
Abstract
Cerebrovascular disease is a major cause of mortality and disability in adults. Diabetes mellitus increases the risk of cerebral ischaemia and is associated with worse clinical outcome following an event. Upregulation of matrix metalloproteinase-2 (MMP-2) and matrix metalloproteinase-9 (MMP-9) in diabetes appears to play a role in vascular complications of diabetes. We hypothesised that inhibition of MMP-2 and MMP-9 by minocycline can be potentiated by aspirin through inhibition of cyclooxygenase-2 and tissue plasminogen activator, resulting in amelioration of clinical cerebral ischaemia in diabetes. In the present study, cerebral ischaemia/reperfusion injury was induced in streptozotocin diabetic rats by 1 h middle cerebral artery occlusion and 24 h reperfusion. Infarct volume, cerebral oedema, neurological severity score and blood–brain barrier disruption were significantly increased in diabetic animals compared with the normoglycemic control group. The combination of aspirin and minocycline treatment significantly improved these parameters in diabetic animals. Moreover, this therapy was associated with significantly lower mortality and reduction in MMP-2 and MMP-9 levels. Our data indicate that combination of aspirin and minocycline therapy protects from the consequences of cerebral ischaemia in animal models of diabetes and is associated with inhibition of MMP-2 and MMP-9. Therefore, this combination therapy may represent a novel strategy to reduce the neurological complications of cerebral ischaemia in diabetes.
Keywords
Introduction
Diabetes is a major risk factor for development of ischaemic cerebrovascular disease. Patients with diabetes are at least two times more likely to have a stroke than non-diabetic subjects, and they are more prone to suffer increased morbidity and mortality after stroke. 1,2 The mechanisms by which diabetes aggravates ischaemic brain damage are not fully understood. Vascular physiological and morphological alterations are prominent in diabetes and contribute to the marked damage. It has been shown that diabetes is associated with a series of vascular alterations, including intracranial atheroma, microangiopathy, cerebrovascular atherosclerosis, rheologic abnormalities and endothelial changes. 2,3
Matrix metalloproteinases (MMPs) constitute a group of enzymes that hydrolyse protein components of the extracellular matrix (ECM). 4 The subgroup of MMPs known as gelatinases, specifically gelatinase A (MMP-2) and gelatinase B (MMP-9), digest collagen, denatured collagens (i.e. gelatins), laminin, elastin and fibronectin among other substrates, 5 and have been implicated in the pathological processes that contribute to fibrotic diseases, tumour progression and inflammation. 6-8 In cardiovascular and cerebrovascular disease, dysregulation of MMPs may have an adverse effect on various organs, resulting in tissue injury and inflammation. 9 In experimental hypertension and atherosclerosis models, for example, increased MMP activity contributes to cardiac and vascular complications. 10-13
Regulation of MMPs in diabetes has been widely investigated. It has been shown that hyperglycemia increased activity and expression of MMP-2 and MMP-9 in rat aortic smooth muscle cells and mouse vascular tissue and plasma. 14 These extracellular proteinases play a role in cerebrovascular changes and alteration of the blood–brain barrier (BBB).
In the present study we hypothesised that inhibition of MMP-2 and MMP-9 by minocycline (MINO, a known inhibitor of MMP-2 and MMP-9) can be enhanced by aspirin (ASP), secondary to cyclooxygenase-2 (COX-2) and tissue plasminogen activator (tPA) inhibitory activity of the latter (Figure 1). COX-2 and tPA can induce expression of MMP-2 and MMP-9 by different pathways. Earlier we reported that the combination of MINO and ASP was beneficial in the treatment of cardiovascular dysfunction of diabetic rats. 15 In the present study we have targeted MMP-2 and MMP-9 activation using minocycline and aspirin combination therapy, in order to improve the outcome of cerebral ischaemia in diabetic rats.
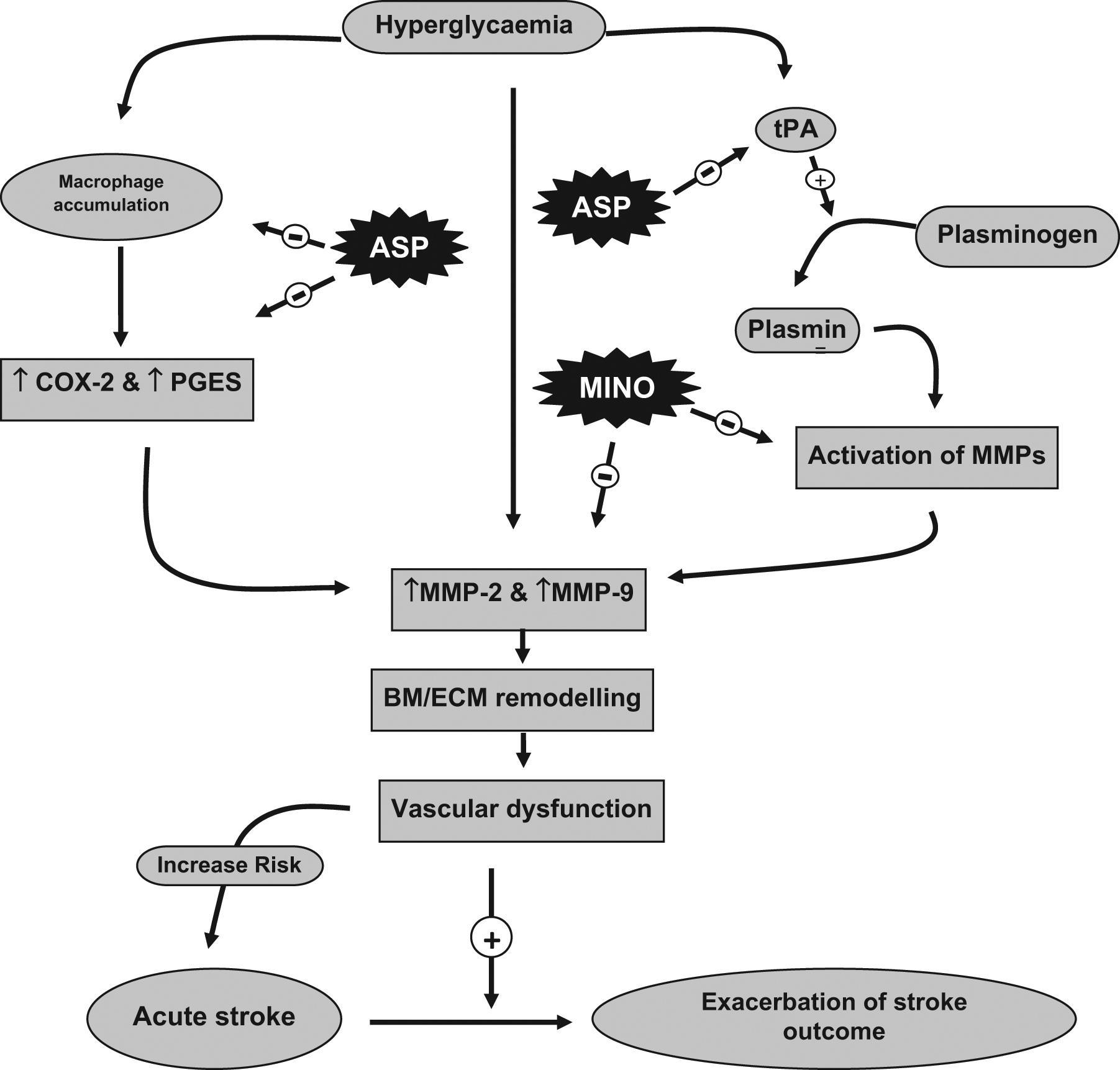
Proposed hypothesis for enhanced inhibition of MMP-2 and MMP-9 by the combination of MINO and ASP in hyperglycaemia-induced exacerbation of stroke outcome.
Materials and methods
Chemicals and drug solution preparation
Streptozotocin (STZ) and 2, 3, 5-triphenyltetrazolium chloride (TTC) were purchased from Sigma (St. Louis, MO, USA). MINO was procured from US Vitamins, India, as a gift sample. ASP was purchased from Central Drug House, India. Glucose oxidase–peroxidase (GOD/POD) glucose kit was purchased from Erba, India. All other chemicals were purchased from Merck (India). Minocycline was dissolved in distilled water. ASP was suspended in aqueous solution of 0.5% carboxy methyl cellulose (CMC). STZ was freshly dissolved in ice-cold citrate buffer (pH 4.5) solution.
Animals
Male Wistar rats (210–250 g) were purchased from the Haffkine Institue, Mumbai, India, and were housed at a temperature of 25±1°C and relative humidity of 45–55% in a clean environment under a 12:12 h light and dark cycle. The animals had free access to food pellets and filtered water was made available ad libitum. The research protocol was approved by Institutional Ethical Committee (IEC) of School of Pharmacy and Technology Management, NMIMS University Mumbai, constituted under Committee for the Purpose of Control and Supervision of Experiments on Animals (CPCSEA).
Induction of diabetes
A single dose (55 mg/kg, i.p.) of STZ was used for induction of diabetes in rats. Age-matched control rats received an equal volume of vehicle. Diabetes was confirmed after 48 h of STZ injection and again on weekly basis during the experiment. Plasma glucose levels were estimated using GOD/POD kit and rats with plasma glucose level >300 mg/dl were considered for further studies. This blood glucose level was chosen based on previous observation of extensive neuronal necrosis in all animals with plasma glucose levels exceeding approx 16 mmol/L. 16
Experimental design and drug treatment
Three weeks (1st, 2nd and 3rd) after diabetes induction, normoglycemic and diabetic rats were randomly divided into experimental groups and treated with drugs once daily for the next 3 weeks (4th, 5th and 6th) as follows.
Diabetes was induced and animals were kept untreated for 3 weeks. Afterwards drug treatments were started for next 3 weeks as follows.
The diabetic vehicle-treated Group 1 (DB+DW) was treated with distilled water (4 ml/kg, p.o., n=18); diabetic vehicle-treated Group 2 (DB+0.5% CMC) was treated with 0.5% CMC (1 ml/kg, p.o., n=19); diabetic Group 3 (DB+MINO) was treated with minocycline alone (MINO, 50 mg/kg p.o., n=16); diabetic Group 4 (DB+ASP) was treated with aspirin alone (ASP, 50 mg/kg p.o., n=16); diabetic Group 5 (DB+MINO+ASP) was treated with a combination of minocycline (MINO, 50 mg/kg p.o.) and aspirin (ASP, 50 mg/kg p.o., n=16). Age-matched normoglycemic Group 6 (NORMO) was untreated (n=16). SHAM-operated age-matched normoglycemic Group 7 (SHAM NORMO) was untreated (n=7). SHAM-operated age-matched diabetic Group 8 (SHAM DB) (n=7).
Transient focal cerebral ischaemia
Six weeks after the administration of STZ or buffer treatment, transient focal cerebral ischaemia procedures were carried out. Anaesthesia was induced by chloral hydrate (400 mg/kg, i.p.). Rectal temperature was recorded and maintained at 37°C±2°C throughout the surgical procedure and up to 2 h after reperfusion. Middle cerebral artery (MCA) occlusion was induced as described elsewhere. 17 The right common carotid artery (CCA) was exposed through a midline neck incision and was carefully dissected free from surrounding nerves and fascia from its bifurcation to the base of the skull. The occipital artery branches of the external carotid artery (ECA) were then isolated, and these branches were dissected and coagulated. The internal carotid artery (ICA) was isolated and carefully separated from the adjacent vagus nerve, and the pterygopalatine artery was ligated. Next, a 3-cm long 3-0 monofilament nylon suture was inserted up to 2 cm length via the proximal ECA into the ICA and then into the circle of Willis, effectively occluding the MCA. Neurological behaviours were examined after reperfusion, and rats without neurological abnormalities were excluded (n=5). Sham operation was performed in the same manner, except that the MCA was not occluded.
Examination of neurological symptoms
Neurological examination was performed 24 h after reperfusion before animals were sacrificed. Neurological outcome was scored on a six-point scale as described: 17 a score of 0 indicated no neurological deficit (normal); 1 (failure to extend left forepaw fully), mild focal neurological deficit; 2 (circling to the left), moderate focal neurological deficit; 3 (falling to the left), severe focal deficit; 4, rat did not walk spontaneously and had a depressed level of consciousness; and 5, stroke-related death.
Measurement of infarct and oedema volume
After 24 h of reperfusion, six rats from each group (SHAM group n=3) were sacrificed with an overdose of anaesthetic and decapitated. The brains were removed and placed in a brain matrix, and coronal sections were cut into 2-mm slices. Brain slices were immersed in 0.5% 2,3,5-triphenyltetrazolium chloride monohydrate solution at 37°C for 30 min, followed by 4% paraformaldehyde solution. The infarct area and hemisphere area of each section were traced and quantitated by an image analysis system (Scion Image, Scion; Frederick, MD, USA) and expressed as percentage of infarct area in the whole brain. The possible interference of brain oedema to infarct volume was corrected by standard methods (contra-lateral hemisphere volume - volume of non-ischaemic ipsi-lateral hemisphere), with infarcted volume expressed as a percentage of the contra-lateral hemisphere. 18
Evaluation of blood-brain barrier integrity
The integrity of the BBB was investigated using Evans Blue extravasation, according to Uyama et al. 19 At 24 h of reperfusion five rats from each group (SHAM group n=2) were injected via the jugular vein with 200 µl of 2% Evans Blue dye in PBS. The chest was subsequently opened under halothane anaesthesia 1 h later. Rats were perfused with PBS through the left ventricle at 110 mmHg pressure until colourless perfusion fluid was obtained from the right atrium. Following perfusion, brains were removed and homogenised in 4 ml of PBS. Supernatants were collected following centrifugation at 1000 × g for 5 min. Dye content within supernatants was determined spectrophotometrically at 610 nm and compared with a dilution series from an Evans Blue standard.
Vascular structure
At 24 h after ischaemic onset, three rats from each group (SHAM group n=2) were anaesthetised deeply and then perfused transcardially with ice-cold PBS, pH 7.4. MCA segments were fixed in 10% formalin, embedded in paraffin, sectioned at 4 µm, and mounted on slides. These sections were stained with Elastin Van Giesen staining using the Elastic Stain kit to stain collagen fibres. Six sections of artery from all animals were used for collagen fibre analysis. Images were captured using a CCD camera mounted in a microscope (Motic®). Area of red-coloured collagen was measured using NIH Scion Image software. The area of collagen was represented as percent value of total area measured.
Gelatine zymography
A gelatine substrate was included in the composition of the polyacrylamide/SDS gels, and samples were separated according to their apparent molecular weight by electrophoresis. After electrophoresis, the gel was washed in 2.5% TritonX-100 solution with gentle agitation for 6 h at room temperature, followed by replacement with developing buffer containing Tris base 12.1 g, Tris–HCl 63 g, NaCl 117 g, CaCl2 7.4 g, Brij-35 0.2% and distilled H2O up to 1 L. The gel was agitated at room temperature for 30 min, placed into fresh developing buffer, and incubated at 37°C overnight. The gel was stained with 0.5% Coomassie brilliant blue R-250 and de-stained in 5% methanol and 7% acetic acid. Gelatinolytic bands were quantified by scanning densitometry with NIH Scion Image software.
Statistical analysis
All values of parametric measures were expressed as mean ±SD. For parametric measures, one-way analyses of variance followed by Dunnett post-hoc test were used. All values of non-parametric measures were expressed as median (range). For non-parametric measures, neurological severity scores Kruskal–Wallis test followed by Dunn’s post-hoc test were used. All these statistical calculations were performed using statistical software Prism (GraphPad Software Inc., San Diego, CA, USA). p<0.05 was considered significant.
Results
Plasma glucose levels and body weight
STZ-induced diabetic rats showed an approximately five-fold increase in the blood glucose levels after STZ administration, which was consistent throughout the study period (Table 1). Diabetic rats showed significant decrease in body weight as compared with age-matched control rats. Treatment with MINO, ASP or with combination of MINO and ASP did not produce any change in plasma glucose levels (Table 1).
Body weight and blood sugar level (BSL) of normal and diabetic rats. The values are given as mean ± SD
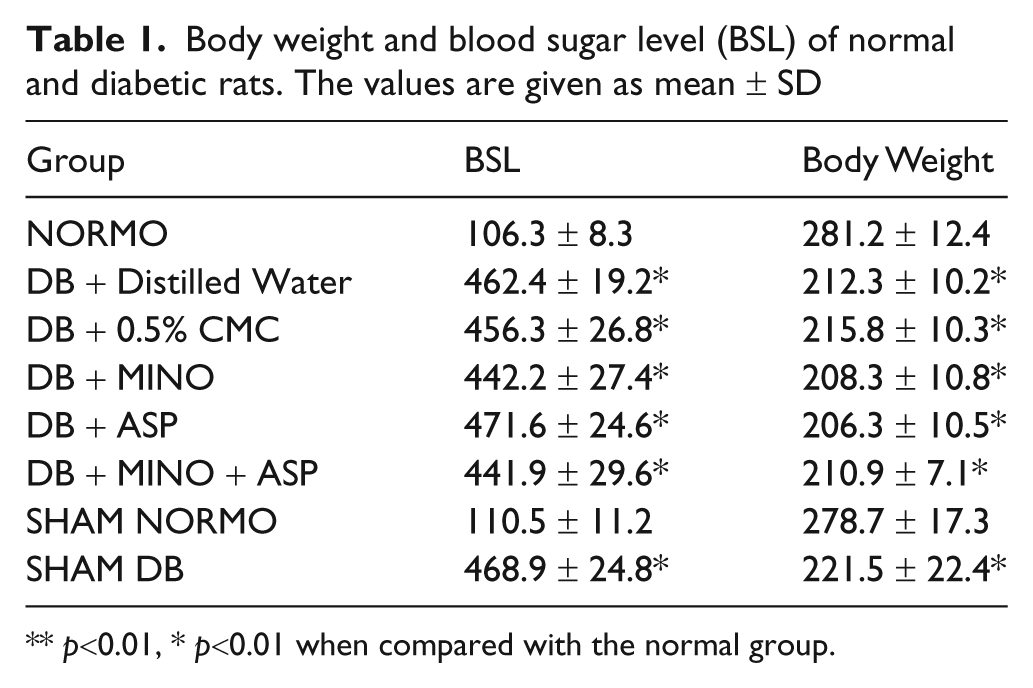
p<0.01, * p<0.01 when compared with the normal group.
Neurological severity score
Diabetes worsened outcome of cerebral ischaemia. Neurological severity score (NSS) after 24 h of reperfusion was higher in diabetic rats [4 (5–3) median (range)] when compared with normal rats [3 (3–2); p<0.05]. Three-week treatment with MINO + ASP in diabetic animals resulted in NSS comparable with the non-diabetic control group and was significantly different compared with untreated animals [3 (3–2)] (Table 2). Treatment with ASP alone and MINO alone reduced the NSS outcome, but this failed to reach statistical significance when compared with diabetic control group.
Effects of 3-week treatment with MINO alone, ASP alone and MINO plus ASP on middle cerebral artery collagen level (n=6 for all groups). The values are given as median (range)

p<0.05 vs. normoglycemic control, ** p<0.01, * p<0.05 when compared with vehicle-treated diabetic group.
NSS, Neurological Severity Score.
Cerebral infarct volume and oedema on TTC staining
Diabetes exacerbated infarct volume and percentage oedema after stroke (Figure 2). Percentage infarct and percentage oedema after 24 h of reperfusion was significantly higher in diabetic rats (24.22±4.42 and 7.79±1.27, respectively) compared with normal rats (15.48±0.70 and 3.95±0.82, respectively; p<0.05 for both). Three-week treatment with MINO plus ASP of diabetic rats significantly decreased infarct volume and oedema (16.54±0.57, p<0.05 and 5.24±1.14, p<0.05, respectively; Figures 3 and 4).
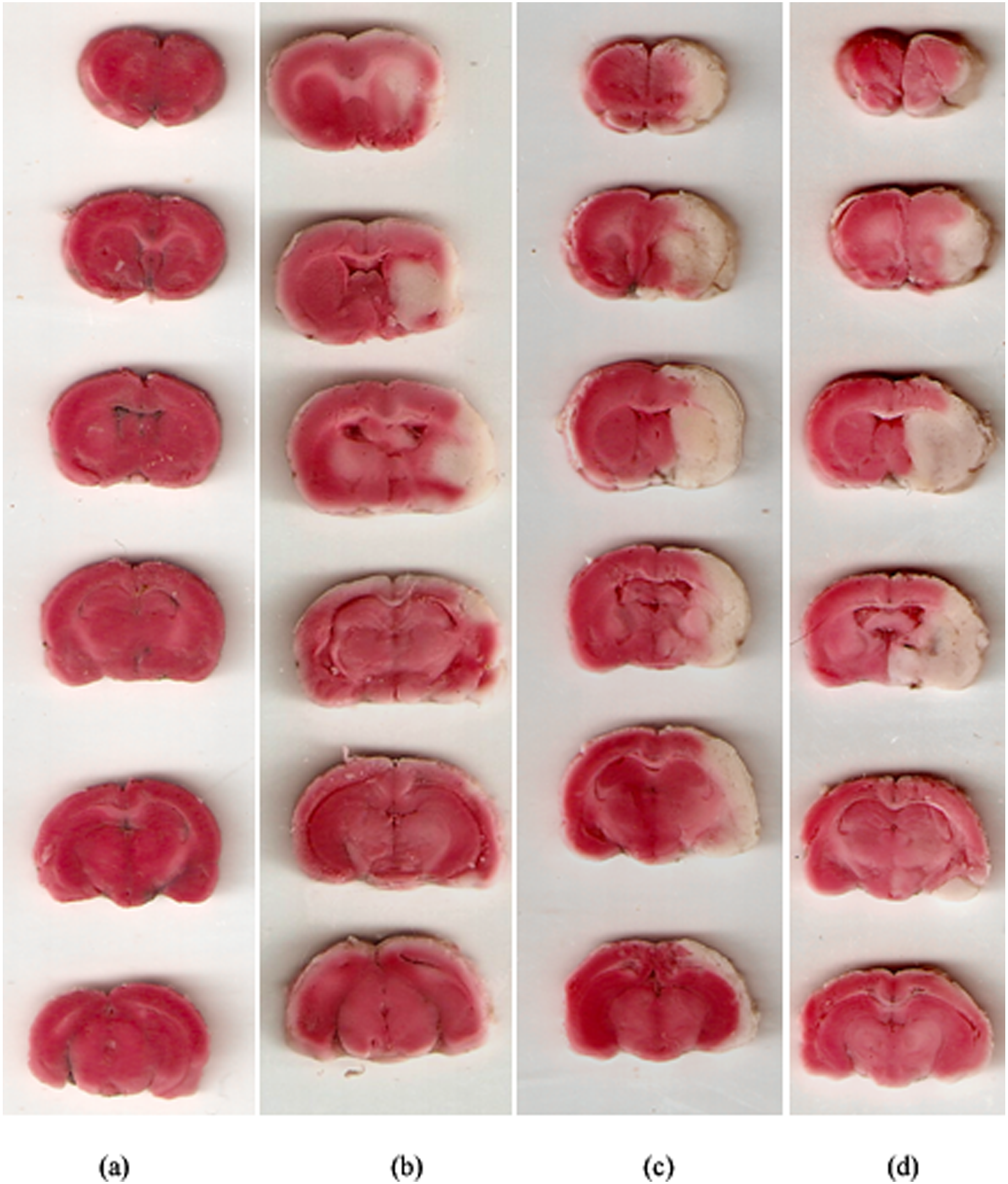
Representative images of rat brain slices stained with TTC after 1 h transient focal cerebral ischaemia: (a) SHAM (b) NORMO (c) DB + DW (d) DB + MINO + ASP.
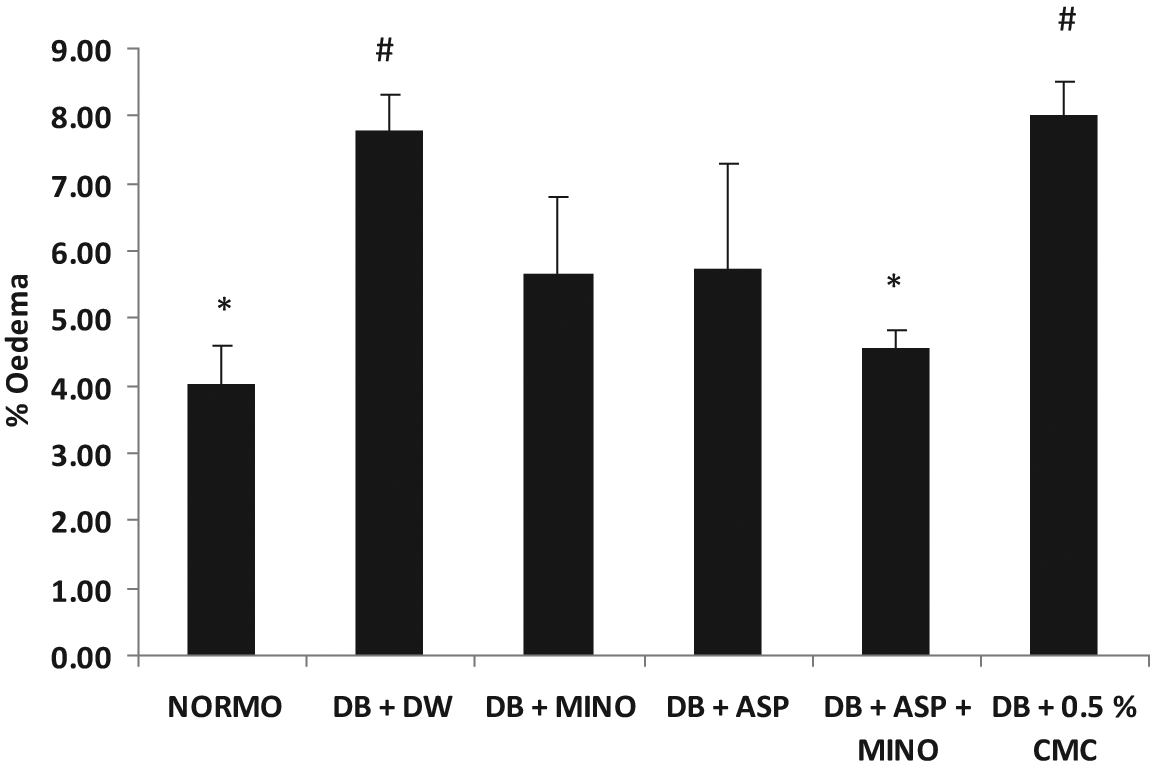
Effect of 3-week treatment with MINO, ASP and MINO in combination with ASP on vasogenic oedema after 1 h ischemia and 24 h reperfusion injury. # p<0.01 vs. normal rats, * p<0.05 vs. vehicle-treated diabetic rats (n=6 for all groups).
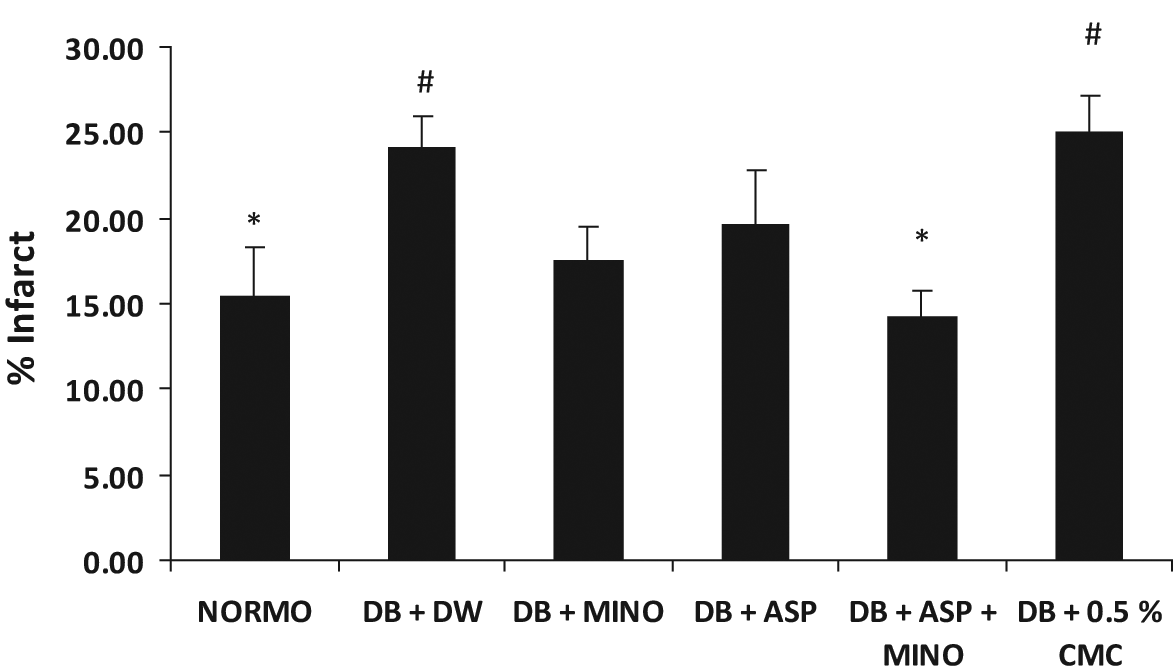
Effect of 3-week treatment with MINO alone, ASP alone and MINO plus ASP on infarct size after 1 h ischemia and 24 h reperfusion injury. # p<0.05 vs. normal rats, * p<0.05 vs. vehicle-treated diabetic rats (n=6 for all groups).
Mortality
In the vehicle-treated diabetic group mortality was found to be high. Seven of 18 DB+DW and eight of 19 DB+0.5% CMC animals died during the 60-min ischaemia or 24-h reperfusion. However, MINO+ASP-treated groups showed no mortality. Groups treated with MINO alone and ASP alone both showed reduced mortality with one and two animals, respectively.
BBB permeability
Evans Blue concentration after 24 h of reperfusion was significantly increased in diabetic rats (11.4±0.6 µg/hemisphere, p<0.05) when compared with normal rats (6.54±0.7 µg/hemisphere). Three-week treatment of diabetic animals with MINO plus ASP significantly decreased dye concentration (8.26±0.5 µg/hemisphere, p<0.05; Figure 5). Treatment with MINO alone and ASP alone showed reduction in BBB leakage, but this was not statistically significant (Figure 5).
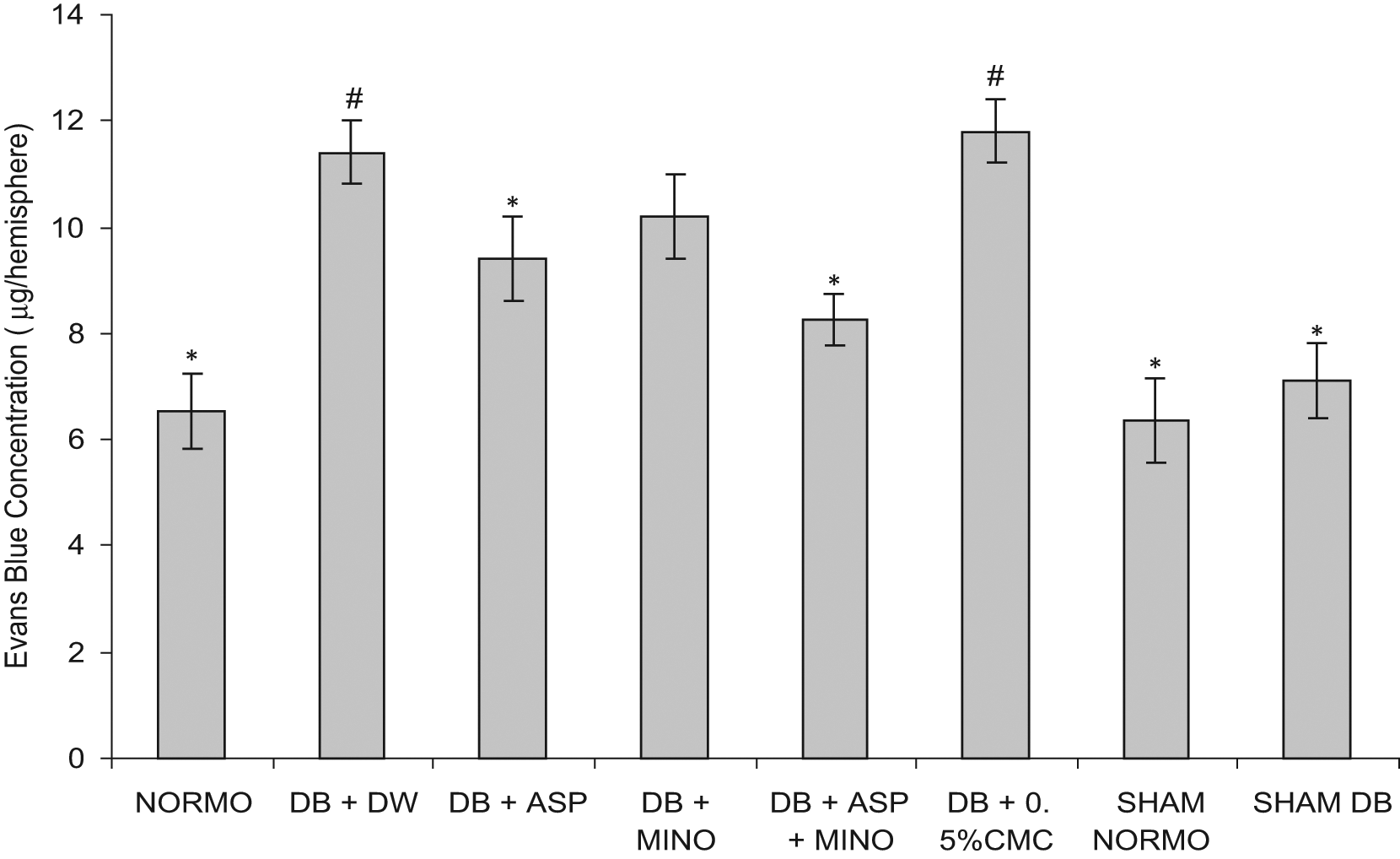
Effect of 3-week treatment with MINO alone, ASP alone and MINO plus ASP on Evans Blue permeability after 1 h ischaemia and 24 h reperfusion injury. # p<0.05 vs. normal rats, * p<0.05 vs. vehicle-treated diabetic rats (n=6 for all groups).
Vascular structure
Verhoeff-Van Gieson elastic staining was performed to determine vessel diameter and wall thickness. There was a two-fold increase in the wall-to-lumen ratio in vehicle-treated diabetic rats that was significantly reduced by treatment with MINO plus ASP (Table 3). Compared with control rats, there was increased staining for smooth muscle fibres and collagen. Diabetes was associated with increased collagen levels (34.25%±2.24) compared with control (23.78%±2.57, p<0.05). Treatment with MINO alone and ASP alone reduced the collagen level slightly but not significantly. Three-week treatment with MINO plus ASP significantly decreased the collagen level to 27.71±3.42 (p<0.01 compared with untreated diabetic group; Table 3).
Effects of 3-week treatment with MINO, ASP and MINO in combination with ASP on middle cerebral artery collagen level (n=6 for all groups). The values are given as mean ± SD
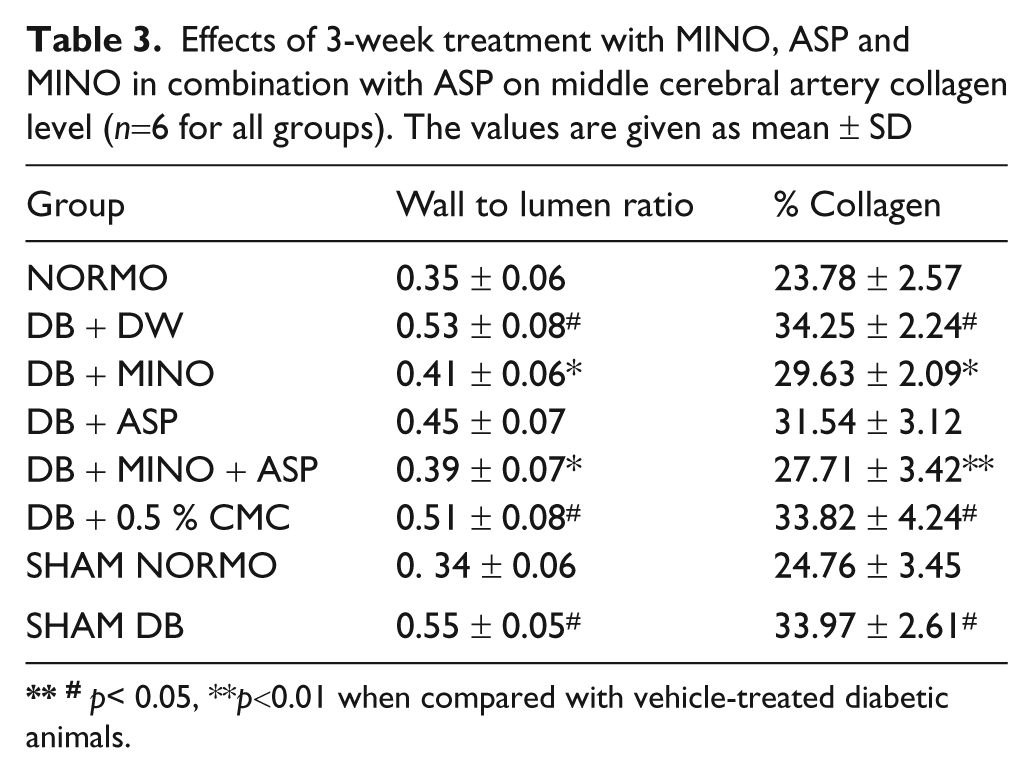
# p< 0.05, **p<0.01 when compared with vehicle-treated diabetic animals.
Gelatine zymography
MMP-2 and MMP-9 levels in brain homogenates from treated and untreated diabetic and normoglycemic rats were assessed using gelatine zymography. Zymograms of homogenates showed high MMP-2 and MMP-9 levels in vehicle-treated diabetic animals compared with normal animals (Figure 6). Treatment with MINO alone, ASP alone and MINO+ASP attenuated level of MMP-2 and MMP-9 levels. Reduction in MMP-2 and MMP-9 protein levels was more pronounced in MINO+ASP treated group compared with MINO alone and ASP alone treated group (Figure 6).
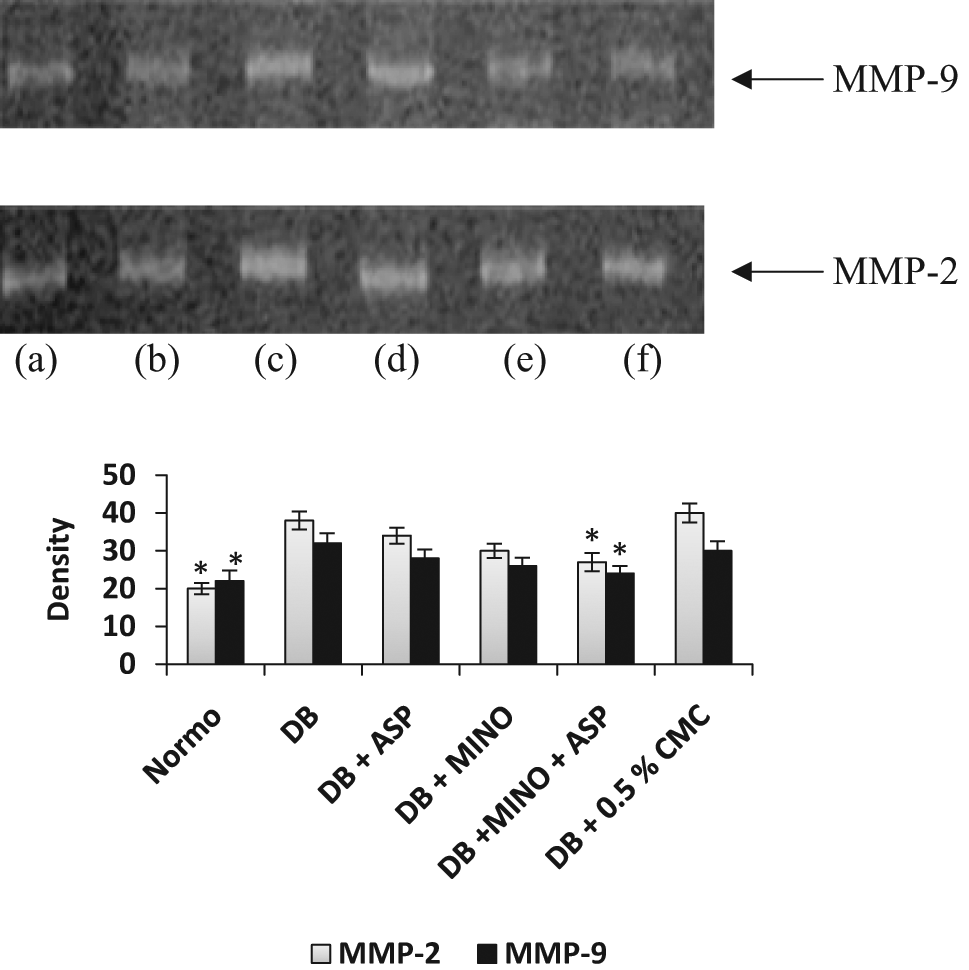
Effect of 4-week treatment with MINO alone, ASP alone and MINO plus ASP on retinal protein (MMP-2 and MMP-9) levels in type 2 diabetic rats. (a) NORMO (b) DB+ASP+MINO (c) DB+DW (d) DB+0.5% CMC (e) DB+ASP (F) DB+MINO. The graph is a densitometric analysis of MMP-2 and MMP-9.
Discussion
Cerebral ischaemia is a devastating disorder that affects the diabetic population disproportionately, and diabetes is a predictor of poor clinical outcome following an event. The various pathophysiological mechanisms of ischaemic cerebral injury that determine clinical outcome are not entirely understood. In general, larger infarct size and higher mortality rates are reported after ischaemic stroke in diabetics. 1,2 The integrity of cerebral blood vessels is critical in the pathophysiology of stroke, and diabetes-induced changes in MCA structure are important to determine extent of stroke. Data from experimental models also suggest the involvement of the extracellular protease family of MMPs. MMPs can degrade basal lamina and BBB substrates, thus leading to oedema and vascular rupture. 20-24 An emerging hypothesis states that neurovascular complications of tPA reperfusion are attributable to tPA-induced MMP-9 dysregulation. 25,26 This hypothesis has been indirectly supported by data showing that combination therapies using broad-spectrum MMP inhibitors reduce tPA-induced haemorrhagic conversion and improve outcomes in experimental clot embolic models of stroke. 27,28
In our study we used MINO in combination with ASP to reduce increased concentration of MMP-2 and MMP-9 in diabetic rats. MINO is an inhibitor of MMP-2 and MMP-9. ASP can inhibit MMP-2 and MMP-9 biosynthesis by inhibiting COX-2 and by inhibiting tPA. In diabetics, hyperglycaemia induces fibronectin (Fn) overexpression causing degradation into proangiogenic Fn fragments (Fn-f). Fn-f have been shown to stimulate tPA-catalysed plasminogen activation; the plasmin produced then activates the proform of MMP-2 and MMP-9. 29 Our findings demonstrate that hyperglycaemia for 6 weeks causes medial thickening in the cerebrovasculature, which is associated with increased gelatinase (MMP-2 and MMP-9) activity. Treatment with MINO plus ASP reduces MPP-2 and MMP-9 gelatinase activity, as evident from our zymography data (reduced level of MMP-2 and MMP-9 protein) and showed protection towards exacerbation of stroke in diabetic rats.
In the present study, diabetes resulted in a worse outcome when compared with focal MCA occlusion alone in normoglycemic rats. Others have demonstrated a similar outcome with different experimental models as well as in clinical studies. 1,2,30-35 It is established that central nervous system dysfunctions in diabetes are reflected in both structural and functional abnormalities, including impaired cognitive function, 36-40 modest cerebral atrophy, 41,42 and increased occurrence of subcortical and brain stem lesions. 43-45 Our studies are supportive of these findings, and we have demonstrated that cerebral infarction was larger in diabetic compared with normoglycemic animals. Treatment with MINO plus ASP significantly reduced these outcomes, which may be due to improvement of vascular structure, secondary to reduced MMP activity.
The present study demonstrated that hyperglycaemia significantly aggravated BBB permeability, cerebral oedema formation, and neurological symptoms after transient focal cerebral ischaemia. When BBB integrity is lost, inflammatory cells and fluid penetrate the brain, causing oedema and cell death. 46 Moreover, brain oedema is known to be an important factor in the acute phase of mortality because of the development of severe brain swelling and herniation. Earlier reports suggest that hyperglycaemia worsens outcome by increasing BBB permeability during reperfusion. 20 In our experiments BBB permeability was increased in vehicle-treated diabetic rats and reversed by MINO plus ASP treatment. This improvement is due to decreased activation of MMP-2 and MMP-9, which further leads to decreased deterioration of BBB.
The results from preclinical studies in ischaemic stroke research are interesting, and many novel agents have advanced to multicentre clinical trials; however, only a minority has been proven to be beneficial clinically. Another approach would be to concentrate on existing agents and explore the effects of combination therapy to improve outcome, guided by established pathophysiological mechanisms and known mode of action of these agents. In the present study we applied one such approach by using a combination of minocycline and aspirin for improved outcome following ischaemic stroke in animal models of diabetes.
In conclusion, the combination of MINO and ASP showed significant protection from the consequences of cerebral ischaemia in animal models of diabetes. This improvement may have been due to amelioration of vascular structure as well as inhibition of MMP-2 and MMP-9 production by the combination of these two agents.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The authors declare that they have no conflicts of interest.