
Abstract
Background:
Accumulating evidence indicates that dyslipidaemia plays an important role in the progression of kidney disease in patients with diabetes. Hyperlipidaemia is a risk factor for microalbuminuria in patients with diabetes. Little information exists on the prevalence and control of dyslipidaemia among diabetic patients with microalbuminuria in China. The aims of this study were to investigate the prevalence and control of dyslipidaemia among diabetic patients with microalbuminuria in a Chinese hospital as well as factors affecting the disease.
Methods:
A total of 1060 type 2 diabetic inpatients were assigned to the with-microalbuminuria group (n = 635) or the without-microalbuminuria group on the basis of urinary albumin-to-creatinine ratios (UACRs = 30–299 mg/g). Serum levels and the control of lipid profiles were assessed and classified according to the 2011 American Diabetes Association (ADA) guidelines, and low-density lipoprotein–cholesterol (LDL-C) was also assessed and classified according to Chinese intensified control criteria. Multiple regression analyses were performed to examine the factors affecting lipid variables.
Results:
Among patients with microalbuminuria, a significantly lower prevalence was found (33.1% vs. 58.6%; 35.3% vs. 52.5%, all p < 0.001) at target levels [LDL-C < 2.60 mmol/L or high-density lipoprotein–cholesterol (HDL-C) > 1.0 mmol/L for men and >1.3 mmol/L for women]. According to the intensified LDL-C goal (<2.07 mmol/L), a lower prevalence was found in male patients (15.5% vs. 32.7%, p < 0.001). Fewer patients with microalbuminuria were adherent to the therapy prescribed for dyslipidaemia (28.8% vs. 43.3%, p < 0.001). Even among patients who were on lipid-lowering treatment, the majority of individuals remained uncontrolled for all three lipid fractions [LDL-C, HDL-C and triglyceride (TG)] (82.5% vs. 69.0%, p = 0.003). Lipid and lipoprotein parameters were associated with gender and age.
Conclusion:
In China, diabetic patients with microalbuminuria displayed typical dyslipidaemias and were not adequately controlled. Intensified LDL-C and overall lipid-lowering clinical goals are potential precautions taken against diabetic nephropathy.
Introduction
Diabetic nephropathy is a common complication of diabetes mellitus (DM) and is an important cause of end-stage renal disease (ESRD) worldwide. With the increasing epidemic of DM and its complication, diabetic nephropathy, in a developing country such as China, the goal is to identify risk factors that accelerate the onset of diabetic nephropathy and to administer therapies that may retard its progression to ESRD. Accumulating evidence indicates that dyslipidaemia plays an important role in the progression of kidney disease in patients with diabetes. Hyperlipidaemia is a risk factor for microalbuminuria in patients with diabetes. 1 Findings from basic and clinical studies strongly suggest that excess amounts of a variety of lipoproteins and lipids worsen diabetes-associated microvascular and macrovascular diseases, promote glomerular and tubulointerstitial injury and contribute to the progression of diabetic nephropathy. The association between hyperlipidaemia and renal disease has led to an interest in the potential use of lipid-lowering therapies to preserve renal function. According to the 2011 American Diabetes Association (ADA) medical care recommendations, the following lipid criteria should be met for patients with diabetes: low-density lipoprotein–cholesterol (LDL-C) < 2.6 mmol/L (100 mg/dL), triglycerides (TGs) < 1.7 mmol/L (150 mg/dL) for both genders and high-density lipoprotein–cholesterol (HDL-C) >1.0 mmol/L (40 mg/dL) in men and >1.3 mmol/L (50 mg/dL) in women. 2 The Third Adult Treatment Panel of the National Cholesterol Education Program (NCEP ATPIII) designated diabetes as a “cardiovascular disease (CVD) risk equivalent” for setting treatment goals for LDL-C. 3 Recent studies suggest that lowering LDL-C to <70 mg/dL may provide even greater cardiovascular benefits, and the latest guidelines recommend <70 mg/dL as an optional LDL goal in very high-risk patients, such as those with diabetes and existing CVD. In China, dyslipidaemia control criteria recommend that an LDL-C < 2.6 mmol/L be met for diabetes patients. Moreover, an LDL-C < 2.07 mmol/L (80 mg/dL) is recommended for diabetic patients with CVD. Lipids are believed to be involved in the pathogenesis of chronic kidney disease and therefore may contribute to the high risk of cardiovascular morbidity and mortality associated with diabetic nephropathy. In addition, both cardiovascular complications and a progressive decline in renal function are associated with the coexistence of lipid abnormalities with diabetes. A more atherogenic plasma lipoprotein profile has been described in microalbuminuric type 2 diabetic patients compared with normoalbuminuric patients,4–7 and recent prospective studies have suggested that an adverse lipid profile may cause nephropathy in both type 1 and type 2 diabetic patients.8,9 High serum cholesterol levels appear to have a similar damaging effect on glomerular mesangial cells and endothelial cells, and this process seems analogous to that of atherosclerosis, since mesangial cells possess binding sites for LDL-C and oxidized LDL-C, can recruit macrophages and secrete proliferative factors. Whether this intensified LDL-C lowering goal target may be achieved pharmacologically and render profound benefits among Chinese diabetes nephropathic patients remained inconclusive.
Microalbuminuria is regarded as the earliest clinical evidence of diabetic nephropathy. It is defined as a urinary albumin excretion (UAE) of 30–299 mg/24 h in a 24-h urinary collection, 20–199 µg/min in a timed urine collection, or 30–299 µg/mg creatinine in a spot urine collection on at least two occasions within a 3- to 6-month period.10,11 The aims of this cross-sectional study were to assess dyslipidaemia, and the treatment and control of dyslipidaemia among diabetic patients with microalbuminuria in a Chinese hospital. Lipid and LDL-C levels were categorized according to the ADA recommendations and Chinese dyslipidaemia control criteria, respectively. The data will extend our understanding on finding proper clinical goals as potential precautions taken against nephropathic decline among diabetic patients in China.
Methods
Patients and data collection
The retrospective data were collected from a total of 1060 type 2 diabetic inpatients (aged ≥18 years) with or without albuminuria. Participants were admitted to Zhongda Hospital of Southeast University over 3 years (from 1 January 2006 to 31 December 2008). Data were collected by means of a case record form, which recorded demographic data, smoking status, medical history, DM and albuminuria diagnoses, and drug treatment. Body and laboratory measurements, including blood pressure, body mass index (BMI), HbA1c and lipid levels were recorded. BMI was defined as the individual’s body weight divided by the square of his or her height, and was calculated as body weight (kg)/body height (m2). Among the patients, BMI was recorded at least twice in 1 year; moreover, no evident factors affecting weight, for example, malignant tumours, existed during this period. Hypertension was defined as systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg. Fasting samples of venous blood were obtained and laboratory values were determined. The Laboratory Center of the Zhongda Hospital of Southeast University has internal and external quality control procedures directed by the Chinese Laboratory Quality Control.
Diagnosis and data classification
Patients were defined as type 2 diabetes if they qualified for one or more of the following criteria: (1) exhibiting at least twice a fasting serum glucose ≥ 7.0 mmol/L (126 mg/dL), a 2-h postprandial serum glucose ≥ 11.1 mmol/L (200 mg/dL), or a random serum glucose ≥ 11.1 mmol/L (200 mg/dL); (2) A1c ≥ 6.5%. The test should be performed in a laboratory using a method that is certified by the National Glycohemoglobin Standardization Program (NGSP) and standardized to the Diabetes Control and Complications Trial (DCCT) assay; and (3) taking antidiabetic medication. The exclusion criteria included fever, infection, pregnancy, wounds, diabetic ketoacidosis and type 1 diabetes. We prescribed additional blood tests to differentiate between a type 1 and type 2 diabetes diagnosis. These include a C-peptide test (which measures levels of this protein associated with insulin production) or tests for islet cell antibodies (ICAs), insulin autoantibodies (IAAs) and glutamic acid decarboxylase antibody (GADA).
According to the guidelines of the ADA, 12 albumin was measured in a spot urine sample, which was collected either as the first urine in the morning or at random. The results of albumin measurements in spot collections may be expressed as the urinary albumin-to-creatinine ratio (UACR).12–14 Albuminuria was defined as at least two measures of the UACR of 30 mg/g or higher, with microalbuminuria defined as an albumin-to-creatinine ratio (ACR) of 30–299 mg/g in a spot urine collection on at least two occasions within a 3- to 6-month period.10,11 Moreover, no evident factors affecting albuminuria, for instance, fever, diabetic ketoacidosis, heart failure, urinary infection or other kidney disease, existed during this period.
The lipid levels of the patients were categorized according to the 2011 ADA recommendations as in-control or out-of-control (LDL-C < 2.6 mmol/L defines in-control and ≥2.6 mmol/L defines out-of-control; an HDL-C ≤ 1.0 mmol/L and >1.0 mmol/L representing out-of-control and in-control, respectively, for men, and ≤1.3 mmol/L and >1.3 mmol/L, representing out-of-control and in-control, respectively, for women; and TGs < 1.7 mmol/L and ≥1.7 mmol/L, representing in-control and out-of-control). The LDL-C levels were categorized again according to the intensified LDL-C target recommended by the Chinese dyslipidaemia control criteria for diabetic patients with CVD (LDL-C < 2.07 mmol/L for in-control and ≥2.07 mmol/L for out-of-control). We also calculated the average total cholesterol (TC), apolipoprotein A1 (apoA1), apolipoprotein B (apoB), apoA1/apoB and lipoprotein(a) [Lp(a)] in diabetic patients with or without persistent albuminuria. The proportion of patients by gender with persistent albuminuria who were in-control or out-of-control for dyslipidaemia was compared with those without persistent albuminuria. Overall, controlled dyslipidaemia was defined as being in-control for these three lipid fractions and uncontrolled status was defined as being out-of-control for at least one of the lipid fractions.
Statistical analyses
Quantitative data were expressed as the mean ± standard deviation (SD), and qualitative variables were expressed as frequencies. The differences in discrete variables were tested by the Pearson’s chi-squared (χ2) test. Because many variables did not show a normal distribution, non-parametric statistical test was used. The Mann–Whitney U test was used to compare the mean data values between the two groups. Correlations between two variables were examined by a linear regression analysis. Independent associations between variables were evaluated by a multiple regression analysis. The p values less than 0.05 were considered statistically significant. All analyses were performed using the statistical software SPSS for Windows, version 13.5 (SPSS Inc., Chicago, IL, USA).
Results
Patients
The 1060 type 2 diabetic inpatients were assigned to one of the two groups: diabetic patients with microalbuminuria (335 men and 300 women) or without microalbuminuria (211 men and 214 women). Diabetic patients with and without microalbuminuria were matched by gender. The patients showed similar smoking histories, hypertension or elevated blood pressures, mean BMIs, and drug administration patterns, including diabetic treatments and angiotensin converting enzyme inhibitors (ACEI) or angiotensin-II type 1 receptor antagonist therapy. Diabetic patients with microalbuminuria had higher HbA1c (all p < 0.001, compared with diabetic patients without microalbuminuria by gender, see Table 1), longer diabetic duration (all p < 0.001, compared with diabetic patients without microalbuminuria by gender) and tended to be older (all p < 0.001, compared with diabetic patients without microalbuminuria by gender). In addition, diabetic women with microalbuminuria showed significantly higher serum creatinines at inclusion level (p < 0.001, compared with diabetic women without microalbuminuria).
Lipid profiles and other characteristics of dyslipidaemia among diabetic patients with microalbuminuria.
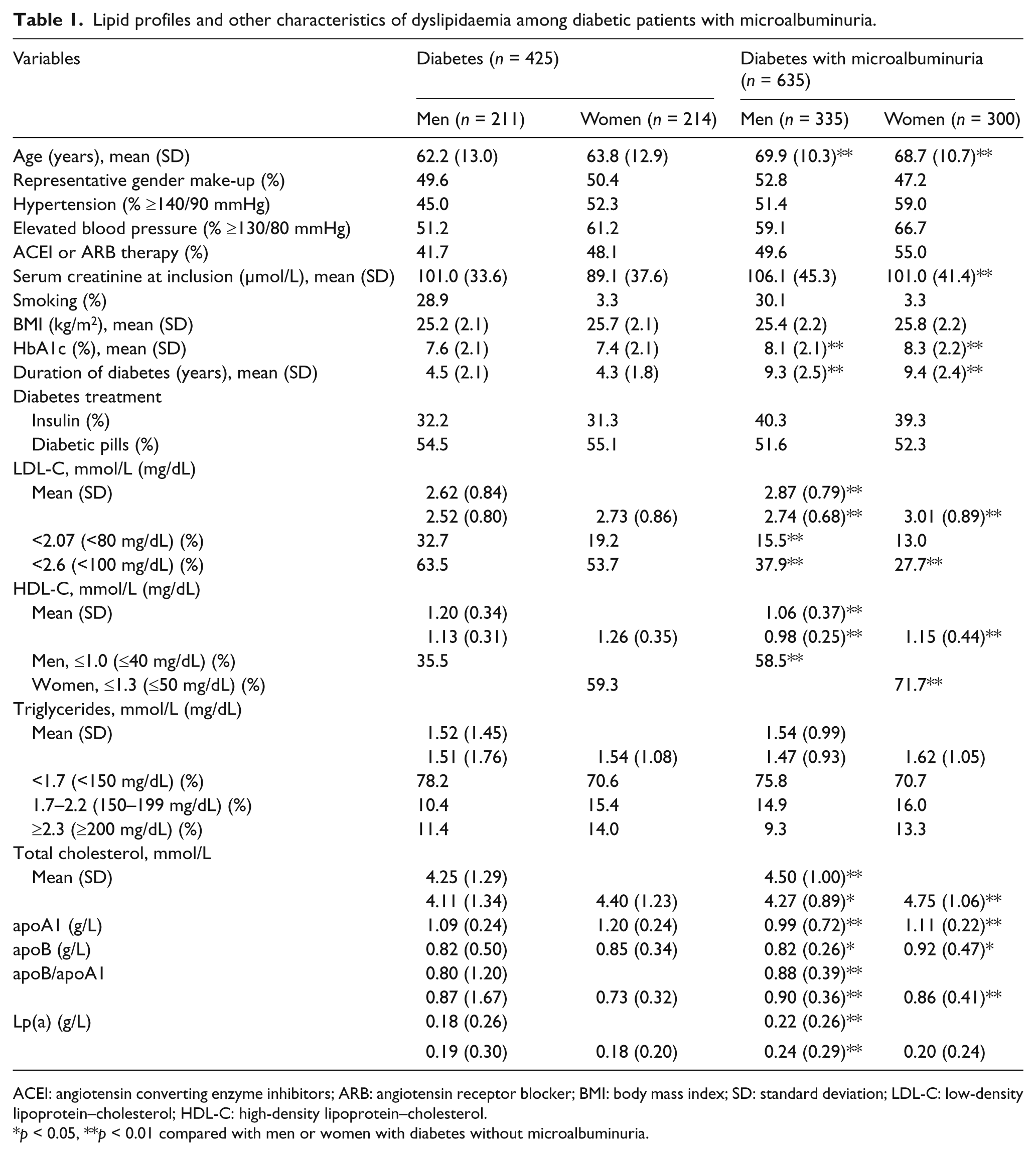
ACEI: angiotensin converting enzyme inhibitors; ARB: angiotensin receptor blocker; BMI: body mass index; SD: standard deviation; LDL-C: low-density lipoprotein–cholesterol; HDL-C: high-density lipoprotein–cholesterol.
p < 0.05, **p < 0.01 compared with men or women with diabetes without microalbuminuria.
Lipid state
Table 1 presents the lipid profiles of all the patients. LDL-C was notably higher in diabetic patients with microalbuminuria, compared with those without microalbuminuria (p < 0.001). LDL-C at the target level (<2.6 mmol/L) was less common in diabetic patients with microalbuminuria (33.1% vs. 58.6%, p < 0.001, compared with those without microalbuminuria) (Figure 1). LDL-C levels ≥2.6 mmol/L were significantly more frequent among them, compared with diabetic patients without microalbuminuria (62.1% vs. 36.5% for men; 72.3% vs. 46.3% for women, all p < 0.001). The proportion of participants with LDL-C < 2.07 mmol/L or LDL-C < 2.6 mmol/L was more frequent in the group of diabetic men without microalbuminuria versus those with microalbuminuria (32.7% vs. 15.5%; 63.5% vs. 37.9%, all p < 0.001) (Figure 2). In addition, no significant difference between diabetic women with microalbuminuria and those without microalbuminuria was found in the proportion of participants who were controlled for LDL-C < 2.07 mmol/L (13.0% vs. 19.2%, p = 0.064), whereas diabetic women without microalbuminuria more frequently had LDL-C < 2.6 mmol/L versus those with microalbuminuria (53.7% vs. 27.7%, p < 0.001).
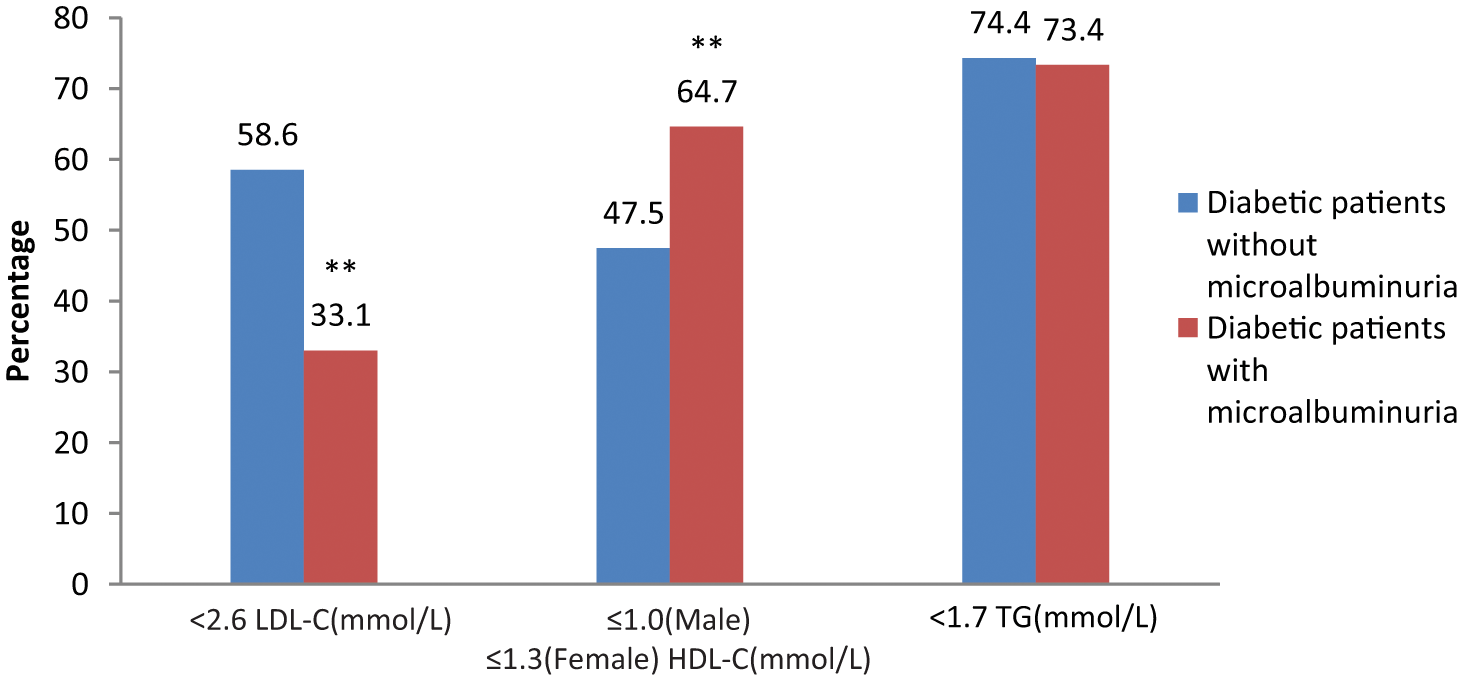
Comparison of control percentage of LDL-C (<2.6 mmol/L), HDL-C (>1.0 mmol/L for men; >1.3 mmol/L for women) and triglycerides (<1.7 mmol/L) among diabetic patients with microalbuminuria (n = 635) versus those without microalbuminuria (n = 425).
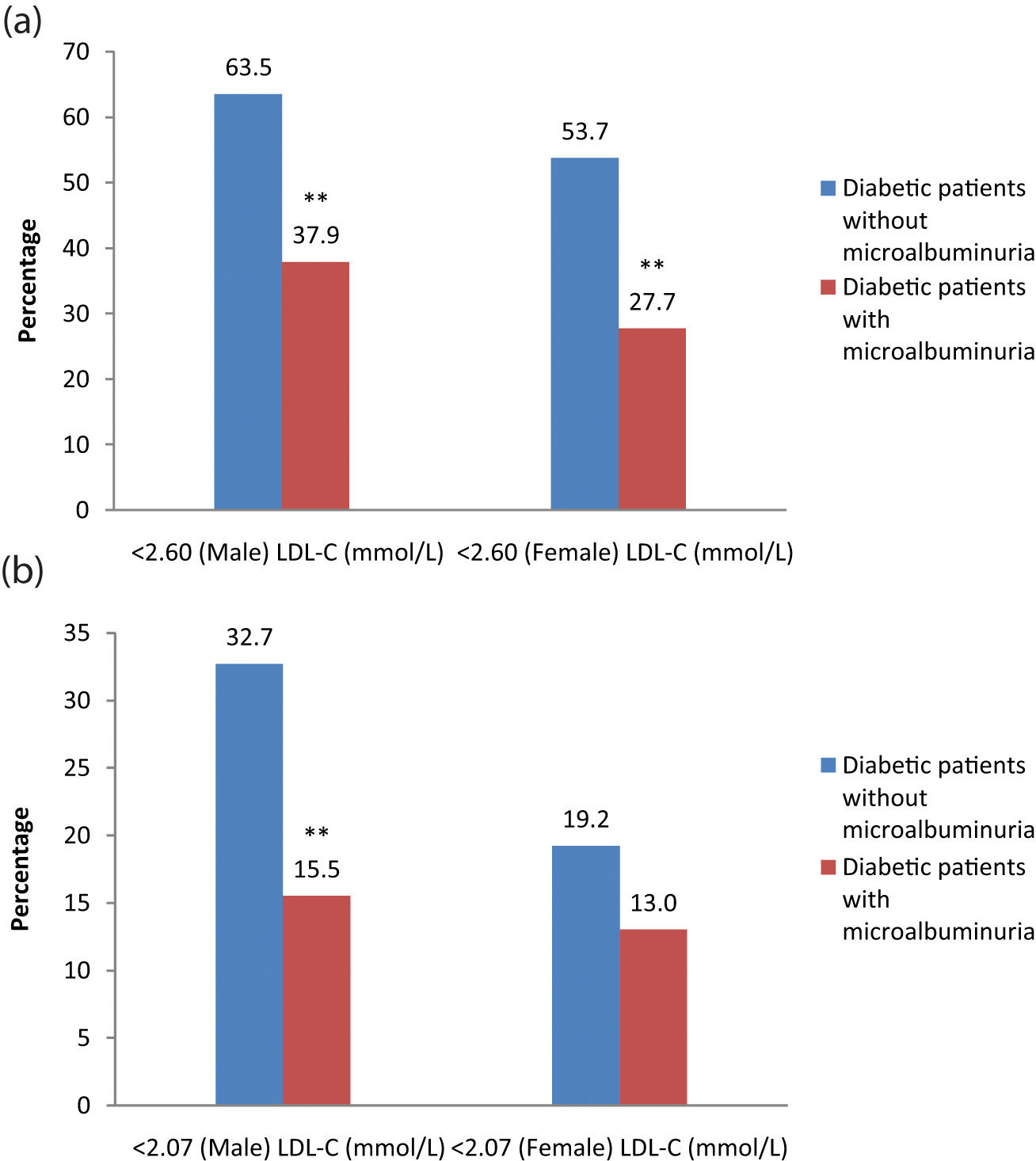
(a) Comparison of control percentage of LDL-C (<2.60 mmol/L) and (b) comparison of intensified control percentage of LDL-C (<2.07 mmol/L) by gender among diabetic patients with microalbuminuria (n = 635; 335 for men, 300 for women) versus those without microalbuminuria (n = 425; 211 for men, 214 for women).
HDL-C was notably lower in diabetic patients with microalbuminuria compared with those without microalbuminuria (p < 0.001), or by gender (all p < 0.001). HDL-C at the target level (>1.0 mmol/L for men and >1.3 mmol/L for women) was less common in diabetic patients with microalbuminuria (35.3% vs. 52.5%, p < 0.001, compared with those without microalbuminuria). A significantly larger proportion of diabetic participants with microalbuminuria had HDL-C levels ≤1.0 mmol/L for men (58.5% vs. 35.5%, p < 0.001 compared with diabetic men without microalbuminuria) or ≤1.3 mmol/L for women (71.7% vs. 59.3%, p = 0.004, compared with diabetic women without microalbuminuria).
There was no difference between the two groups in the level of TGs by gender. Moreover, the proportion of diabetic patients with controlled TGs (<1.7 mmol/L, 1.7–2.2 mmol/L or ≥2.3 mmol/L) was not significantly different between participants with and without microalbuminuria. Diabetic patients with microalbuminuria showed notably higher level of TC (p = 0.038 and p = 0.001, compared with their counterparts by gender), higher level of apoB (p = 0.046 and p = 0.044, compared with their counterparts by gender), higher ratio of apoB/apoA1 (all p < 0.001, compared with their counterparts by gender) and lower level of apoA1 (all p < 0.001, compared with their counterparts by gender). In addition, elevated lipoprotein(a) [Lp(a)] levels were displayed among diabetic men with microalbuminuria compared with their controls (p = 0.005).
Lipid-lowering therapy
Table 2 shows the treatment status of diabetic patients with and without microalbuminuria based on LDL-C levels. The data show that fewer diabetic patients with microalbuminuria were adherent to the therapy prescribed for dyslipidaemia, compared with diabetic patients without microalbuminuria (28.8% vs. 43.3%, p < 0.001). Only 18.6% of diabetic patients with microalbuminuria and LDL-C ≥ 2.6 mmol/L underwent lipid-lowering therapy, compared with 38.6% of those without microalbuminuria, indicating significant statistical difference (p < 0.001). No remarkable difference was found in the percentage of patients with LDL-C < 2.6 mmol/L, when the lipid treatment status of diabetic patient s with microalbuminuria was compared with that of patients without microalbuminuria.
Treatment status among diabetic patients with or without microalbuminuria on the basis of LDL-C level [n (%)].
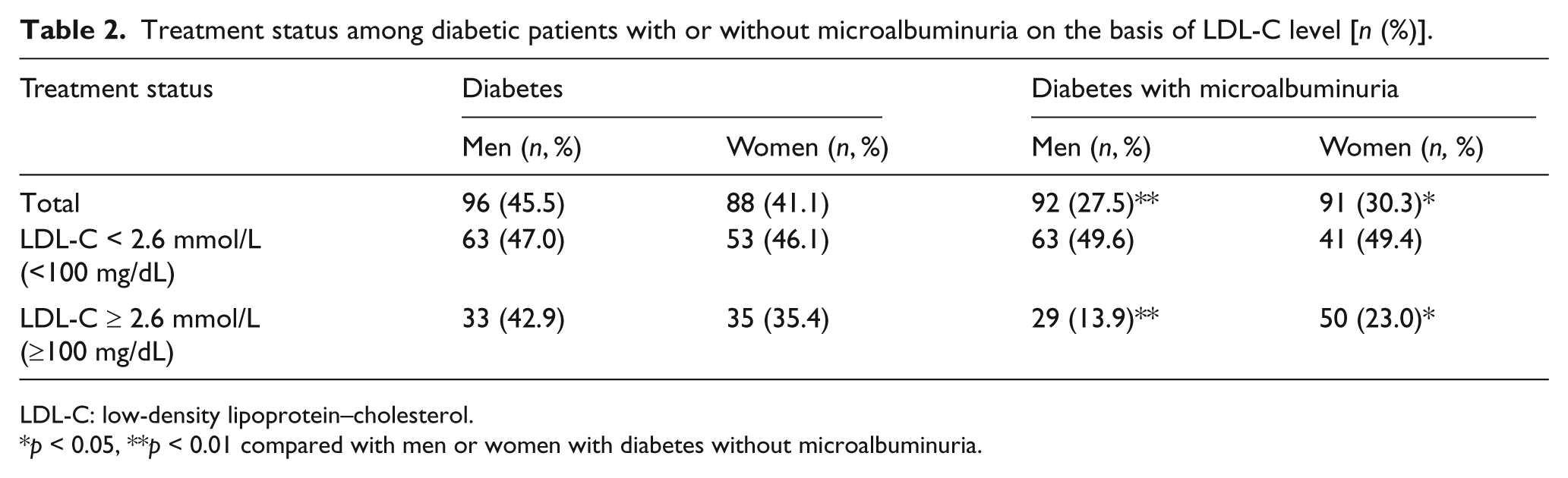
LDL-C: low-density lipoprotein–cholesterol.
p < 0.05, **p < 0.01 compared with men or women with diabetes without microalbuminuria.
Table 3 shows the lipid profiles of diabetic patients with or without microalbuminuria after lipid-lowering therapy. Even among diabetic patients who were on lipid-lowering treatment, the majority of individuals with microalbuminuria remained uncontrolled for all three lipid fractions (LDL-C, HDL-C and TGs) (82.5% vs. 69.0%, p = 0.003, compared with diabetic patients without microalbuminuria). Overall, uncontrolled dyslipidaemia was more frequent in women with microalbuminuria, despite their treatment status (p = 0.012 for treated and p = 0.001 for untreated, compared with diabetic women without microalbuminuria). For male participants with microalbuminuria, normalized levels of all three lipid fractions were rarer if they were not prescribed for dyslipidaemia treatment (10.7% vs. 27.8%, p < 0.001, compared with diabetic men without microalbuminuria).
Lipid profiles among diabetic patients with or without microalbuminuria after lipid-lowering therapy [n (%)].
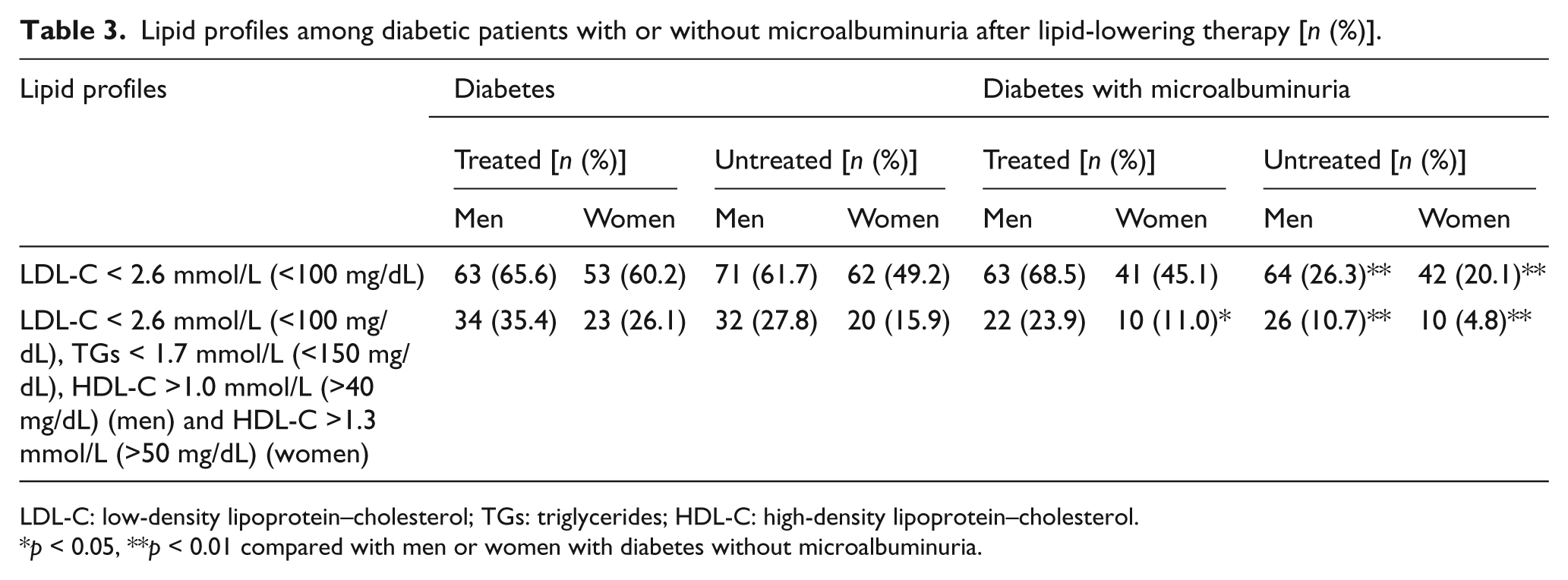
LDL-C: low-density lipoprotein–cholesterol; TGs: triglycerides; HDL-C: high-density lipoprotein–cholesterol.
p < 0.05, **p < 0.01 compared with men or women with diabetes without microalbuminuria.
Multiple regression analyses of factors affecting lipid and lipoprotein variables in 635 diabetic patients with microalbuminuria
The results showed a high prevalence of dyslipidaemia in diabetic patients with microalbuminuria, including elevations in LDL-C, TC, apoB and apoB/apoA1 ratio and reductions in HDL-C and apoA1 levels. Factors correlating with these lipid parameters in diabetic patients with microalbuminuria were examined by multiple regression analyses (Table 4). HbA1c, duration of diabetes, serum creatinine and BMI did not correlate with any of these variables. LDL-C, TC and apoB associated inversely with male gender and age. HDL-C and apoA1 showed independent positive associations with female gender. TG was inversely associated with age.
Multiple regression analyses of factors affecting lipid variables in 635 diabetic patients with microalbuminuria.
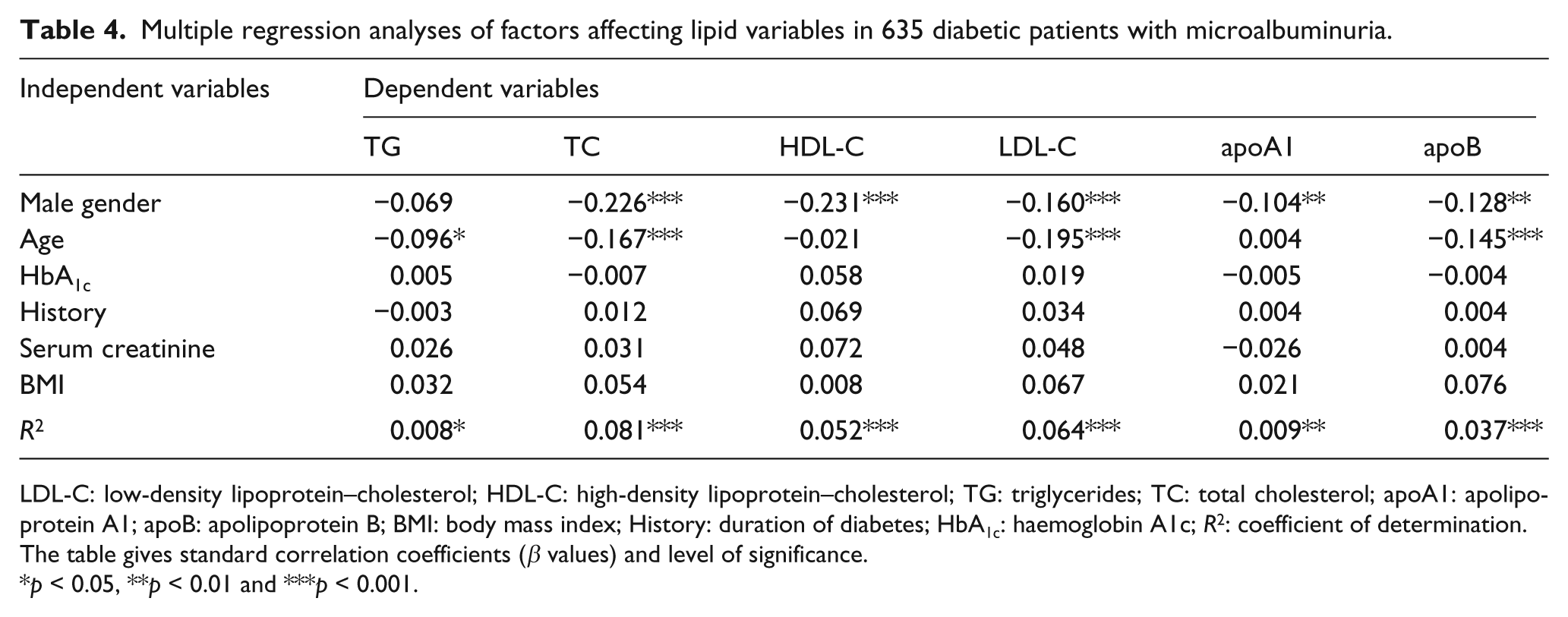
LDL-C: low-density lipoprotein–cholesterol; HDL-C: high-density lipoprotein–cholesterol; TG: triglycerides; TC: total cholesterol; apoA1: apolipoprotein A1; apoB: apolipoprotein B; BMI: body mass index; History: duration of diabetes; HbA1c: haemoglobin A1c; p2: coefficient of determination.
The table gives standard correlation coefficients (β values) and level of significance.
p < 0.05, **p < 0.01 and ***p 0.001.
Discussion
The main findings of this cross-sectional study were that diabetic patients with microalbuminuria in a Chinese hospital displayed dyslipidaemia and were not adequately controlled according to the 2011 ADA recommendations. For example, LDL-C (<2.6 mmol/L) or HDL-C (>1.0 mmol/L for men and >1.3 mmol/L for women) at target levels was significantly less common. Both lipid-lowering therapy and the target for the control of the overall lipid level were less common in the diabetic with microalbuminuria group, compared with those without microalbuminuria. When we used the Chinese dyslipidaemia control criteria of an intensified LDL-C goal (<2.07 mmol/L), a lower prevalence was found in male but not in female diabetic patients with microalbuminuria. Higher level of Lp(a) was found in male diabetic patients with microalbuminuria. Among 635 diabetic patients with microalbuminuria, lipid and lipoprotein parameters were associated with gender and age independently of other confounding factors, such as HbA1c, duration of diabetes, serum level of creatinine and BMI.
Apart from hyperglycaemia, hypertension, abdominal obesity and smoking, hyperlipidaemia is a risk factor for microalbuminuria with diabetes.1,15–21 A close relationship between serum cholesterol level and the progression of renal dysfunction in type 2 diabetic patients was found.9,22 This study showed that patients with microalbuminuria have TC and multiple lipoprotein abnormalities, but this result is inconsistent with an earlier study. 23 According to an epidemiological study reported by Shoji et al., 23 aside from TG, TC and LDL-C were not elevated in diabetic patients with microalbuminuria and were not different among the early stages of nephropathy corresponding to those with normoalbuminuria and microalbuminuria by the ADA criteria. Compared with the non-diabetic participants, HDL-C tended to be statistically lower in diabetic patients, but it was not altered in diabetic patients with or without microalbuminuria. Moreover, conflicting results were also found in TG control compared with the former studies. In our study, the proportion of diabetic patients with TGs controlled to <1.7 mmol/L, 1.7–2.2 mmol/L, or ≥2.3 mmol/L was not significantly different between participants with and without microalbuminuria. In a study of 90 patients with type 2 diabetes, Kim et al. 24 reported TGs to be a factor in the progression of diabetic nephropathy. Similarly, the UK Prospective Diabetes Study (UKPDS) reported fasting plasma TG levels to be a strong independent determinant of microalbuminuria and macroalbuminuria. 25 In prospective studies of patients with type 2 diabetes, an elevated TG-to-HDL-C ratio has been independently associated with the progression of microalbuminuria. 26 The differences in the results of these studies may have resulted from differences in sample sizes, ethnic groups, or study designs (cross-sectional or longitudinal). For example, in the Shoji study, there were 200 patients with type 2 DM, including 85 patients with ACR < 30 mg/g and 48 patients with ACR from 30 to 300 mg/g. 23 Our patients with microalbuminuria tended to be elderly and to have had diabetes longer than those with normoalbuminuria. In the Shoji study, patients with normoalbuminuria and microalbuminuria were age matched and had similar durations of diabetes.
Our data showed that the percentage of patients with an in-control LDL-C target goal (value < 2.6 mmol/L, according to the 2011 ADA medical care recommendations) was less common in male or female diabetic participants with microalbuminuria. Lipid-lowering therapy is almost always required in diabetic patients with chronic kidney disease, since an LDL goal of ≤70 mg/dL has been suggested in such high-risk patients. 27 A recent review discussed the pathophysiological links between microvascular complications, especially nephropathy, and an increased risk of cardiovascular events in type 2 diabetes patients. 28 It was implicated that the treatment of diabetic nephropathy can lower the prevalence of cardiovascular events. Chinese dyslipidaemia control criteria recommend an intensified therapy to meet the LDL-C goal (<2.07 mmol/L, equal to 80 mg/dL), which has been shown to be effective in reducing cardiovascular morbidity and mortality in diabetic patients with hyperlipidaemia. Our results indicated that male diabetic patients with microalbuminuria may benefit from this intensified LDL-C goal. Lipid-lowering therapy might be able to prevent microvascular complications, independent of its action on lipid levels through pleiotropic effects.29,30 The pleiotropic effects of statins include actions on endothelial dysfunction, vascular endothelial growth factor (VEGF) and inflammatory pathways. 29 A meta-analysis of 13 studies examining the effect of lipid-lowering therapy on the progression of chronic kidney disease showed a lower rate of glomerular filtration rate (GFR) decline with treatment compared with controls. 31 A more recent meta-analysis of the effects of statins on albuminuria showed significant decreases, reaching 48%, in microalbuminuric participants (UAE 30–300 mg/day). 32 However, the effect of statins on renal outcomes was not statistically significant in patients with diabetic nephropathy. 33
HDL-C was reduced in the diabetic patients, as reported in previous studies34–38 and our recent study. 39 In this study, HDL-C was also decreased in diabetic patients with microalbuminuria. Sibley et al. 38 reported that HDL-C was independently associated with urinary albumin but not with creatinine clearance in diabetic patients. Studies in endothelial cell cultures have demonstrated that HDL-C suppresses the expression of markers of inflammation and cell-adhesion molecules (which are markers of endothelial dysfunction). 40 Elevated levels of circulating cell-adhesion molecules and systemic markers of inflammation occur in the early stages of diabetic and non-diabetic renal disease and are cardiovascular risk factors. These data indicated that the reduction of HDL-C levels is associated with an increased risk of diabetic nephropathy in type 2 diabetic patients, as reported for type 1 diabetic patients. 41
Evidence for the roles of the atherogenic lipids in the pathology of diabetic nephropathy also come from our Lp(a) and apolipoprotein (apo) data. Lp(a) is a subclass of lipoprotein that is potentially atherogenic and is a known risk factor for CVD. 42 Epidemiological studies have reported that an increased Lp(a) level is associated with ischaemic heart disease and diabetic nephropathy and that Lp(a) is present in higher levels in patients with diabetes than in non-diabetic patients. 43 A study in Taiwan 44 showed that Lp(a) levels were similar for normoalbuminuria and microalbuminuria but increased significantly at the macroalbuminuric stage. On the other hand, apoB was elevated in the early microalbuminuria stage and remained at similarly high levels throughout the later stage of macroalbuminuria. Accumulating data suggest that apo is a more accurate cardiovascular risk marker than conventional lipids, for example, LDL-C.45–47 The level of apoB indicates the number of potentially atherogenic lipoprotein particles, and apoA1 reflects antiatherogenic HDL particles. The higher level of Lp(a) and the apoB/apoA1 ratio has been shown to be potentially related to the risk of diabetic nephropathy and may indicate that atherogenic factors play a role in the development of diabetic nephropathy.
The interpretation of the data presented in this study has certain limitations. First, the data in this study only show an association between dyslipidaemia and microalbuminuria, not a cause and effect relationship. A recent study 48 indicated that a significantly positive correlation exists between the prevalence of microalbuminuria and the corresponding components of metabolic syndrome. Patients with metabolic syndrome, including a clustering of obesity, hypertension, insulin resistance and dyslipidaemia, frequently have microalbuminuria, which is an early sign of renal impairment. CVD risk factors may cause vascular injury and direct kidney damage. It is also possible that kidney dysfunction can contribute to hypertension and promote other CVD risk factors, including insulin resistance and dyslipidaemia leading to ongoing vascular damage. These complications lead to a vicious cycle of ongoing endothelial damage and dysfunction of target organ, such as the kidney. 49 Further studies including a cohort with and without microalbuminuria and no diabetes will be helpful.
In summary, this study demonstrated that Chinese diabetic patients with microalbuminuria display a lower achievement of goals for lipid levels. While the interpretation of the data presented in our study has certain limitations, the findings indicate that microalbuminuria develops in many Chinese diabetic patients with dyslipidaemia. Intensified LDL-C and overall lipid-lowering clinical goals are potential precautions that could be taken against the development of diabetic nephropathy.
Footnotes
Acknowledgements
Shao-hua Wang and Lu Wang contributed equally to this article and are equal first authors.
Funding
This study was partially supported by the National Nature Science Foundation of China (grant no. 30870870, Shao-hua Wang), (grant no. 81070638, Shao-hua Wang) and (grant no. 81070916, Yi-jing Guo).
Conflicts of interest
The authors declare that they have no conflicts of interest.