
Abstract
Keywords
Introduction
Cardiovascular complications are the leading cause of morbidity and mortality in individuals with type 2 diabetes mellitus. 1 The overall prevalence of coronary artery disease (CAD) has been reported to be as high as 60% in patients with diabetes referred for stress testing. 2 Moreover, in patients with diabetes mellitus, CAD has frequently progressed to an advanced state before it becomes clinically manifest. 3
The poor clinical outcome of diabetic patients, together with the scarce clinical symptoms, demands the development of practical strategies to detect CAD at an early stage. This is particularly true for the subgroups of diabetic patients who have a very high cardiovascular risk, as those with diabetic nephropathy, clinically defined by the presence of both increased albumin excretion rate (AER) and severe diabetic retinopathy. 4,5
In clinical practice, non-invasive techniques, including myocardial Single Photon Emission Computed Tomography (SPECT) and dobutamine stress echocardiography, are used to detect CAD in asymptomatic diabetic patients. 6 A link between abnormal testing and a worse outcome has been shown to be similar to the general population. 7 Nonetheless, after normal findings, high rates of events are still observed in diabetic patients compared with non-diabetic individuals, 7 indicating a need for further refinement of prognostics in this population, as underlined by the last DIAD Study. 8
Recently, multi-slice computed tomography (MSCT) has been proposed as an alternative imaging modality to evaluate patients with known or suspected CAD. 8,9 MSCT allows anatomical, non-invasive imaging of the coronary arteries, including detection of coronary atherosclerosis by assessing the coronary artery calcium (CAC) burden (calcium score) and by performing non-invasive angiography. With the 64-slice MSCT, high sensitivity (up to 93%) and specificity (up to 96%) for the detection of significant (≥50% luminal narrowing) stenoses have been reported, and this technique has been weighed against conventional coronary angiography (CCA). 8–10
The purpose of this study was to evaluate the prevalence of CAD in a cohort of asymptomatic type 2 diabetic patients, with diabetic nephropathy and negative nuclear imaging, using MSCT angiography.
Materials and methods
Patients were referred from outpatient diabetic clinics to our Institution for assessment of cardiovascular risk. Inclusion criteria were: type 2 diabetes mellitus, age ≥40 years, persistent AER ≥30 mg/day, 11 severe diabetic retinopathy, 12 no angina or angina-equivalent symptoms, myocardial SPECT performed in the last 3 months before the study at rest and after dynamic exercise interpreted as negative for ischaemia by two independent expert physicians, after wash-out of any vasoactive drug. Asymptomatic status was confirmed using the Rose questionnaire for angina. 13
Exclusion criteria were: known or suspected CAD, history of coronary revascularisation, treatment with anti-angina medications, arrhythmias, previous congestive heart failure, previous cerebrovascular accidents, aortic stenosis, serum creatinine level ≥1.5 mg/dl and/or glomerular filtration rate (GFR) <30 ml/min, diabetic neuropathy, age ≥70 years, contraindications to iodinated contrast media, intolerance to beta-blockers, pregnancy (excluded through specific test performed within 24 h before MSCT).
Among 770 Caucasians type 2 diabetic patients screened from January 2008 through July 2010, 132 were eligible for the study. Some 638 diabetic patients were excluded: 597 did not meet all inclusion criteria and/or had one or more exclusion criteria, and 41 declined the invitation to take part in the study.
In particular, 223 (29%) were excluded because they experienced silent myocardial ischaemia during SPECT. Among them, 207 were referred for CCA, that confirmed CAD in 183 and identified 24 false-positive SPECT.
The protocol included CAC evaluation and MSCT study in all patients, and a follow-up coronary angiography only in patients with obstructive plaque (≥50% lumen narrowing), in order to execute revascularisation procedures, when possible. CAC and MSCT studies were performed within 2 months after negative stress test to exclude a progression of the disease. Coronary angiography was performed within 3–6 weeks after MSCT (Figure 1). Any metformin use was interrupted 72 h before both imaging techniques. To prevent the risk of contrast-induced nephropathy, patients received before and after the contrast intravenous normal saline hydration. In addition patients assumed daily N-acetylcysteine, 600 mg per os, starting 3 days before and continuing 3 days after the procedure. The GFR of all the patients before receiving the contrast was greater than 30 ml/min.
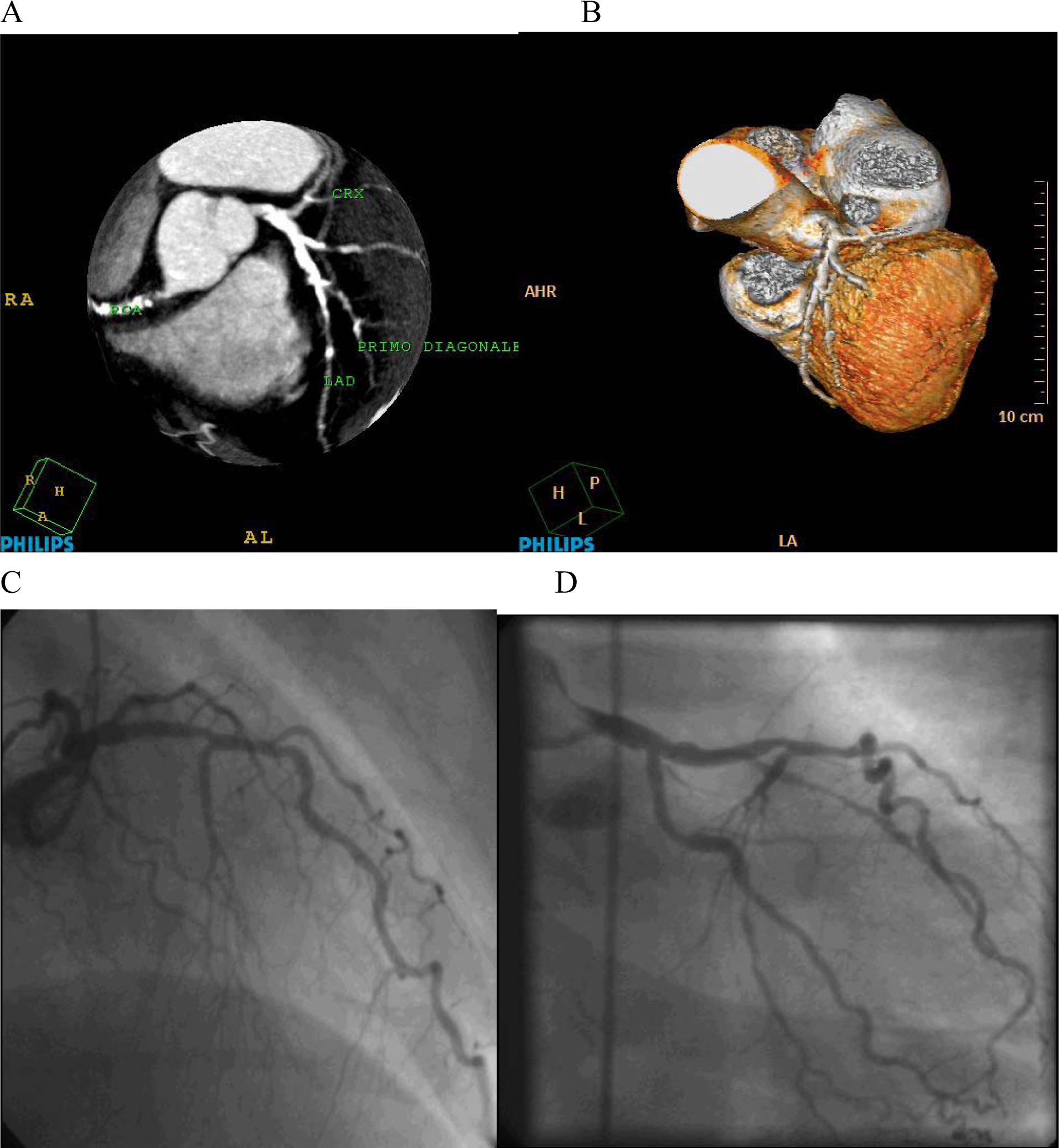
Sample case in individual with stenosed coronary arteries. Matched positive readings. In Panels A and B, respectively, Maximum Intensity Projection and 3-D reconstructions are provided, showing considerable atherosclerosis with diffuse calcifications of the left anterior descending (LAD), left circumflex (CRX) and right coronary artery (RCA). Panels C, D show the conventional coronary angiography of the same patient, that matched positive with multi-slice computed tomography, respectively: stenosis of LAD (panel C), and stenosis of CRX (panel D).
The ethical committee at the Second University of Naples approved the study design and all eligible patients signed an informed consent.
MSCT
Data acquisition
Imaging was performed using a 64-slice MSCT scanner and 0.5-mm slice thickness reconstruction (Brilliance, Philips Healthcare). To maintain heart rates <65 beats/min, beta-blocker metoprolol (2.5–5 mg, single dose i.v.) was given to 44 of 132 studied patients.
First, a prospectively triggered coronary calcium scan was performed before MSCT angiography. Sublingual nitroglycerin spray was administered (800 µg) 2 min before computed tomography angiography (CTA) scanning.
Scanning was performed at 120 KV, an effective tube current of 600–1000 mA, and data were acquired with a slice collimation of 0.625, 0.4 gantry rotation time and pitch of 0.2. The temporal window was set at 75% after the R-wave for electrocardiographically triggered prospective reconstruction.
A contrast bolus of 60 ml non-ionic contrast material was administered with a flow rate of 6 ml/sec, followed by 40 ml of iomeprole (60%) and saline chaser (40%), then by 60 ml saline chaser (Iomeron 400H, Bracco Atlanta Pharma, Konstanz, Germany). Automated detection of peak enhancement in the aortic root was used for timing of the scan. All images were acquired during an inspiratory breath hold of approximately 10 s, with simultaneous registration of the patient electrocardiogram.
Images were initially reconstructed at 75% of the cardiac cycle. In case of motion artefacts, a representative single slice was reconstructed throughout the cardiac cycle in steps of 20 ms to determine the most optimal additional reconstruction phases. Subsequently, datasets were reconstructed and transferred to a remote workstation (Extended Brilliance Workspace, Philips Medical System). A variety of 3D post-processing techniques (multiplanar reconstruction, maximal intensity projection, volume rendering and volume averaging) were performed to optimise coronary artery imaging.
In accordance with international guidelines, 14 coronary segments were classified as being normal (smooth parallel or tapering borders), as having non-obstructive disease (luminal irregularities or stenosis <50%), or as having obstructive disease (stenosis ≥50%).
None of the patients experienced arrhythmia during MSCT data acquisition, rendering the MSCT data set non-diagnostic.
Data analysis
CAC score
The CAC score was assessed with the application of dedicated software (Vitrea 2, Vital Images, USA). CAC was identified as a dense area in the coronary artery exceeding the threshold of 130 HU. An overall Agaston score was recorded for each patient. 15
Coronary plaque assessment
All angiograms were independently evaluated by two experienced observers unaware of the clinical history of the patients. In case of disagreement, a joint reading was made and a consensus decision was reached. Coronary arteries were divided into 16 segments according to the modified American Heart Association classification. 16 Only segments with a diameter >1.5 mm (as measured on the MSCT coronary angiogram) were included. First, each segment was classified as interpretable or not. Then, the interpretable segments were evaluated for atherosclerotic plaques using axial images and curved multiplanar reconstructions. Coronary plaques were defined as structures >1 mm2 within and/or adjacent to the coronary artery lumen, which could be clearly distinguished from the vessel lumen and the surrounding pericardial tissue. 16,17 One coronary plaque was assigned per segment. Finally, in accordance with the modified American Heart Association classification, 16 a threshold of 50% luminal narrowing was used to define whether the lesion was (moderately/severely) obstructive or not. For vessel-based analysis, the segments of one vessel branch were combined. The coronary tree was separated into the left main artery, left anterior descending artery, left circumflex artery and right coronary artery.
The number of diseased vessels was determined for each patient. Patients without plaques were considered normal. An abnormal MSCT was defined in the presence of ≥1 vessel disease. Significant CAD was diagnosed when at least one vessel had an obstructive stenosis (≥50% luminal narrowing).
Selective coronary angiography
All the subjects with obstructive plaque at MSCT underwent CCA, using Philips Integris 5000 equipment (Medical Philips System, Best, The Netherlands). Vascular access was obtained using femoral puncture. Coronary angiograms were evaluated by an experienced angiographer unaware of the results of MSCT. Coronary vessel segments were classified in the same way as for MSCT coronary angiography. Quantitative coronary analysis was performed offline by a resident MPS (Medical Philips System) program using the catheter tip for calibration. Stenoses were quantified only in vessels >1.5 mm in diameter. A decrease in diameter of 50–74% was defined as a moderate stenosis, ≥75% as severe stenosis. 16
Statistical analysis
Continuous variables are expressed as mean ± standard deviation. Proportions are expressed in percentages.
Comparisons between groups were made by the Student’s t-test or Chi-square test, when indicated. A logistic regression model was used to confirm the independent association of clinical characteristics with significant CAD.
Statistical analysis was performed using the Statistical Package Software System (version 12.0, SPSS Inc., Chicago, IL, USA).
Results
The clinical characteristics of the study patients are shown in Table 1.
Baseline characteristics of the study population (n = 126)
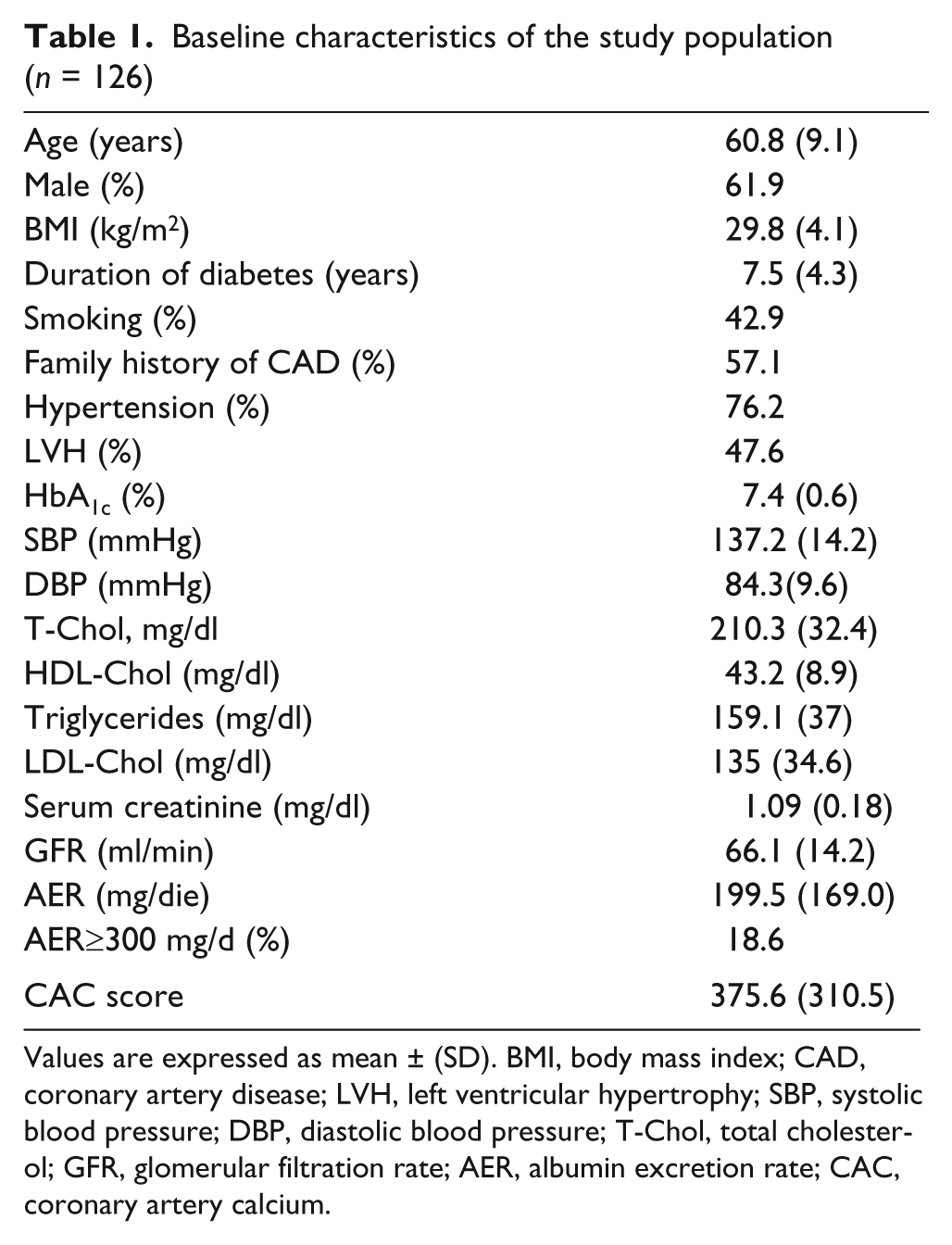
Values are expressed as mean ± (SD). BMI, body mass index; CAD, coronary artery disease; LVH, left ventricular hypertrophy; SBP, systolic blood pressure; DBP, diastolic blood pressure; T-Chol, total cholesterol; GFR, glomerular filtration rate; AER, albumin excretion rate; CAC, coronary artery calcium.
Of the132 studied patients, six (4%) were not included in the analysis because of motion artefacts. Of the remaining 126 subjects, MSCT was positive for CAD in 114 patients (90%), whereas MSCT was negative in the other 12. No patient experienced contrast nephropathy after MSCT angiography, as verified measuring GFR and potassium serum levels 24 h, 72 h and 7 days after the procedure.
Of the patients with positive MSCT, 60 (48% of all the studied patients) showed one or more significant lesions. Quantitative CCA confirmed significant stenosis (≥50%) in 48 of these 60 patients (80%). Moreover, among these 48 patients, 21 (35% of patients with positive MSCT) showed severe stenosis (≥75%). All these with severe stenosis were submitted to the revascularisation procedure (16 percutaneous coronary interventions (PCIs) and five coronary artery bypass grafting (CABG) procedures).
Each MSCT and CCA examination was also evaluated on a vessel and segmental basis. Table 2 summarises the results of obstructive stenosis at MSCT and CCA.
Detection of significant coronary artery disease through multi-slice computed tomography and conventional coronary angiography
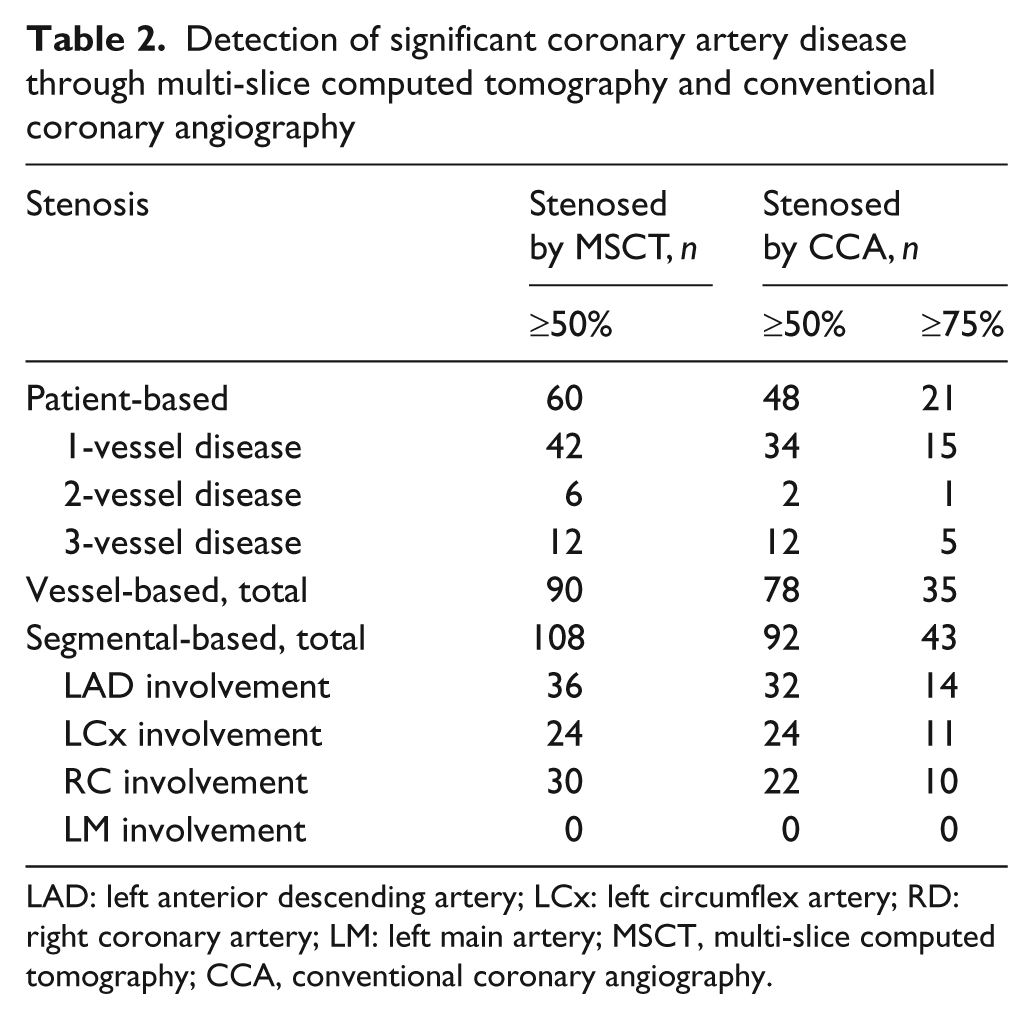
LAD: left anterior descending artery; LCx: left circumflex artery; RD: right coronary artery; LM: left main artery; MSCT, multi-slice computed tomography; CCA, conventional coronary angiography.
Notably, neither left main artery disease nor 100% vessel occlusion were observed in any patient.
The comparison between the group of patients with significant stenosis (≥50%) and the group with negative/non-significant stenosis (≤50%) at MSCT is showed in Table 3.
Comparison of patients with significant and no/non significant stenosis at multi-slice computed tomography
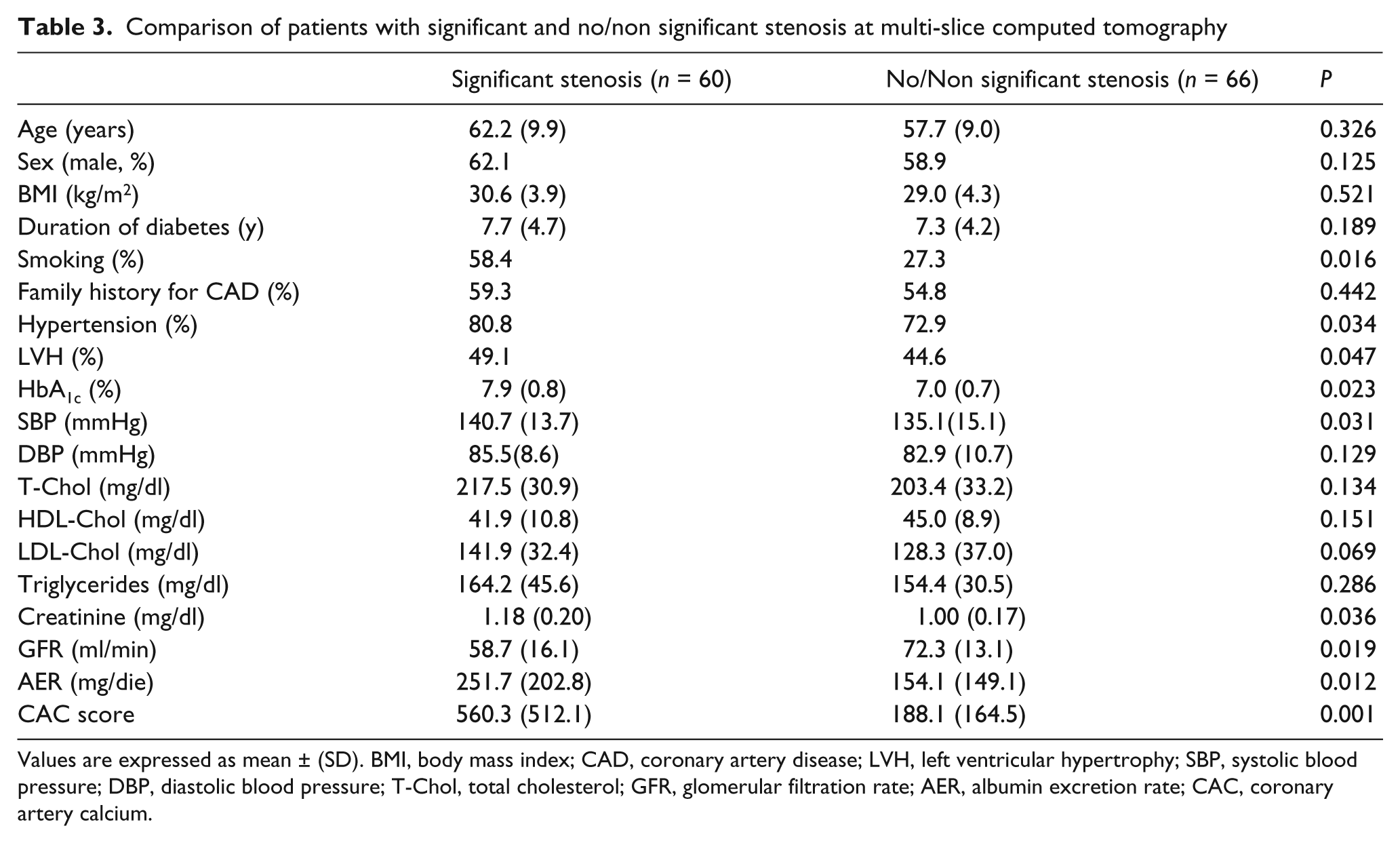
Values are expressed as mean ± (SD). BMI, body mass index; CAD, coronary artery disease; LVH, left ventricular hypertrophy; SBP, systolic blood pressure; DBP, diastolic blood pressure; T-Chol, total cholesterol; GFR, glomerular filtration rate; AER, albumin excretion rate; CAC, coronary artery calcium.
In particular, a smoking habit was more frequent in the group with significant stenosis. Laboratory data reported higher HbA1c and serum creatinine as well as lower GFR levels in the group with stenosis, while total-, low-density lipoprotein-, high-density lipoprotein-cholesterol, triglycerides and diastolic blood pressure did not reach a statistically significant difference. The group with stenosis had a higher rate of hypertension, left ventricular hypertrophy and higher values of systolic blood pressure and AER. No significant difference in duration of diabetes and body mass index was observed between the two groups. Finally, CAC value was higher in the group with stenosis. No significant difference in pharmacological therapy (hypoglycaemic agents, statins, ASA and antihypertensive drugs) was observed between the two groups.
Independent association with significant stenosis was confirmed for the following: smoking habit, HbA1c, GFR, AER and CAC score (respectively, p=0.021, p=0.033, p=0.029, p=0.018 and p=0.001).
Discussion
Our results may be summed up in two messages: first, MSCT can diagnose CAD in an asymptomatic group of patients with diabetic nephropathy; second, the study indicates in patients with significant stenosis the most important risk factors for coronary atherosclerosis.
The patients of our study were enrolled from an ordinary diabetes outpatients department. Therefore they represent the actual population of a country with its typical risk factors. Experience shows that conventional stress tests, such as exercise electrocardiography, stress echocardiography and nuclear perfusion imaging, may not be feasible and are sometimes equivocal in asymptomatic patients. Previous data revealed that MSCT shows CAD accurately and non-invasively in symptomatic populations. 18,19
We studied a specific group of asymptomatic diabetic patients, with diabetic nephropathy who are considered at high risk for CAD, to examine the value of MSCT angiography. The exclusion of patients aged over 70 and/or with diabetic neuropathy allows us to exclude the principal reasons for nociceptive dysfunction.
It is important to underline that all recruited patients had a negative stress test result by myocardial SPECT, while MSCT demonstrated CAD in 90% of the patients, and significant stenosis in 48%.
In patients with significant lesions at MSCT, lesions in 80% and severe stenosis in 35% were confirmed by quantitative CCA. All patients with severe stenosis were treated with revascularisation (PCI or CABG).
Left main artery disease as well as 100% vessel occlusion were probably identified by SPECT during the screening. Therefore, this could explain the absence of the more severe CAD in the group studied by MSCT and CCA.
Our results are similar to those from a recent study 20 where MSCT was performed in a group of symptomatic diabetic patients in primary and even secondary prevention. The high percentage of CAD in our study confirms the elevated risk of our population, along with the need to continue diagnostic examination even in the event of negative stress imaging. Asymptomatic diabetic patients were previously studied in the DIAD study, 6 showing a prevalence of silent myocardial ischaemia of 22%, assessed by adenosine technetium-99m sestamibi SPECT myocardial perfusion imaging.
Asymptomatic diabetic patients have also been evaluated using MSCT, 21 with the result of CAD in 80% of patients and significant stenosis in 26%. Although the prevalence of CAD was similar to our results (90%), significant stenoses were less prevalent (26% vs. 48%). A possible explanation for this difference could be the selection of patients: in fact, our patients had a higher prevalence of hypertension and smoking habit; moreover, all of them had diabetic nephropathy.
Appropriate clinical indications for the use of computed tomography coronary angiography and cardiac computed tomography imaging according to an expert consensus document endorsed by several professional societies was published in 2008. 14 One possible role could be to indicate whether and when MSCT may serve as an alternative (or an addition) to imaging techniques in detecting CAD. Most studies which have compared MSCT (utilising 16 detector rows) with nuclear perfusion imaging agree with a high negative predictive value of MSCT and a lower concordance of abnormalities in MSCT. 22 On the other hand, evidence for high accuracy for the detection of significant stenosis, in comparison with conventional invasive coronary angiography has been provided in patients with suspected CAD. 23 The diagnostic performance of MSCT angiography has been significantly improved with the latest 64-slice CT, with resulting high qualitative and quantitative diagnostic accuracy. 24 In our study, MSCT correctly classified all patients who had significant CAD on CCA, whereas 12 patients had significant stenosis with MSCT, but not with CCA. On the other hand, patients with negative/non-significant stenosis did not undergo coronary angiography, so we cannot define the specificity of MSCT, as a limit of the study.
A recent study 25 evaluated a group of asymptomatic type 2 diabetic patients by SPECT imaging, CAC scoring and 64-slice MSCT, concluding that the different modalities visualised different aspects of silent atherosclerosis. Anatomical evidence occurred more frequently than functional evidence, as in our study, where no functional evidence was found at all. The next great challenge is to define the relative prognostic value of each technique. Even if quantification of CAC by CT is not yet supported by strong evidence in diabetes, our study supports its possible role in a specific group of patients.
A relevant point is the risk of contrast-induced nephropathy (CIN) in patients with diabetic nephropathy. Kim et al. 26 showed that the incidences of CIN after CT were 0.0%, 2.9% and 12.1% in patients with a GFR of 45-59, 30-44 and <30 ml/min, respectively.
In agreement with these findings, very recent European guidelines 27 stated that the risk of CIN is lower after intravenous (as in MSCT) than after intra-arterial (as in CCA) contrast medium administration (at a similar dose), and considered that only patients with a GFR <45 ml/min are at risk of CIN by intravenous administration of iodinated contrast media. In addition, these guidelines agreed that volume expansion with either sodium bicarbonate or normal saline is effective in preventing CIN. Our study was performed in patients with a GFR of 66.1±14.2 ml/min. All of them received hydration before and after MSCT, and none experienced CIN. Therefore, an accurate screening of renal function is necessary before MSCT examination in patients with early diabetic nephropathy, with a value of GFR>45ml/min being safe.
Limitations
Only 126 patients, though very homogeneous because of the strict inclusion criteria, were studied, and data concerning the prevalence of atherosclerosis as determined by MSCT in larger populations are needed. Moreover, despite the excellent diagnostic accuracy of MSCT, uninterpretable segments due to motion artefacts remain problematic.
The radiation burden (10–15 mSv) of MSCT, although not higher than myocardioscintigraphy, remains a drawback of this imaging modality. However, a reduction in radiation burden is anticipated with the new generation of MSCT scanners, which are currently being developed.
Finally, the CCA was performed only in subjects with obstructive plaques at MSCT, for ethical reasons. Therefore, it is not possible to completely exclude coronary damage in subjects with unremarkable MSCT.
Clinical implications
An unresolved clinical problem is the relation between morphology and function in CAD. A very recent multicentre study 28 suggests that cardiovascular risk prediction is improved by adding asymptomatic CAD, diagnosed through coronary angiography, to routine risk assessment in type 2 diabetic patients with ≥1 additional risk factor. In particular, during a 5.4±3.5 years follow-up period, asymptomatic CAD was independently associated with a first cardiovascular event, with a risk increase greater than two-fold. These findings strongly suggest the utility of a diagnosis of CAD in asymptomatic patients at high CV risk.
In conclusion, our study showed that MSCT can detect CAD in 90% of asymptomatic type 2 diabetic patients with clinically defined diabetic nephropathy and negative myocardial SPECT. Significant stenosis was observed in a high percentage of them, and a one-third needed a revascularisation procedure for severe stenosis. Moreover, smoking habit, HbA1c level, kidney function and AER may be regarded as markers for significant coronary atherosclerosis in these asymptomatic patients. This study shows that non-invasive imaging technique MSCT may be better than myocardial SPECT in selecting patients who need CCA for a conclusive diagnosis, as well as in defining individual therapeutic strategy. A clinical follow-up of those patients with asymptomatic CAD could actually show the true clinical impact of our findings.
Finally, we imagine that the economic savings for National Health Systems, through a more intensive diagnostic effort on selected subjects at high cardiovascular risk, as in our study, could be greater than the costs of non-invasive screening up to MSCT. Further studies, also on different populations, are necessary to confirm this intriguing hypothesis.
Footnotes
Acknowledgements
Authors’ contribution: RN and OC designed and wrote the manuscript and researched data. MLMSS, RA, SE and GP researched data. NL, AP and RT contributed to the discussion and reviewed/edited the manuscript. FCS designed, wrote and reviewed the manuscript.
Grant from Italian Ministry of University and Research (PRIN).
The authors exclude any financial or other relationships that might lead to a conflict of interest.