
Abstract
A study on the prevalence of coronary heart disease (CHD) and its risk factors in Ceningan Island was conducted. The prevalence of CHD was 11.5%. Older age (odds ratio, OR, 27.0), underweight (OR, 3.6), systolic hypertension (OR, 4.6), high total cholesterol (OR, 5.9), and high low-density lipoprotein cholesterol (OR, 3.1) were risk factors for a history of myocardial infarction (MI). By logistic regression analysis, only age (B=3.937) and underweight (B=1.275) consistently appeared to be risk factors for MI. The prevalence of CHD in the population was comparatively high.
Keywords
Introduction
Cardiovascular disease (CVD) remains one of the most important causes of death in the world. Davies et al. reported that from 1996 to 2005 there was a decreasing incidence of coronary heart disease (CHD), but the prevalence increased by 1.3% in men and 1.7% in women. The results might be due to improvement in survival among people with CHD. 1 However, a report from Japan (1964–2003) showed a significant increase in the incidence of CHD in Asia. 2
The objectives of the study were to characterise the prevalence of CHD and its risk factors in a remote, island population of Ceningan.
Methods
A cross-sectional field study was conducted on the population of Ceningan Island, Bali, Indonesia. From a total population of the island of 888, 305 were recruited by simple random sampling (mean age 43 [14–100] years; male/female, 148/157). Diagnosis of heart disease was based on electrocardiography (ECG) examination. 3 Classification of nutrition states and obesity were defined by WHO criteria for the Asia Pacific population (2000). 4 Diagnosis of impaired fasting glycaemia and diabetes mellitus was established using the ADA (2009) criteria. 5 Diagnosis of metabolic syndrome was defined by the criteria of A Joint Interim Statement of the IDF TaskForce on Epidemiology and Prevention; NIH; AHA; WHF;IAS; and IASO (2009). 6
Results
The prevalence of CHD was 11.5% (myocardial ischaemia 3.6% and myocardial infarction (MI) 7.9%). Subjects with CHD had a significantly lower body weight than those without CHD (54.6 kg in subjects without CHD, 45.2 kg in subjects with myocardial ischemia, and 48.3 kg in subjects with MI). By excluding subjects with myocardial ischemia, the following variables appeared to be significant risk factors for history of MI: older age (odds ratio (OR) 27; 95% confidence interval (CI) 6.2–117.9; p<0.001), underweight (OR 3.6; 95% CI 1.5–8.7; p=0.003), systolic hypertension (OR 4.7; 95% CI 1.9–11.6; p<0.001), high total cholesterol (OR 5.9; 95% CI 2.4–14.1; p<0.001) and low-density lipoprotein (LDL) cholesterol (OR 3.1; 95% CI 1.3–7.9; p=0.01) (Table 1). With multivariate logistic regression analysis by entering all risk factors as independent variables, only older age (B=3.937; Exp[B]=51.266; 95% CI=6.615–397.306; p<0.001) and underweight (B=1.275; Exp[B]=3.580; 95% CI=1.159–11.060; p<0.027) consistently contributed to having a history of MI.
Prevalence risk (odds ratio) of some risk factors for history of myocardial infarction event
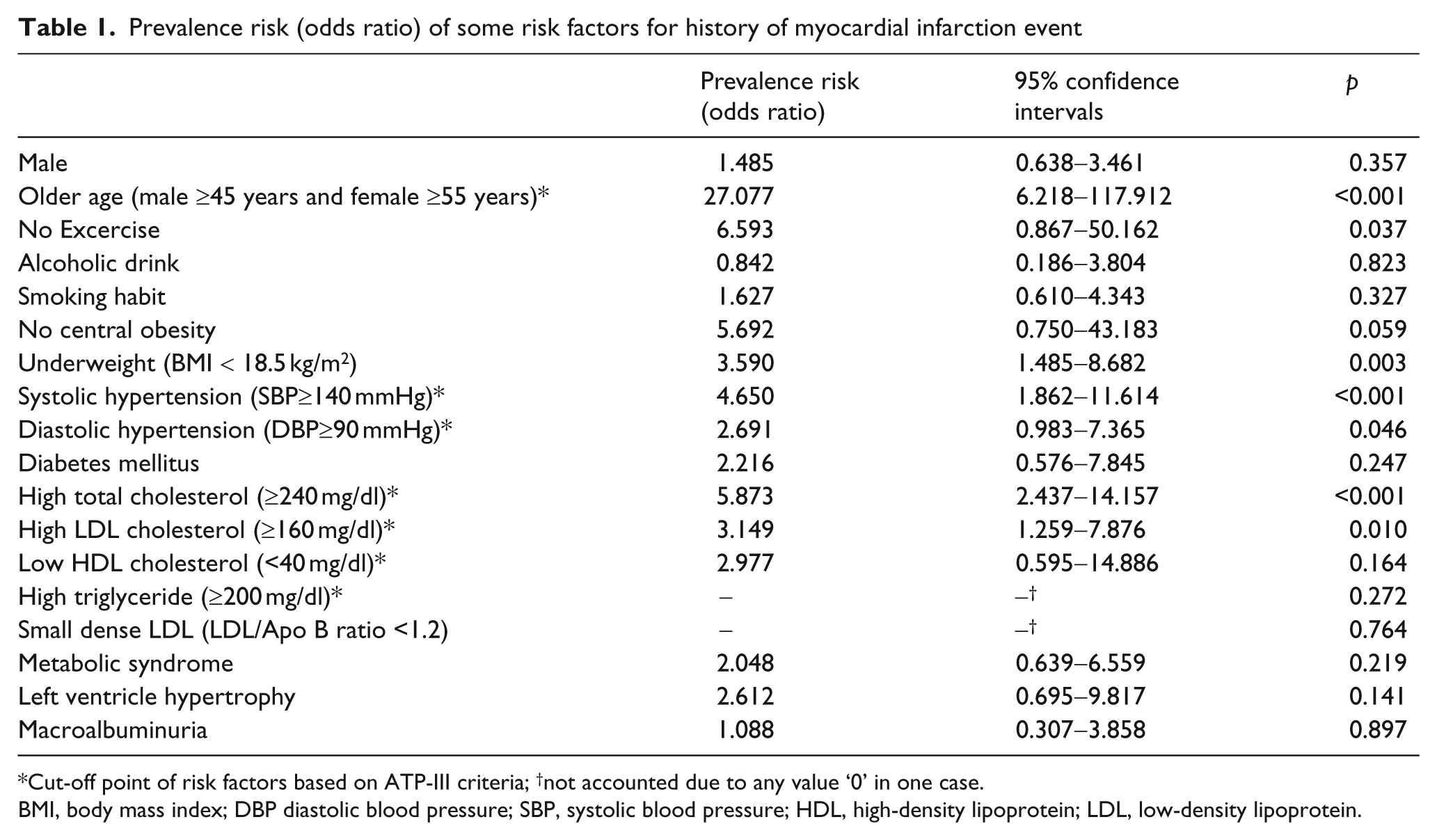
Cut-off point of risk factors based on ATP-III criteria; †not accounted due to any value ‘0’ in one case.
BMI, body mass index; DBP diastolic blood pressure; SBP, systolic blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Discussion
In our study, older age and underweight were important risk factors for a CHD event. Our tentative hypothesis is that atherosclerosis proceeds hand-in-hand with aging, independent of the individual’s general nutrition status. A study by Suastika et al. revealed that the prevalence of MetS and central obesity increased with age, peaking at 50–59 years and decreasing in the older age group. 7 This finding might add fuel to the prevailing controversy about the relationship between age, underweight, and CHD. A study of coronary artery disease (CAD) after prenatal exposure to the Dutch famine revealed an earlier onset of CAD among individuals conceived during the famine, suggesting that maternal nutrition in early gestation may play a role in the onset of CAD. 8 Huxley et al. in their systematic review revealed that a 1 kg higher birthweight was associated with a 10–20% lower risk of subsequent ischaemic heart disease. 9
Important questions related to this study that remain unanswered include elucidation of factors driving the relationship between underweight and CHD in this population, and effects of increasing age on these processes. Weaknesses of the study include the possibility that bias might be introduced in a cross-sectional study, and that the diagnosis of CHD was confirmed only by ECG.
Footnotes
This study was funded by the Udayana University Faculty of Medicine, Denpasar, Bali, Indonesia; Indonesian Society of Endocrinology, Jakarta, Indonesia; Kobe Women’s University, Japan; and partly supported by a Grant-in-Aid for Scientific Research (B): Overseases [grant nos 12576021 and 20406018] from the Japan Society for the Promotion of Science, Japan.
The authors declare no conflict of interest relevant to this article.