
Abstract
Introduction
The cardiovascular morbidity of patients with diabetes confers increased risk of surgical morbidity and mortality than non-diabetic patients. 1 Anaesthetics may alter the rate and extent of ventricular filling and often modify and destabilise cardiac haemodynamics during surgery in euglycaemic patients, and in patients with autonomic dysfunction. 2 Thus, cardiovascular (CV) responses to induction of anaesthesia in diabetic patients can be less predictable, making these patients more susceptible to CV complications during surgery. The most appropriate agent for induction of anaesthesia in diabetic patients, however, has yet to be determined.
Previous studies from our laboratory have shown that 1 month after diabetes induction, CV function in streptozotocin (STZ)-diabetic rats, a well known animal model of hypoinsulinaemic diabetes, deteriorates significantly compared to non-diabetic rats.3,4 The cardiomyopathy present in STZ-diabetic rats is similar to that observed in diabetic patients, making these animals a model for studying CV responses to induction of anaesthesia in diabetes.
The present study compares the effects of ketamine, etomidate and propofol on the CV profile of STZ-diabetic rats.
Materials and methods
Experimental animal model
Sixty Sprague–Dawley rats (Hilltop, Scottdale, PA, USA), at approximately 5 weeks of age were used. To induce diabetes, rats were injected intraperitoneally (IP) with streptozotocin (STZ, 65 mg/kg). The rats were used at 4 weeks following diabetes induction and did not receive insulin supplementation. All experiments were approved by the Institutional Animal Care and Use Committee, and adhered to the Guide and Care for the Use of Laboratory Animals published by the US National Institutes of Health. Ketamine (100 mg/kg), etomidate (20 mg/kg) and propofol (50 mg/kg) were administrated IP. These doses were the minimum required for each specific anaesthetic to induce anaesthesia based upon the ranges used in previous studies in which these agents were administered IP.5–7
Evaluation of cardiovascular parameters
After anaesthetic administration, the rats received serial transthoracic echocardiographic evaluation using a digital portable ultrasound system (Model 180P; Sonosite Inc., Bothell, WA, USA) equipped with a pulsed-wave Doppler and a transducer (bandwidth 7.5–9.0 MHz) as previously. 4 SBP was determined by sphygmomanometry. 3 Data were analysed using LabView software (National Instruments Co., Austin, TX, USA). The mean value of five measurements, separated by 3-min intervals, was reported for each animal.
Statistical analysis
Results are presented as the mean ± SEM. Statistical comparisons between groups were performed with analysis of variance (ANOVA; GraphPad-Prism 5.0, San Diego, CA, USA). The Student–Newman–Keuls test was used for post hoc analyses. Values were considered statistically significant at p < 0.05.
Results
The blood glucose concentration in diabetic rats was maintained at >400 mg/dl throughout the study period. In non-diabetic rats, by contrast, glucose concentrations remained within the normal range. Body mass increased in the non-diabetic rats (from 219 ± 12 g to 402 ± 11 g, N = 10), but did not increase significantly in the diabetic group (from 209 ± 11 g to 238 ± 12 g, N = 10).
Cardiovascular parameters are shown in Table 1. In non-diabetic rats, SBP was significantly higher in the group treated with ketamine than the groups treated with etomidate and propofol. In diabetic rats, by contrast, SBP was higher in the propofol and etomidate groups than in the ketamine group.
Effects of ketamine, etomidate, and propofol on systolic blood pressure and echocardiographic parameters in type 1 diabetic and non-diabetic rats
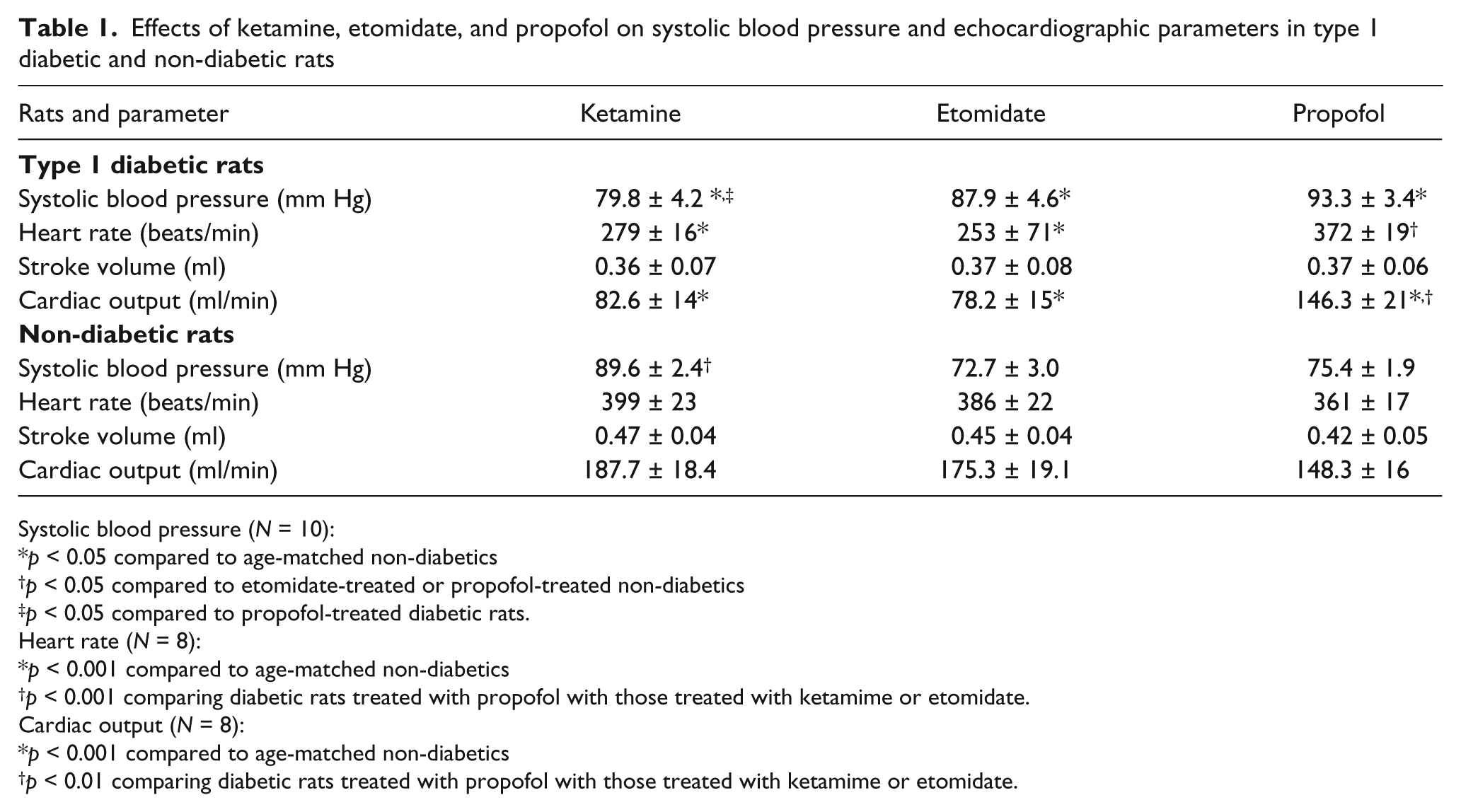
Systolic blood pressure (N = 10):
p < 0.05 compared to age-matched non-diabetics
p < 0.05 compared to etomidate-treated or propofol-treated non-diabetics
p < 0.05 compared to propofol-treated diabetic rats.
Heart rate (N = 8):
p < 0.001 compared to age-matched non-diabetics
p < 0.001 comparing diabetic rats treated with propofol with those treated with ketamime or etomidate.
Cardiac output (N = 8):
p < 0.001 compared to age-matched non-diabetics
p < 0.01 comparing diabetic rats treated with propofol with those treated with ketamime or etomidate.
In non-diabetic rats, cardiac output did not show a statistically significant difference between the ketamine-, etomidate- and propofol-treated groups. In diabetic rats, by contrast, cardiac output was significantly higher with propofol treatment than with etomidate or ketamine. The changes in heart rate were comparable to changes in cardiac output. In non-diabetic rats, no differences in heart rate were observed after anaesthetic treatments. In diabetic rats, however, heart rate was significantly higher with propofol than with etomidate or ketamine. None of the tested anaesthetics induced changes in stroke volume.
Discussion
Our results demonstrate that ketamine, etomidate and propofol produce different CV responses in STZ-diabetic rats than in non-diabetic rats. Comparison of these effects is difficult to interpret because the haemodynamic baseline characteristics of the two groups are different. 4 Thus, this paper compares the haemodynamic effects of the three anaesthetics within each group, a comparison that is designed to indicate a preferred induction anaesthetic for diabetes patients.
The observed increase in SBP among non-diabetic rats treated with ketamine, compared to those treated with etomidate or propofol, was expected due to its known sympato-excitatory effects. 8 Unexpectedly, however, a different pattern of CV responses is found in diabetic rats, where the cardiac output, heart rate and SBP values are lower with ketamine and etomidate than with propofol. The reduced cardiac output may be attributed primarily to a reduction in heart rate induced by these drugs, because no alterations in stroke volume occurred with either anaesthetic. Similarly, a decrease in cardiac output, secondary to a reduction in heart rate, has been observed in horses treated with a combination of ketamine, medetomidine and propofol. 9
Diabetes is known to alter neurotransmission by reducing presynaptic norepinephrine release, and by facilitating the development of autonomic dysfunction. 10 Thus, the reduced values for cardiac output, heart rate and SBP observed in diabetic rats treated with ketamine might result from a combination of two factors: the depletion of catecholamine stores and the autonomic dysfunction present in diabetes. This combination could impair baroreflex sensitivity and CV regulation. Our findings with ketamine in STZ-diabetic rats agree with other studies which report that when the sympathetic nervous system is impaired; ketamine produces myocardial depression both in vivo 11 and in vitro. 12
Contrary to expectations, propofol decreased cardiac output, heart rate, and SBP to a lesser degree than ketamine or etomidate. Propofol is known to produce vasodilation by increasing nitric oxide (NO)-mediated relaxation secondary to eNOS activation. 13 In diabetic rats, however, NO-mediated relaxation is impaired, and oxidative stress is increased. 4 Thus, the relatively high SBP observed in diabetic rats treated with propofol may be a consequence of increased oxidative stress, which in turn may decrease NO availability, and thereby impair the relaxing effect of propofol. Although the increases in SBP and cardiac output may have a positive impact on diabetic patients undergoing surgical procedures because tissue perfusion will improve, the propofol-induced increase in heart rate may have a deleterious effect on a compromised heart, and even induce cardiac arrhythmias. In line with this possibility, Wickley and collegues 14 suggest that propofol should be administered cautiously to patients with limited inotropic reserve and/or diastolic dysfunction because it causes a decrease in myofilament Ca2+ sensitivity, which may worsen cardiovascular status.
The unexpected CV responses of diabetic rats to induction anaesthetics may result from a combination of autonomic dysfunction, hyperglycaemia and oxidative stress. Two limitations of this study should be noted. Firstly, the anaesthetics were administered by a single intraperitoneal dose, compared with intravenous administration to patients. Secondly, the STZ-diabetic rat is severely insulinopenic, as in type 1 (but not type 2) diabetes.
In conclusion, CV responses of STZ-diabetic rats to anaesthetic induction agents differ from non-diabetic rats. The mechanisms remain to be understood, but the observations may be relevant to induction of anaesthesia in diabetic patients.
Footnotes
This work was supported by RCMI Program Grant G12RR03051 of the NIH and the Department of Anesthesiology of the University of Puerto Rico-School of Medicine.
The authors declare that they have no conflicts of interest.