
Abstract
Objective:
The objective of this article is to evaluate the limb salvage and patency rates after crural arterial revascularization, differences between graft material and co-morbidities.
Patients and methods:
All patients with crural artery bypasses were analysed retrospectively in a single centre (Department of Vascular Surgery, Thüringen Kliniken Saalfeld, Rudolstadt, Germany) over a 10-year period (1996–2006); 157 patients with 170 consecutive arterial reconstructions could be included.
Results:
Follow-up time was 55 months (6–119). Median age of the 56 women and the 101 men at the time of operation was 70 years (45.6–93.6). The five-year secondary patency rates were 71.5 ± 6.22% (vein), 44.3 ± 10.8% (composite; p = 0.0011), 52.6 ± 13.4% (prosthetic graft with distal vein cuff/patch; p = 0.00953) and 42 ± 12% (prosthetic graft without distal vein cuff/patch; p = 0.00443). Limb salvage rates after five years were 79.5 ± 5.8%, 61.6 ± 10.3%, 77.9 ± 11.3% and 70.1 ± 14.7%, respectively. Cumulative limb salvage rate was significantly higher in diabetic patients (78.9 ± 4.9%), than in non-diabetic patients (66.6 ± 6.8); p = 0.023.
Conclusion:
Crural reconstruction is a suitable method for peripheral arterial occlusive disease to prevent amputation, particularly in diabetics.
Keywords
Introduction
Treating claudication is the target in Rutherford stages 1–3, whereas in critical limb ischemia the major target is preventing limb amputation or wound healing. Several studies have described the feasibility of femorodistal arterial reconstruction with acceptable patency (47%–76% over a five-year period) and limb salvage rates (56–72% over a five-year period), most with pre-selected patient groups.1–4 Either they include only one bypass graft type or follow-up is limited to a few years. Vein graft shows the best results and is considered the material of choice for infragenual bypass grafting. Unfortunately the saphenous veins are often of poor quality or have been used for other reasons.
In our study we describe a 10-year single-centre experience of femorodistal bypass with single- or dual-vessel outflow in a non-selected patient group. This reflects the ‘real world’, where most patients do not have any or enough suitable veins for bypass grafting. The goal of this study was to evaluate patency and limb salvage rates over a 10-year period, comparing different graft materials and co-morbidities.
Material and methods
All patients who underwent femorodistal bypass between January 1996 and December 2006 were retrospectively analysed. Included in the study were 170 consecutive bypasses; 19 were excluded because they were lost to follow-up directly after discharge. These 170 bypasses were performed in 157 patients (101 men and 56 women). The 13 bilateral bypasses were done as staged reconstructions.
We recorded the following variables: age at time of operation, co-morbidities, Rutherford stage, location of proximal and distal anastomosis, anatomic or extraanatomic reconstruction, graft material, type of surgical intervention, preoperative angiographic findings and minor or major amputation.
Surgical procedure
All patients were investigated preoperatively by digital subtraction angiography (DSA) or magnetic resonance angiography (MRA). In 155 cases, the indication was critical limb ischemia Rutherford stages 4–6. In the other cases, the reason for arterial reconstruction was severely disabling claudication (Rutherford stage 3).
For vein mapping, duplex sonography was used. Primary used veins were ipsi- and contralateral great saphenous veins (GSV) and small saphenous veins (SSV). Arm veins were not examined. GSV or SSV were used when diameter was > 3 mm, absence of reflux at the Valsalva maneuvre and no evidence of deep vein thrombosis were seen. When suitable, short vein segments for composite grafts were used, otherwise, prosthetic grafts were used.
Allografts and spliced veins were not included because they are not used at our institution. Heparin-bonded grafts and precuffed grafts were used during the last years of this study, but were excluded due to small patient numbers.
All patients were operated on in the operation room under general anaesthesia. Before arterial clamping, 2000–3000 IE heparin was administered, activated clotting times (ACTs) were checked and further heparin was administered if necessary. Intraoperative angiography was used for quality control of the distal anastomosis and run-off.
All patients were postoperatively full-dose heparinised (activated partial thromboplastin time (apTT) = 60–80 sec) for three to five days and received a standard dose (100 mg) of acetyl salicylate thereafter. Patients who received Clopidogrel or Warfarin/Phenprocoumon for other reasons continued their medication.
The used grafts were: vein grafts (n = 79), prosthetic grafts with distal vein cuff or patch (n = 23), prosthetic grafts without distal vein cuff/patch (n = 30) and composite grafts (n = 38). The majority of the vein grafts were GSV (n = 78); only one SSV was used. GSV was used in 68 cases as non-reversed, in five cases as reversed and in five cases as in-situ bypass; for overview, see Table 1.
Overview of the used graft materials.
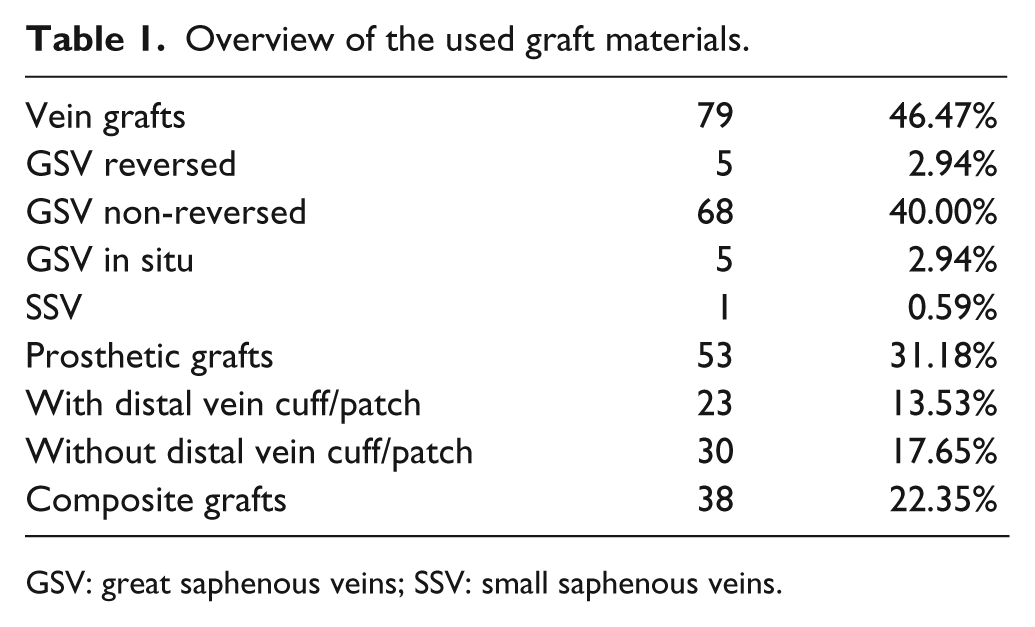
GSV: great saphenous veins; SSV: small saphenous veins.
For prosthetic grafts, standard expanded polytetrafluoroethylene (ePTFE), thin wall grafts with a 6 mm diameter and external support systems consisting of parallel rings were used.
Distribution of the distal anastomosis site was anterior tibial artery (AT) in 83 patients, followed by posterior tibial artery (PT) (n = 35), tibioperoneal trunk (TP) (n = 27) and peroneal artery (PER) (n = 25). In 56 (32.9%) cases the popliteal artery was used as inflow artery as a short bypass.
In our study 72 (42.3%) patients had previous surgical interventions before receiving an infrapopliteal bypass, with no difference between diabetics and non-diabetics. This demonstrates the progressive character of this disease.
Patients were examined directly postoperative, before discharge, six- and 12-month postoperative, and then annual. Follow-up information was obtained by measuring the ankle brachial index (ABI), colour duplex sonography and by telephone interview of the general practitioner. The bypass was determined patent when the ABI was stable and normal flow in duplex scanning was seen.
Statistics
Results were expressed as median ± standard error or median and range for quantitative variables and as percentage (%) for categorical findings. Patencies, survival and limb salvage rate were demonstrated in Kaplan-Meier survival curves. A p-value <0.05 was considered statistically significant. Differences in survival curves were assessed with log-rank test. Excel 2003 (Microsoft, Redmond, WA) and SigmaStat 3.5 (Systat Inc, San Jose, CA) were used for statistical analysis.
Results
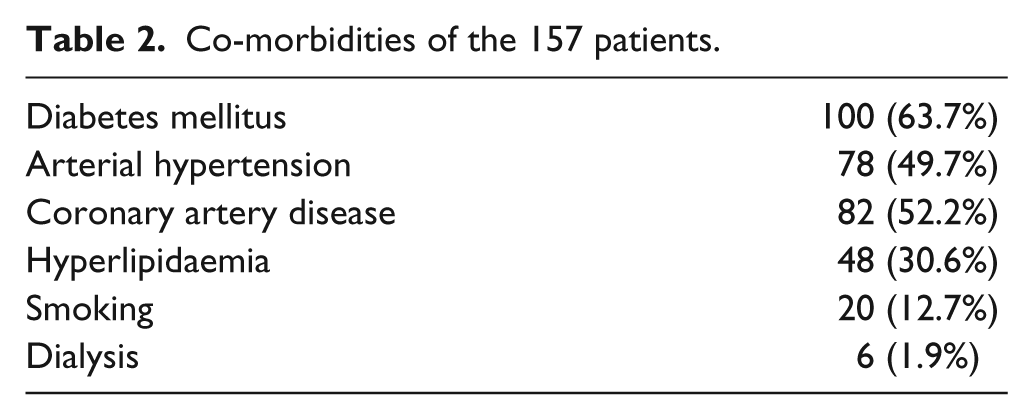
The median age at time of operation was 70.8 years (45.6–93.6). The 37 women (74.3 ± 7.3 years) were significantly (p < 0.001) older than the 63 men (67.9 ± 9.1 years). For an overview of the co-morbidities, see Table 2.
Co-morbidities of the 157 patients.
Thirteen patients needed later arterial reconstruction for the contralateral limb (eight men and five women). The in-hospital mortality was 4.7% (n = 8). Most patients (n = 6) died because of myocardial infarction. One patient died because of a severe graft infection with subsequent sepsis-induced multi-organ failure, and another patient died because of major bleeding after septic erosion of the central anastomosis, located at the aorta. The mean survival was 87.4 months; no difference was found between diabetics and non-diabetics (90.7 vs. 78.8 months; p = 0.298).
The total in-hospital reintervention rate was 14.1% (n = 24): 21 cases due to bypass occlusion, and three due to bleeding problems. Fifteen of the occluded bypass patients could be treated successfully by thrombectomy, and six patients underwent major amputation after unsuccessful therapy within the clinical stay. Six of the 21 occluded bypasses were vein grafts, eight were composite grafts, five were prosthesis with distal vein interposition and two were without distal vein cuff/patch.
During the follow-up, 17 patients underwent redo surgery; five cases were successful and 12 cases were unsuccessful.
The median follow-up period was 55 (6–119) months. After completion of follow-up, 50 bypasses were patent. From 70 occluded bypasses during follow-up, only 40 needed major amputation. In contrast nine patients underwent major amputation with patent bypass: seven for progressive infection and/or gangrene, one for septic aneurysm with deep MRSA infection, and one for knee empyema evolving from a deep bypass infection. Seven patients were diabetics (five vein grafts and two composite grafts); the target vessels were in five cases the AT and in two cases the PT. The other two patients were non-diabetics with vein grafts to the PER and to the AT. The total major amputation rate was 30% corresponding to 51 patients: eight exarticulation of the knee, 24 above-knee and 19 below-knee major amputations.
The five-year primary patency rates of the vein grafts were 59.3 ± 7.9% (standard error %), of the composite grafts 33.9 ± 15.8% (p = 0.008) and of the prosthetic grafts 45.5 ± 14.3% (p = 0.004). The p-value was p = 0.0008 (vein vs. composite grafts). No statistical significance was found between composite and prosthetic grafts (p = 0.734) and between prosthetic grafts with or without distal vein cuff/patch (p = 0.405).
The five-year secondary patency rates after autologous vein grafts were 71.5 ± 7.9%, for the composite graft 44.3 ± 10.8% (p = 0.0011), for the prosthetic graft with distal vein cuff/patch 52.6 ± 13.4% (p = 0.00953) and for the prosthetic graft without distal vein cuff/patch 42 ± 12% (p = 0.00443). No significant difference between composite and prosthetic grafts was found (p = 0.81), nor between prosthetic grafts with distal vein cuff/patch and without (p = 0.925). See Figure 1.
Life table analysis of the secondary patency rates. Vein grafts (black) showed significantly better results than composite grafts (dark red; p = 0.0011) or prosthetic grafts with distal vein cuffs/patch (dark grey, p = 0.00953) and prosthetic grafts without distal vein cuffs/patch (light grey, p = 0.00443).
No significant difference in patency rate was found between different composite grafts, between men and women (p = 0.35) and between reversed and non-reversed autologous GSV (p = 0.36).
We analysed also the patency rates for distal anastomosis site. Best results showed AT, worst results the TP. Patency rate of the PT and PER was between TP and AT. Five-year secondary patency rates were 68.08 ± 7.29% for the AT, 44.44 ± 9.57% for the TR, 52.47 ± 10.8% for the PT and 42.47 ± 8.88% for the PER. The p-values were not significant.
An extraanatomic reconstruction was used in 20 (of 80) cases to the AT and in only one case (of 35) to the PT.
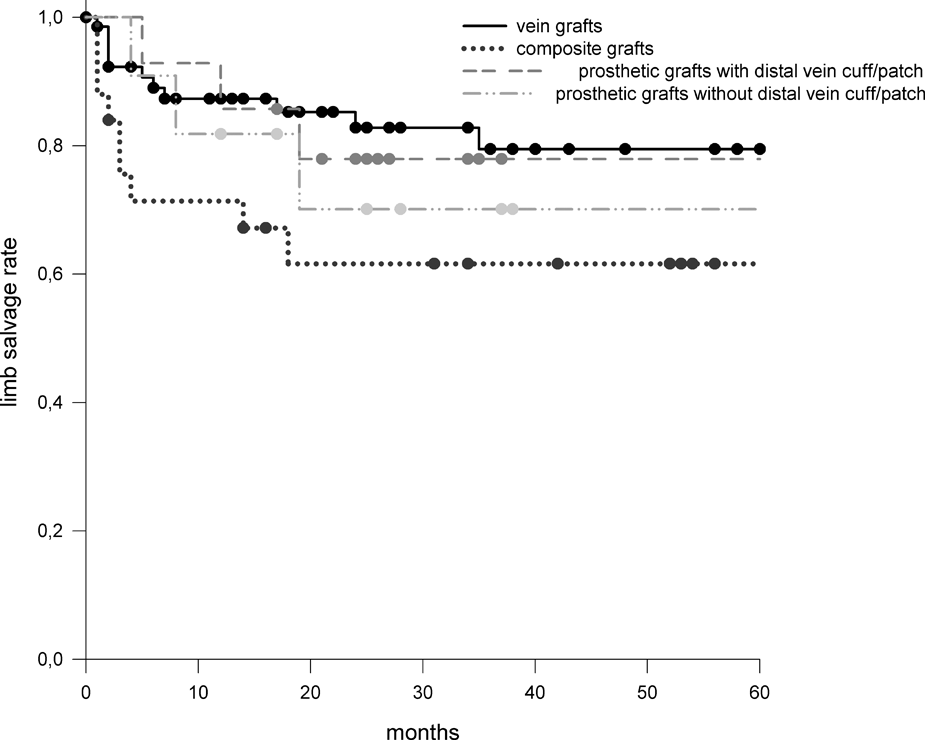
Analysis of the Kaplan-Meier table demonstrated a five-year limb salvage rate of 79.5 ± 5.8% for vein grafts, 61.6 ± 10.3% for composite grafts, 77.9 ± 11.3% for prosthetic grafts with distal vein cuff/patch and 70.1 ± 14.7% for prosthetic grafts without distal vein patch/cuff. No significant difference was found between different grafts. Between reversed and non-reversed autologous GSV (p = 0.31) and between men and women (p = 0.44), no significant difference was found. See Figure 2.
Life table analysis of the limb salvage rates of different graft types.
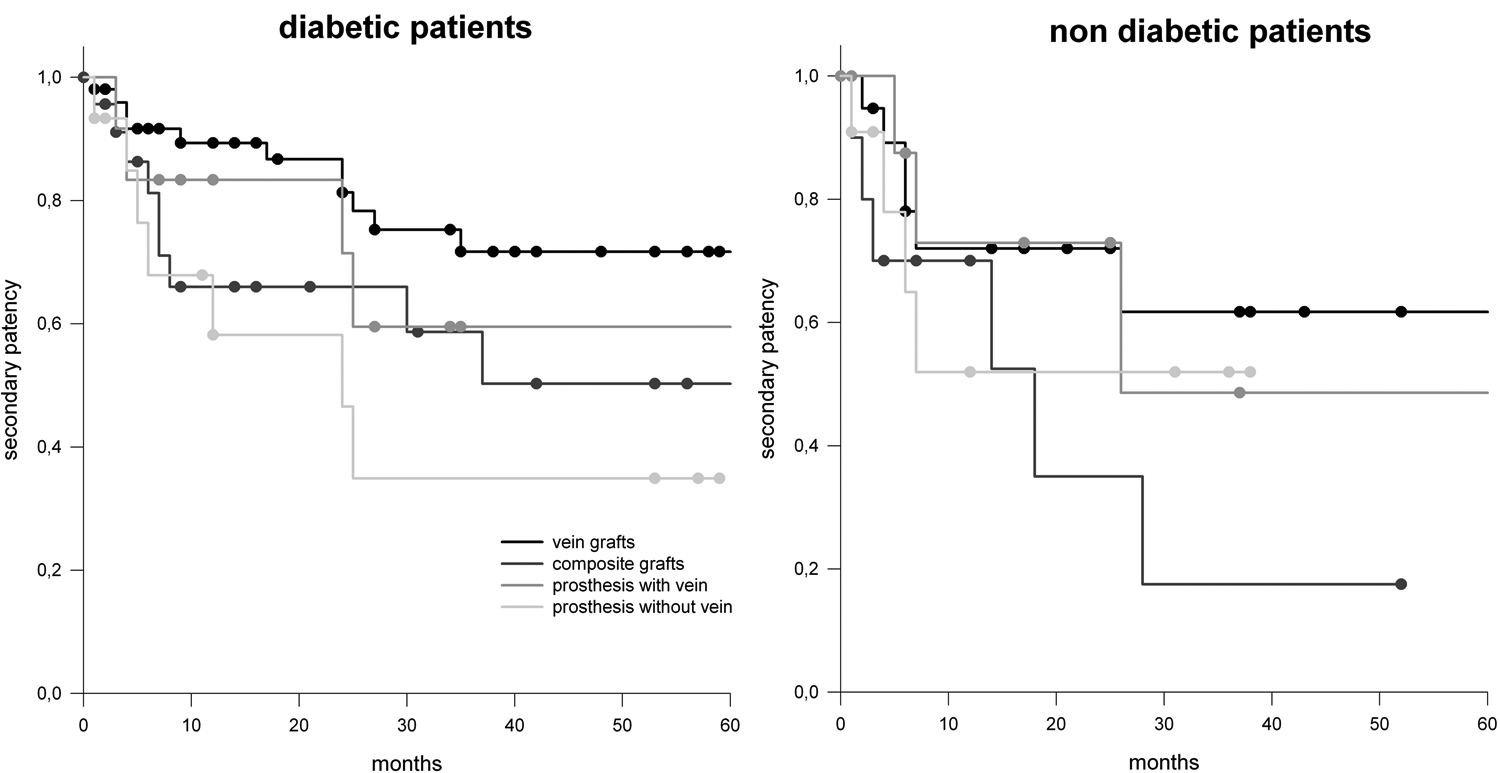
Diabetic patients showed higher patency rates of all grafts than non-diabetic patients, but without statistical significance. See Figure 3.
Life table analysis of secondary patency rates of different graft types from diabetic patients and non-diabetic patients.
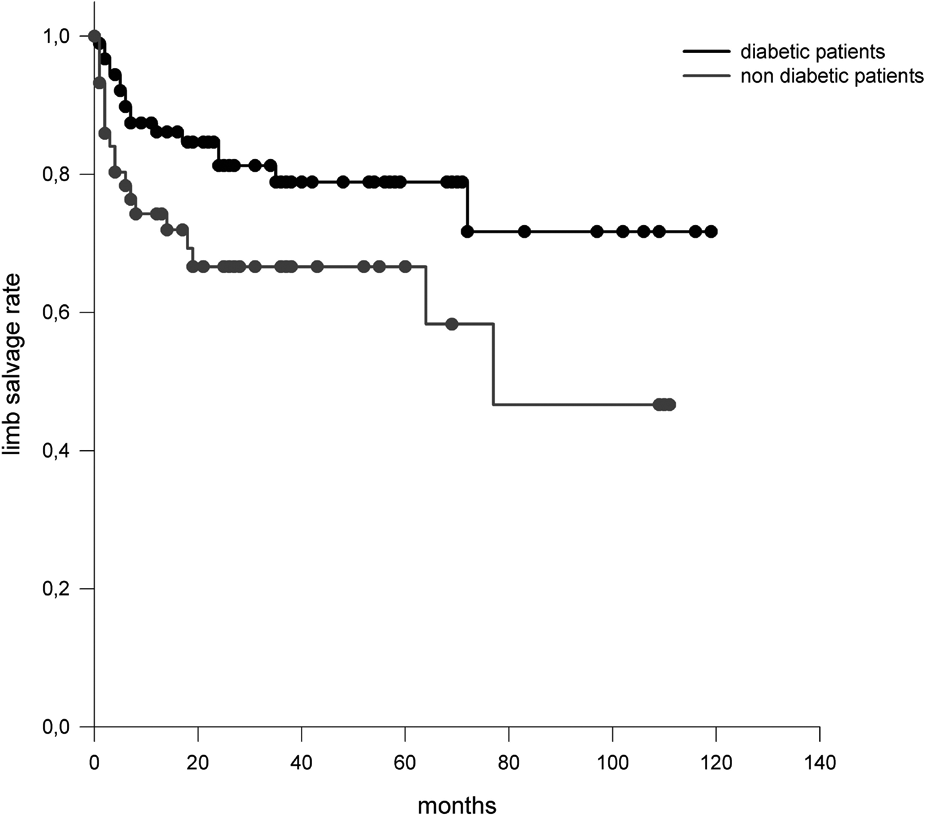
The cumulative limb salvage rate of diabetic patients was 78.9 ± 4.9% (at three years and five years) vs. 66.6 ± 6.8% (at three years and five years) in non-diabetic patients; p = 0.023. See Figure 4.

Life table analysis of limb salvage rate from diabetic patients vs. non-diabetic patients (p = 0.023).
The five-year limb salvage rate for vein grafts were 80.4 ± 7.56% in diabetics and 78.3 ± 8.62% in non-diabetics (p = 0.1145); 77.8 ± 13.9% for prosthesis with distal vein cuffs/patch in diabetics and 75 ± 21.7% in non-diabetics (p = 0.9); 75 ± 21.7% for prosthesis without distal vein cuffs/patch in diabetics and 66.7 ± 19.2% in non-diabetics (p = 0.542); 85.7 ± 9.37% for composite grafts in diabetics and 28.3 ± 15.5% in non-diabetics (p = 0.0135). The small number of patients, especially in the prosthesis groups, limits this subgroup analysis. When the 15 patients with severely disabling claudication were removed from the limb salvage calculation and only the patients with Rutherford stages 4–6 were included, the significance between diabetics and non-diabetics reaches p = 0.007.
Discussion
The major goals in advanced peripheral arterial occlusive disease are healing of chronic wounds, stopping of ischemic rest pain and limb salvage. Long patency rates are preferable but not strictly necessary. A lot of studies have been conducted but have some limitations. Some have pre-selected patient groups,1–3 others mixed up femoro-popliteal and femoro-crural bypasses.5–7 To represent a standard cohort of a vascular surgery unit, the ‘real world’, we did not exclude patients from our study except those with incomplete data or those who were lost during follow-up (directly after discharge). All patients with critical limb ischemia or ultrashort walking distance with suitable angiogram for infrapopliteal bypass grafting were included. Since no endovascular procedures in the infrapopliteal vessels were done between 1996 and 2006 (interval of patient recruitment), a pure open surgery cohort could be analysed. Only femoro-distal bypass to one crural artery (the tibial, PER or TP) were included.
Other groups used a run-off score.5–7 We included in our study only crural bypasses with a one-vessel or two-vessel (TP) run-off. In these cases we think a run-off score is not as useful as those in patients with femoro-popliteal bypasses with more than one vessel run-off.
Described five- year patency rates vary from 76% to 88% for vein grafts,8–10 from 44% to 62% for composite grafts11–13 and from 12% to 49% for prosthetic grafts.11,12
Analysis of our results showed comparable secondary patency rates. Best results showed, as expected, vein grafts, followed by composite and prosthetic grafts for short-term analysis. As for long-term results, not enough composite or prosthetic grafts were patent or not enough patients were still alive to be compared. It is noteable, however, that independent of the graft material, after the first 36 months with common graft thrombosis, a stable situation can be achieved. During this time graft occlusion is rare and may be caused by arteriosclerosis progress. This phenomenon has also been shown by other authors.14,15
The postoperative graft failure rate of 14.1% corresponds to findings by other authors.8,16,17. Luther et al. 18 describe a significantly higher patency rate for experienced vascular surgeons than forless experienced surgeons. A problem comparing both groups is the small number of operated on patients in the less experienced surgeons group. Also, in our institution the experienced surgeons had better results than others (data not shown), whereas the experienced surgeon operated on more than 60% of the patients. The indeed high postoperative failure rate is likely also due to a poor run-off.
Only 61.1% of the occluded bypasses required major amputation. In 38.9%, duration of revascularization was long enough for wound healing. On the other hand, nine patients required major amputation despite patent bypass due to progressive gangrene.
Limb salvage rate is not directly correlated with patency rates. This demonstrates the dilemma of determining the right time to amputate. Sometimes the revascularization is too late and the gangrene is too advanced for limb preservation. But it must be considered that a primary major amputation has a higher mortality rate than primary revascularization. Barshes et al. 19 reported a 9.9% 30-day mortality rate after major amputation vs. 6.5% in primary revascularization in high-risk patients.
Preoperative angiogram and in unclear cases a duplex scan were used to identify a distal anastomosis site. Distribution was comparable to that found by other authors.11,18,20 No other group investigated the patency rate of the single arteries.
We found slightly better, but statistically not significant, patency rates in diabetic patients in the first 24 months. This advantage disappears after two years, so the patency rates are comparable. Despite the equal patency rates in these two groups, we found a significantly higher cumulative limb salvage rate in diabetic patients (78.9% vs. 66.6%). When analysing the subgroups of different grafts, a statistically significant higher limb salvage rate could be found only in composite grafts. In vein grafts the limb salvage rate was higher, but not statistically significant. The prosthetic group (with or without distal vein cuff/patch) had a very small number of patients, so comparison is difficult.
Diabetics profit from crural arterial reconstruction more than non-diabetic patients based on higher limb salvage rates.1,21 This underlines that major criteria for crural bypass is not patency rate but limb salvage rate, and preservation of the leg means improved quality of life for the patient.
The reason that diabetic patients have higher limb salvage rates than non-diabetics despite comparable patency rates is not completely clear. The problem might be the different nature of gangrene or a foot ulcer. In the diabetic patient more factors than arterial hypoperfusion influence wound healing, e.g. neuropathy and inflammatory status. Even a small, superficial scar can lead to a progressive gangrene in the diabetic patient. 22 Arterial revascularisation may influence the microenvironment as well as the microangiopathy, enabling wounds to heal better.
Newer studies about heparin-bonded polytetrafluoroethylene (PTFE) grafts report better patency rates than standard PTFE grafts, but long-term results are missing.23–26 Due to the small numbers of heparin-bonded PTFE grafts used during the last years, they weren’t entered in this study.
Conclusion
Autologous veins are still the first choice for crural bypass. With increasing patient age, fewer veins are available due to harvesting for cardiac or prior peripherial revascularization or varicose changes. In these cases prosthetic or composite grafts are alternatives. In selected patients a prosthetic graft can also achieve an acceptable limb salvage rate. The best alternative for vein grafts has not yet been found. The long-term results of heparin-bonded or grafts with pre-cuffed distal anastomosis may provide further information. What we can say is that the diabetic patient receives a higher benefit from infragenicular revascularization than the non-diabetic patient.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
No conflicts of interest have been declared.