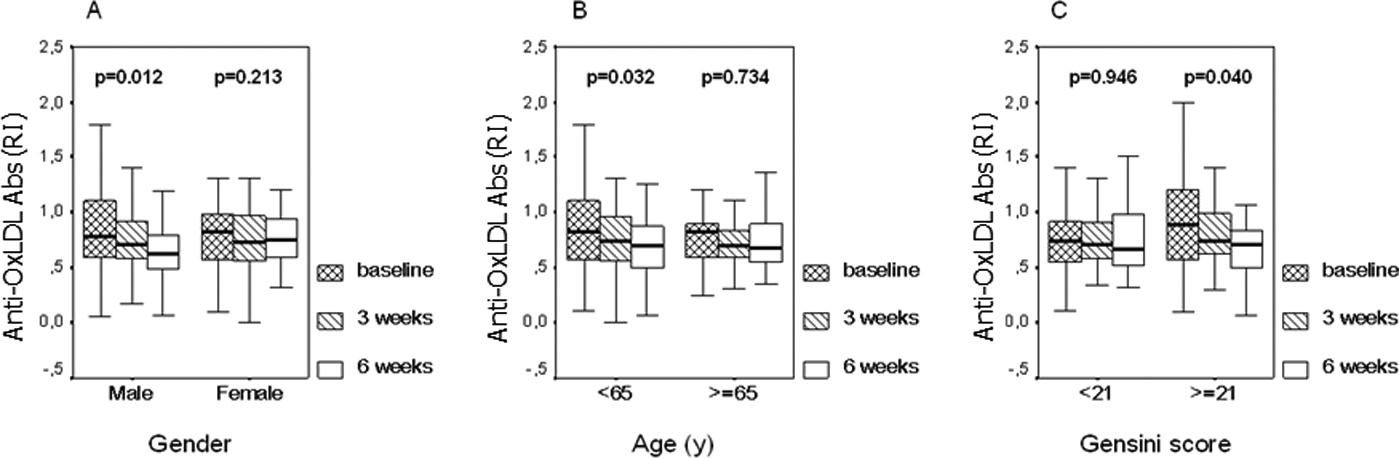
Box-plots showing medians, interquartiles and 95% confidence interval for oxLDL autoantibodies (RI) at baseline, three and six weeks after an ACS in patients with MetS, according to gender (a), age (< 65 or ≥ 65 y) (b) and severity of coronary atherosclerosis (Gensini score < 21 or ≥ 21) (c).
In addition, stratified by gender and clinical condition, we found that the decline in anti-oxlDL Abs occurred in males with MI (p = 0.012), with Gensini score above the median (p = 0.020), and in those below age 65 (p = 0.004), whereas decline in anti-oxLDL Abs was seen only in females with unstable angina (p = 0.040). Percutaneous intervention with bare metal stent implantation did not affect anti-oxLDL Abs levels (Table 3).
Distribution of anti-oxLDL Abs by clinical condition.
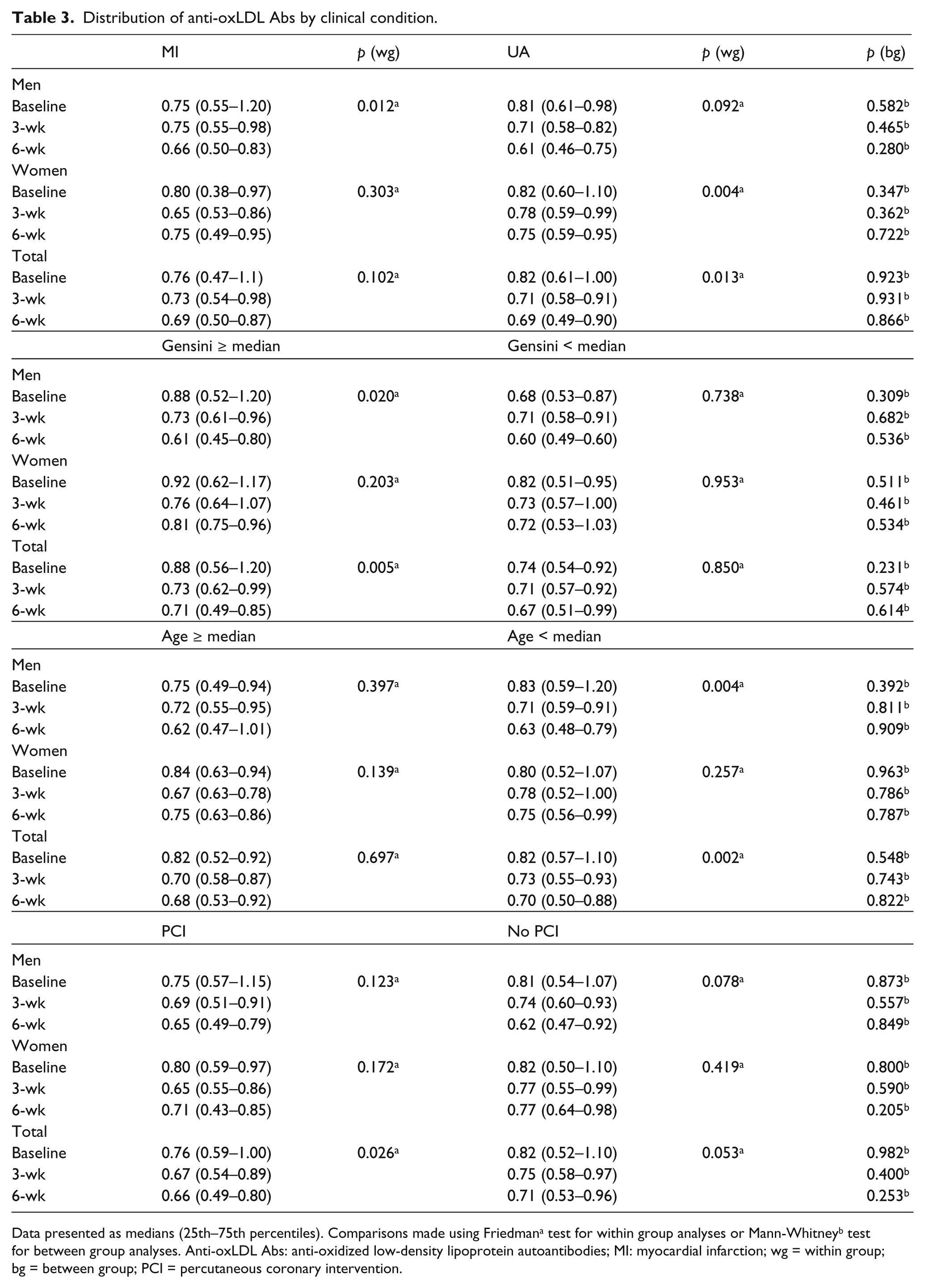
Data presented as medians (25th–75th percentiles). Comparisons made using Friedmana test for within group analyses or Mann-Whitneyb test for between group analyses. Anti-oxLDL Abs: anti-oxidized low-density lipoprotein autoantibodies; MI: myocardial infarction; wg = within group; bg = between group; PCI = percutaneous coronary intervention.
Discussion
Our study showed a continuous decrease in the anti-oxLDL Abs titers after an ACS among subjects with MetS, during the first six weeks of follow-up, in spite of a stable condition and global improvement of risk factors. Interestingly, this decline in the titers of anti-oxLDL Abs was observed in males, in middle-aged patients and in those individuals with more severe coronary artery disease. The decline in circulating anti-oxLDL Abs could be explained by consumption due to formation of immune complexes (IC) in an attempt to clear oxidized substrates (i.e. oxLDL) generated in this inflammatory environment. In agreement with this concept, a previous study involving smokers, subjects with increased oxidative milieu, found decreased oxLDL autoantibodies levels. 28
Anti-oxLDL Abs can be detected in healthy individuals, 28 but also in many other inflammatory conditions, such as periodontitis, 29 systemic lupus erythematosus, 12 as well as in chronic non-communicable diseases, like hypertension, 30 diabetes, 31 heart failure, 32 and in end-stage renal disease. 33 We have previously demonstrated that in healthy middle-aged subjects, these titers were higher than in ACS. 13
In the setting of coronary artery disease the presence of antibodies to different epitopes of oxidized lipids or peptides has been associated with acute coronary events. 34 Interestingly, in a murine model, human-derived IgG Fab antibody anti MDA-LDL blocked the uptake of oxLDL by macrophages in vivo, thus suggesting an important role in atherogenesis. 35 Antibodies of the IgG class recognize oxidized-specific epitopes; these antibodies are capable of binding and clearing proinflammatory oxidized lipids, and therefore may be atheroprotective. On the other hand, immunocomplexes (IC) of oxLDL with β2-glycoprotein I (β2GPI) and/or CRP were reported to localize in the intima of atherosclerotic lesions and were considered pro-atherogenic. 36 Our group has previously demonstrated that in patients with unstable angina, titers of oxLDL autoantibodies were lower than in stable patients. 25 It is therefore most likely that two classes of antibodies possibly exist: one protective and another that aggravates the risk of coronary disease, as previously suggested by Fernvik and colleagues. 24
The assumption that there is a consumption of antibodies by the formation of IC is based on the dynamic by which antibodies are produced by B-cells. The levels of antibodies are rapidly upregulated either via antigen-specific stimulation of memory cells or by recruitment of virgin B-cells as in the case of a primary response. The normal decay of IgG antibodies seems much slower; one reason could be linked to the maintenance of an immune state. Therefore, the explanation for our findings appears to be “consumption” of antibodies by the formation of IgG-oxLDL complexes. This is further emphasized by the short time in which the study was done and the inverse correlation found between circulating anti-oxLDL Abs and circulating or tissue-fixed oxLDL.
Our results support the hypothesis that acute inflammation decreases levels of anti-oxLDL Abs, and that if there is a sustained inflammation in the short-term follow-up of an ACS associated with MetS, these titers continue to decline, possibly due to increased generation of oxidized LDL components or oxidative products formed from the LDL particle that binds to free antibodies.
Balada et al. have postulated that the cause of the decreased levels of circulating anti-oxLDL Abs in the presence of oxidative stress may be explained by the clearance of these immunocomplexes. 37 Thus, anti-oxLDL Abs seem to have a dual effect, sometimes related to cardiovascular and autoimmune diseases, or have a protective role in atherosclerosis.10–14,38
However, conflicting results exist39–41 that may be explained by the different nature of the studied antibodies, different assays, differences in clinical scenario or even by the time when blood samples were obtained.
The observed differences between gender regarding autoantibodies levels is a matter of debate. In our study, women presented higher HDL-C and Apo A levels and less atherosclerosis than men. These characteristics may have accounted for the antioxidant effects and the inverse association between atherosclerosis and the level of these antibodies, as reported by Tinahones et al. 42 in a large population study.
Our study has some strengths and limitations. Anti-oxLDL Abs were assessed only in the short-term follow-up of an ACS. It is possible that stable clinical conditions following risk factors control and pharmacological therapy affect anti-oxLDL Abs generation and/or consumption over time. The behavior of the adaptive immunity at longer periods seems crucial for a better understanding of the role of B-cells on the modulation of atherosclerosis, its contribution for coronary risk stratification, as well as the opportunity for future therapeutic approaches. We did not perform intravascular ultrasound (IVUS) that could have been valuable for the evaluation of non-obstructive atheroma.
We did not assess anti-oxLDL Abs of IgM class and did not compare acute coronary syndrome in patients with and without MetS in this study. However, recent unpublished data of our group showed that mean (SD) values for Abs titers in patients with acute MI were 1.25 ± 0.17, higher than those observed in our patients with ACS (unstable angina/MI plus MetS).
Our study showed that anti-oxLDL Abs titers decline in the short-term follow-up after an ACS in subjects with MetS. These findings occurred mainly in males with higher extension of coronary artery disease and with the acute coronary event occurring earlier in their lives. In conclusion, early decrease in circulating anti-oxLDL Abs is associated with coronary disease severity among subjects with MetS.
Footnotes
Funding
This work was supported by research grant number 2004/00325-8 from FAPESP (The State of São Paulo Research Foundation), São Paulo, SP, Brazil; The Complex Fluids Institute of the National Council of Research Foundation (CNPq-INCT-FCx), São Paulo, SP, Brazil; The National Institute of Science and Technology— Nanomaterials for Integrated Markers (INCT-INAMI), Recife, PE, Brazil.
Conflicts of interest statement
No conflicts of interest have been declared.