
Abstract
This paper uses a newly created database of all women who gained a qualification registrable with the General Medical Council between 1877 and 1914 to answer the following questions. Where and when were they born, where were their parents born and where did they train? The paper shows that women doctors born in Scotland or of Scotland-born parentage formed a much higher proportion of the population of that country than those born in England and Wales, or in Ireland. In addition, Scotland trained a disproportionately higher share of those trained in the United Kingdom. Odds ratios are used to establish the significance of this picture. Some provisional ideas are advanced towards an explanation of these findings.
Keywords
Introduction
The literature on women doctors in the 19th and early 20th centuries has focused on sub-populations, sometimes too small for statistical analysis. Nothing equivalent for women matches the detailed and illuminating analysis of men who matriculated in the medical faculties of Glasgow and Edinburgh Universities, c. 1871.1,2 The primary example of a focus on small populations is the writing about the efforts of women to gain a medical qualification in Edinburgh between 1869 and 1873.3,4 In the public imagination, seven women – the septem contra Edinam, in the words of their leader, Sophia Jex-Blake (1840–1912) – attended medical classes in Edinburgh in this period.3,5 The University class records, however, list 40 women who did so. 6 While 29 of these women did not go onto a medical career, we know a great deal about the 10 who finally gained a medical qualification, along with Isabel Thorne, née Pryer (1835–1910), who became Honorary Secretary of the London School of Medicine for Women (LSMW).1,7 Similarly, the history of the other members of the early cohorts of women who qualified from the LSMW has received attention.7 –9 What of the women who trained and qualified elsewhere?
Bonner provides an excellent account of the context of efforts elsewhere in Europe and in North America by women attempting to gain medical qualifications. 10 In a pathbreaking work, Alexander studied the 62 women who gained Glasgow medical degrees in the 6 years, 1898–1900 and 1908–1910. 11 Kelly’s study of Irish doctors analyses some data on 759 women who matriculated in medicine in Irish medical institutions, 1885–1922. Her listing of those who qualified up to 1914 includes 65 women. 12 Good accounts also exist of how the First World War transformed the short-term opportunities for hospital work of many women doctors, especially those who worked in the Scottish Women’s Hospitals for Foreign Service and for the Royal Army Medical Corps in Malta and Salonika.13 –18 Their contributions to the women’s suffrage movements have also been addressed.19,20
These sources nevertheless provide only partial and incomplete information on the total number of women who became doctors in the United Kingdom (UK) before the end of 1914, and their social origins, training patterns and career paths. This paper, by contrast, uses a database of all women who gained UK qualifications registrable with the General Council of Medical Education and Registration, later the General Medical Council (GMC), between 1877 and 1914, to analyse, inter alia, patterns of social and geographical origins and the medical institutions attended.
Context
After 1858, registration with the GMC was essential to be employed in official positions or have some protection in law when practising medicine in the UK and its colonies. 21 Women were unable to register until a recognised college or university admitted them to sit for qualifying examinations. An Enabling Act in 1876 allowed, but did not require, recognised institutions to admit women. The King and Queen’s College of Physicians in Ireland (later the Royal College of Physicians of Ireland) opened its licentiate examinations to women in 1877. This event provides the start date for the study discussed in this paper. Other UK colleges and universities followed suit over the following 30 years or so.
Educational institutions for women in medical subjects started well before women could gain a recognised medical qualification. In London, the Ladies’ Medical College, established in 1864, lasted until 1873, and is noteworthy for having provided Isabel Thorne and Matilda Chaplin (1846–1883) with early training: both took medical classes in Edinburgh in 1869–1873.7,9 The training schools and colleges established across the UK after the Enabling Act were much better funded and offered a fuller range of courses. Table 1 shows the number of women who finished their training at each of them. It demonstrates that the LSMW was by far the largest single source to complete the training for women medical students in this period. The LSMW opened in 1874, and by 1877, the Royal Free Hospital had allowed its students to complete their clinical studies on its wards. All their classes were single sex.
Medical colleges and university medical courses in the UK, by date of opening to women, first women students matriculated, year of first woman’s graduation and numbers of women who qualified up to 1914.
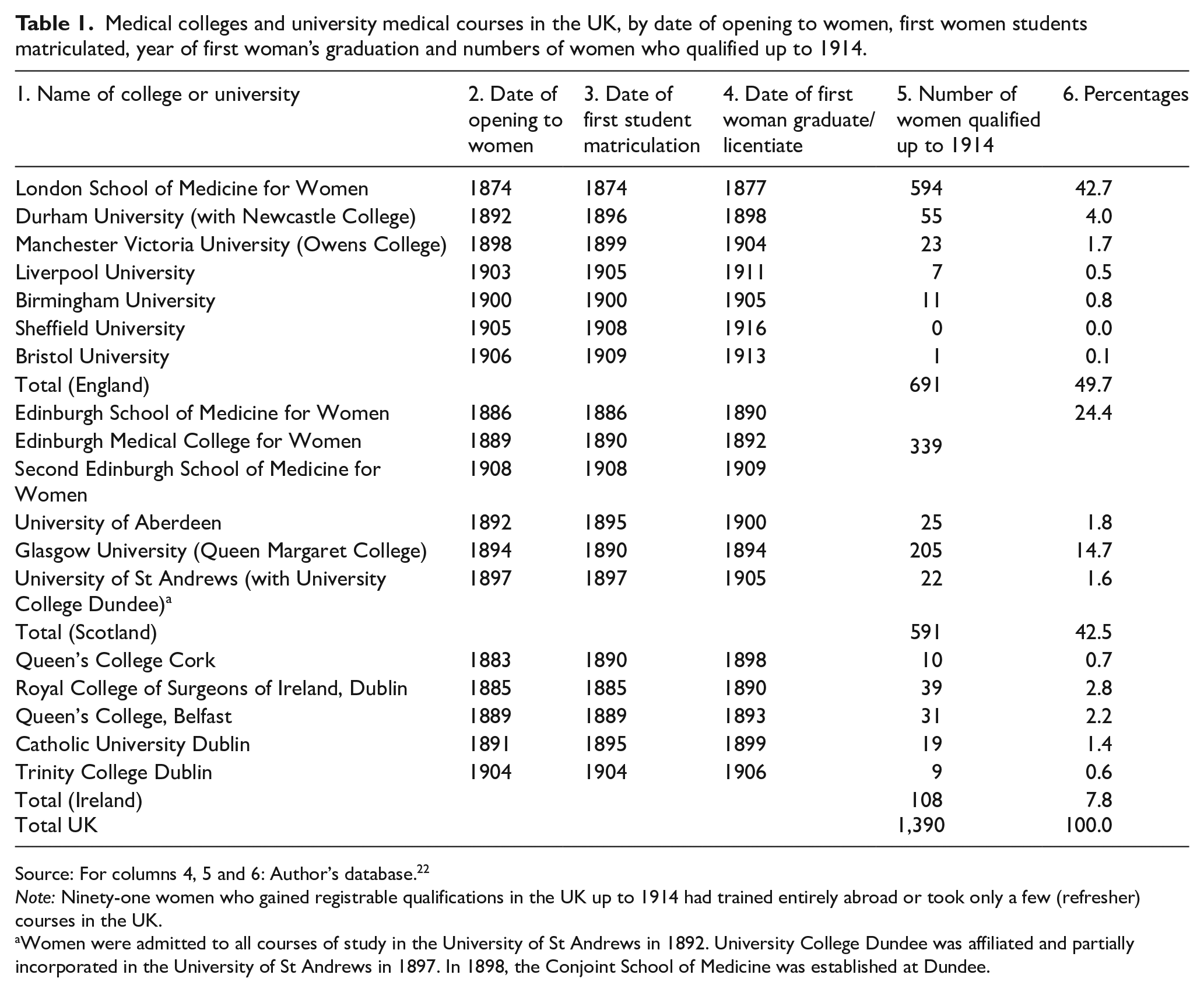
Source: For columns 4, 5 and 6: Author’s database. 22
Note: Ninety-one women who gained registrable qualifications in the UK up to 1914 had trained entirely abroad or took only a few (refresher) courses in the UK.
Women were admitted to all courses of study in the University of St Andrews in 1892. University College Dundee was affiliated and partially incorporated in the University of St Andrews in 1897. In 1898, the Conjoint School of Medicine was established at Dundee.
The monopolistic position of LSMW was challenged when women were admitted to university, college or extra-mural training programmes elsewhere in the UK, where women were sometimes trained alongside men. The second UK city to host a college for women’s medical education was Edinburgh, where the Edinburgh School of Medicine for Women (ESMW) was established by Sophia Jex-Blake in 1886. A rival institution, the Edinburgh Medical College for Women (EMCW), was established in 1889.23,24 The two institutions operated in competition until 1898, when the ESMW closed. The EMCW continued until 1908, when the University of Edinburgh abruptly sold the building that had housed the women medical students. A group of approved teachers from Edinburgh’s Extra-Mural Medical School quickly established a new Edinburgh School of Medicine for Women (ESMW2), which operated until 1916, when women were finally allowed to take all their classes alongside men.
Some of the classes offered by the EMCW and ESMW2 were mixed and others not, varying from year to year depending on approval from the University of Edinburgh’s Medical Faculty. In the University of Glasgow, at least some separate classes for women were held at Queen Margaret College from 1890 until 1911, when women were fully admitted into university classes. 25 By 1900, mixed instruction in Scotland was also available in the University of Aberdeen, and, later, for some classes at the University of St Andrews and University College Dundee. 26
Estimates of the number of women who gained these qualifications have used various sources with different results. The pioneering work of Harrison 27 and of Elston 28 used England and Wales census data and lists of women doctors and their residence and employment printed up to 1911 in the Englishwomen’s Yearbook. The Yearbook reported on the progress in women’s position not only in the UK, but also in continental Europe, the British Empire and North America. The Yearbook’s list of women doctors was derived solely from the Medical Directories. On the basis of the sources he consulted, Harrison concluded that the few women doctors he found could not have made any substantial contribution to women’s health overall in the UK, because they were concentrated in London and a few other towns. 27 Scott’s BMJ article using GMC records relating to women doctors unfortunately gives no sources for its estimates of numbers up to 1921, nor clarity over whether they referred to England and Wales, Great Britain or the UK, for example. 21 Estimates for the number of women doctors in 1911 range from 477 (Digby) and 495 (Harrison, both based on the census) to 600 or 610 (Scott and Elston, sources unclear) and 930 (Elston, based on Medical Directory entries).21,26 –28
All these studies note that each of the sources analysed has limitations. The 1911 census missed an unknown number of suffragette doctors who refused to complete a return. Definitions of medical practitioners varied by census year, for example, and included retired doctors until 1931. 28 Not all women who qualified at this period joined the Medical Register. Some, especially those who worked outwith the UK, in the colonies or in continental Europe or the USA, for example, either never registered or allowed their registration to lapse while abroad, as did some of the women who were not practising medicine or had retired. Entries in the Medical Directory were optional. In any event, taking snapshots of one year at a time can provide a misleading picture, especially when disparate sources are used to estimate trends. 2
To be able to analyse trends through time, and to compare those trained in different parts of the UK or the impacts of birthplace and heritage, requires a different approach, which is the one adopted here. To contribute to the historiography of women’s medical training, a searchable database was developed and is archived and available for public access. 22 It draws not just on census returns, the Medical Directory and Medical Register, but also on a wide range of other sources. These include, for example, parish registers; records of birth, marriage and death; passenger listings for those who travelled; newspaper articles; the GMCs Register of Medical Students; and the matriculation and examination records of some universities and qualifying bodies. One stimulus for creating this database was a desire to identify the women who qualified after training in Edinburgh, and the project grew to cover the rest of the UK to contextualise these women and to discover whether they varied in any significant ways from those trained elsewhere.
Method of database creation
The database includes 1,481 women doctors who gained a UK registrable qualification between 1877 and the end of 1914. The database consists of 48 key variables, including women’s birth and death years, their places of birth and death, training institution(s) attended, qualifications gained, basic information on their social origins and careers, marriage (if any), war service, missionary employment and connections to India and China. Elizabeth Blackwell (1821–1910) and Elizabeth Garrett, later Anderson (1836–1917) who joined the Register before 1870, were excluded. The end date avoids the changes wrought by the First World War, when a rapid expansion in women medical students took place: London medical colleges temporarily admitted women, to compensate for the great reduction in numbers of male applicants.8,29
Digitisation of some key sources has made creating such a database much easier than was possible in the 1980s. Care must still be taken, if only because digitisation of handwritten texts is an imprecise art. Even skilled transcribers must sometimes guess meanings from sources, especially when relating to unfamiliar topics. 30 In addition, establishing whether women married, and if so, whether they changed their surnames for professional purposes, is challenging. For women born, married or died outwith the UK, basic data, such as the occupations of fathers, are often unavailable.
The main sources consulted are as follows:
Names of women who attended the LSMW up to 1914. 31
Names of women who took the triple qualification (TQ), that is, the Licences of the Royal College of Physicians of Edinburgh (LRCPE), the Royal College of Surgeons of Edinburgh (LRCSE) and the Faculty of Physicians and Surgeons of Glasgow (LFPSG) (later the Royal College of Physicians and Surgeons of Glasgow, RCPSG). 32
The digitised versions of the Medical Students Registers, 1882 and 1889–1911, available on Ancestry.co.uk, and the hard copies for 1877–1888 held at the RCPSG. 33
Supplementary information comes from the Calendars of the University of Edinburgh 34 ; a list of alumnae of the Edinburgh College of Medicine for Women, up to 1908, held in the Centre for Research Collections, University of Edinburgh 35 ; Kelly’s list of women who qualified in Ireland 12 ; Alexander’s discussion of Glasgow graduates 11 ; and lists of alumnae provided by Glasgow University. 36 The Journal of the Association of Medical Women in India lists medical women in India, from which those who qualified in the UK were extracted. The website of the Friends of Millbank lists 84 women who served in the Maltese Islands and Salonika between 1916–1919. 14 Married women were matched to their birth surnames, using census and other sources digitised by Ancestry.co.uk from regional records offices and the national archives, the British Newspaper Archive, family history data provided by Families in British India, etc. All data have been cross-checked wherever possible, and the assistance of two professional genealogists was engaged for complicated or difficult cases. For example, wherever possible, dates of birth are taken from birth and baptismal records (where they also give a date of birth). If these records are unavailable, the census nearest the probable birth year is used. The 1939 England and Wales Register gives dates of birth and occupation and serves in many cases as a useful source for the triangulation of such data.
These data have been entered into family trees where possible. These trees include links to source information for the focus person and her immediate family: parents, siblings, partners and children. For example, the family tree for Elsie Rosa Cresswell Taylor (1873–1968) includes links to scans of her entries in enumerators’ forms for the 1881, 1891, 1901 and 1921 censuses, as well as to the 1939 England and Wales Register. It also includes two links to her baptismal record; one to a newspaper report of her marriage to Ernest Eldrid (1876–1961), employed in the Imperial Bank of Persia, in 1905, in Yazd, Iran, where she was a medical missionary – the reason for her omission from the 1911 census. Also included are scans of the pages where she is mentioned in the Medical Students’ Register for 1893, for two entries in the Medical Register (which confirm the date on which she registered, on the basis of her Triple Qualification) and one in the Medical Directory, and finally, her entry in the England and Wales National Probate Calendar (Index of Wills and Administrations). The material on Elsie Taylor is relatively detailed and reliable, whereas for some other women only one or two items are available. For example, Vera Nicolaevna Bolotine (1889-?), born in Samara, Russia, who studied for 3 years at St Andrews and completed her training in Edinburgh in 1913, disappears from available records after the outbreak of the First World War. In principle, it is possible to use these data to investigate whether, for example, position in sibling groups, the presence of siblings who also studied medicine, or the death of a parent, might have had an impact on decisions or the financial ability to study medicine.
The database excludes trained women who did not take a registrable qualification yet practised medicine for a few years, such as Annie Bonus, later Kingsford (1846–1888) and Emily Bovell, later Sturge (1841–1885), who gained MD degrees in Paris in 1877 and 1880, respectively, and Helen Johnston, described in the LSMW records as ‘Unqualified but in practice’. Elizabeth Mary Clark, (the wife of a missionary, Robert Clark) practised in India on returning there, without gaining a registrable qualification. 6 Women who registered in the Colonial or Foreign Lists through qualifications solely gained outwith the UK, usually British settler colonies and South Asia, are not included in the database, though they were able to work in the UK or for British employers during the First World War.
The database allows a new way of estimating the number of women doctors who had qualified in the UK by the time of the 1911 census. At that date, 1,116 UK-qualified women doctors were alive, but not all were in the UK, nor necessarily in paid or self-employment. On the other side of the equation, in 1911, some women who registered with the GMC with foreign qualifications were working in the UK.
The rest of this paper presents some initial key findings from this database, starting with the social origins of the women (birthplace and parentage), where they trained and which qualifications they gained. Because many were mobile, taking their training from more than one medical school, for this paper they are counted as having qualified from the final medical college or school they attended.
Social origins
Birthplaces
Table 2 shows the birthplaces of the women who qualified. Amongst those born in the UK, the prominence of those born in Scotland is striking. Because the number of women born in Wales is small (29) and no training institution in Wales could provide a full medical training at this period, data on Wales have been included with those for England. The odds ratios for Scotland and Ireland, relative to England and Wales, compare the numbers of women doctors with number of women born in these countries in the same years. Women doctors were about four times more likely to have been born in Scotland than in England and Wales, with the odds ratio 4.02 (95% CI 3.54–4.57). No statistically significant relationship emerges for Ireland-born women, compared to those born in England and Wales, odds ratio 1.10 (95% CI 0.92–1.08).
Birthplaces of women doctors qualified in the UK, 1877–1914, by year of first UK qualification.
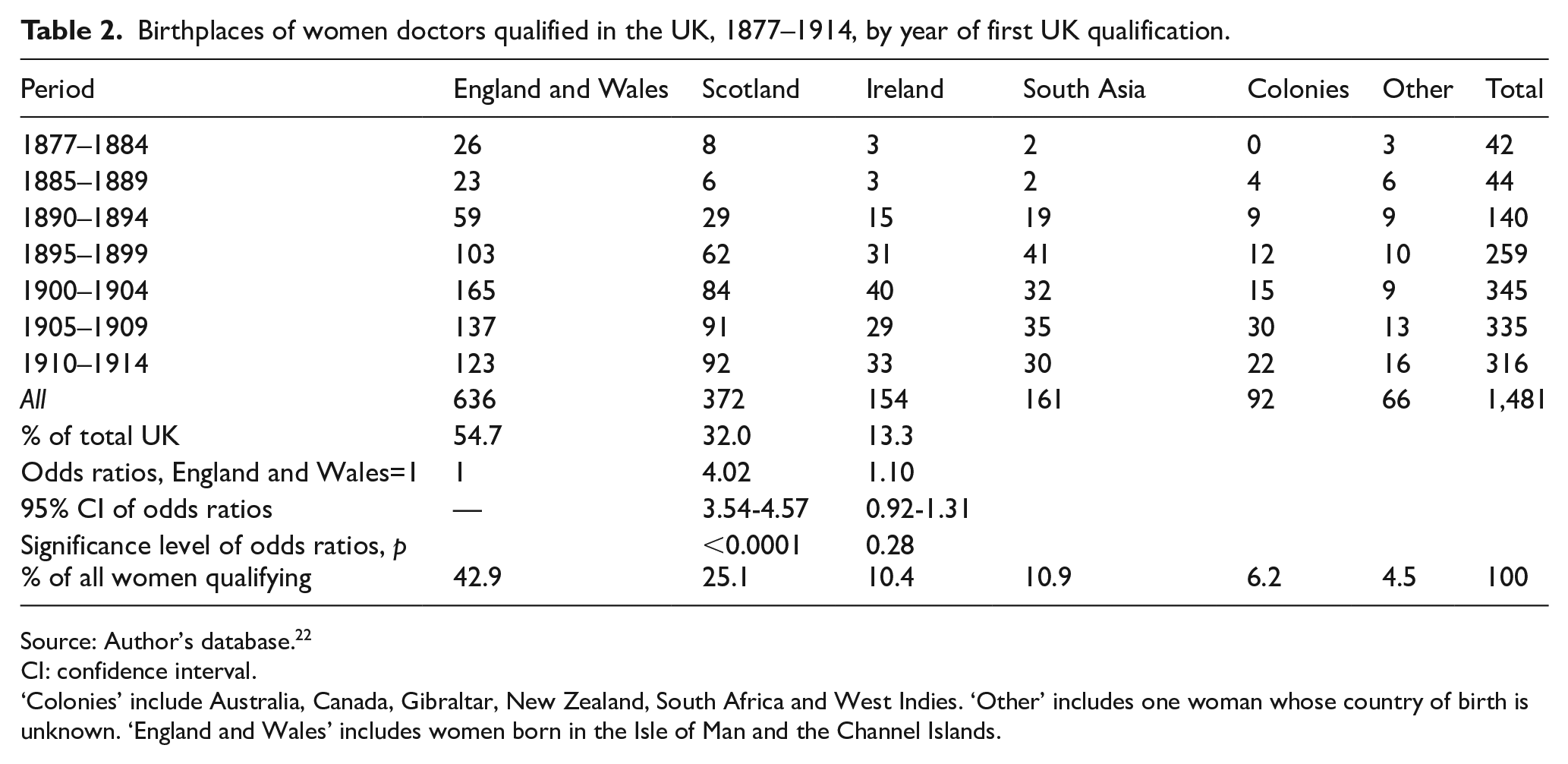
Source: Author’s database. 22
CI: confidence interval.
‘Colonies’ include Australia, Canada, Gibraltar, New Zealand, South Africa and West Indies. ‘Other’ includes one woman whose country of birth is unknown. ‘England and Wales’ includes women born in the Isle of Man and the Channel Islands.
Of the women in the database, 319 (21.5%) were born outside the UK. Their origins reflect the intrinsically imperial position of the UK at the time. One hundred sixty-one women (10.9% of the total) were born in South Asia. Most of these women had European names: at least 100 had at least one parent themselves born in South Asia. Ninety-two women (6.2% of the total) were born in the British settler colonies – Australia, New Zealand, Canada and South Africa. The remaining 66 women (4.5% of the total) were born in continental Europe including Russia and Turkey (37 women), the USA (10 women), Asia and the Pacific (9 women), Madagascar (5 women), British Guiana (2 women) and one each born in Syria, Aden and Argentina. Of these 66 women, 31 had at least one parent born in the UK.
Parentage
Birthplace is a blunt indicator of ethnicity or identity, particularly among a mobile population when many British-born adults were serving as missionaries, colonial administrators and military personnel overseas or had themselves migrated, expecting to live in a new country for the rest of their days yet sometimes returning to the UK. One example is Laura Elizabeth Forster (1857–1917), who was born in Australia; her father was born in Madras, India, of Irish-born parents, who had married in Australia. Laura’s mother was born in Australia, but Laura’s maternal grandfather was born in Ireland and her maternal grandmother in England.
The birthplaces of parents provide an additional, admittedly not entirely adequate, indicator of social identity, of how they might feel or see themselves in relation to others, or to have experienced aspects of upbringing with a strong national character – for example, having an attachment to Presbyterianism. The evidence from the database shows that women doctors were disproportionately likely to have Scotland-born parentage, even amongst those women born outwith Scotland. Table 3 shows that 369 of the 1,4812 women doctors had both parents born in Scotland compared to 542 with both born in England and Wales. A further 136 women had 1 parent born in Scotland, so that 678 (46%) had at least 1 parent born in Scotland. Using the relative average population sizes in 1871 as the base, women doctors were four to five times as likely to have both parents born in Scotland than to have both parents born in England, with the odds ratio 4.61 (95% CI 4.04–5.26). Again, no statistically significant relationship emerges in the case of parents born in Ireland, compared with those born in England and Wales, with an odds ratio of 1.03 (95% CI 0.86–1.24).
Birthplaces of parents of women who qualified in medicine in the UK, 1877–1914.
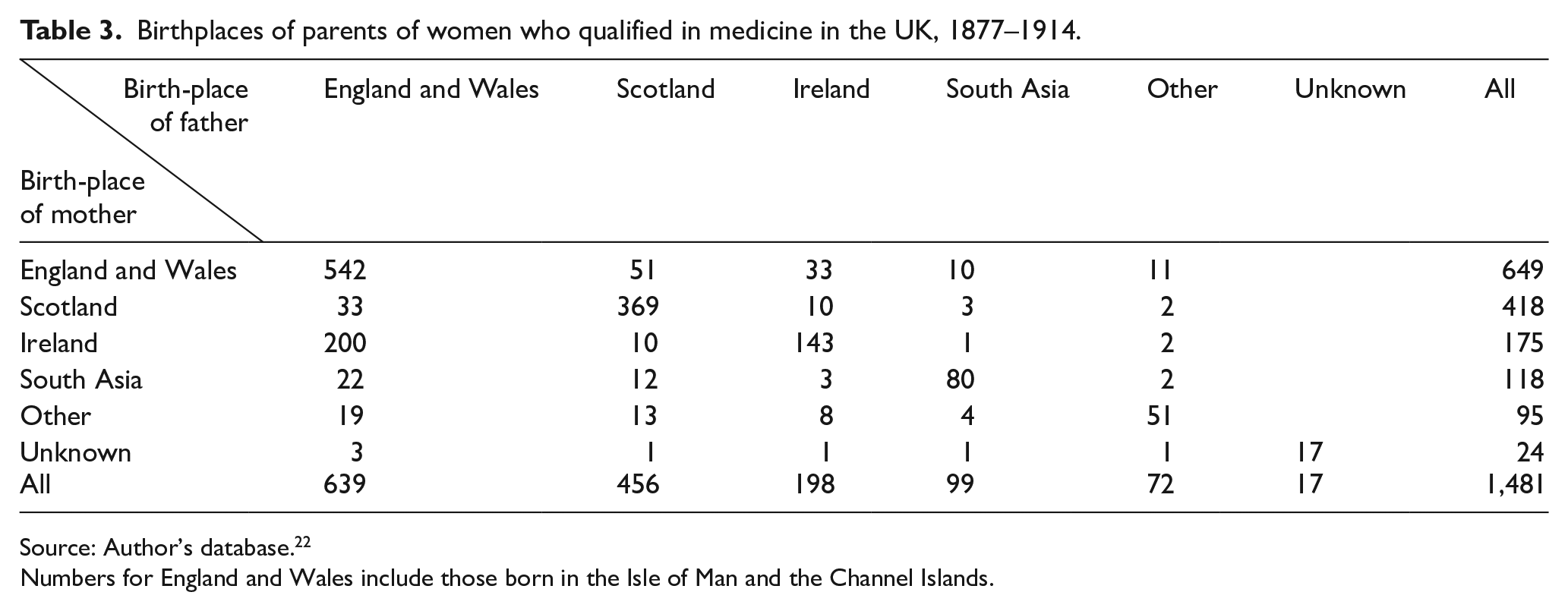
Source: Author’s database. 22
Numbers for England and Wales include those born in the Isle of Man and the Channel Islands.
Occupations of fathers
For social class, we have only the occupations of fathers to use as indicators. Married women in the middle and upper classes rarely had paid employment in the 19th century; indeed, their daughters who became women doctors formed one of the largest groups among the pathbreakers in this respect. More research is needed to discover whether mothers played as significant a role in encouraging (or discouraging) daughters from taking up medical training as did their fathers. The paternal backgrounds of 35 (2.5%) women are currently missing.
Economic, cultural and social capital, in Bourdieu’s terms, 37 were all important: men with higher education themselves are well-represented amongst the fathers. Information on the schooling of these women is limited. Universal primary education had begun in 1870, and girls’ secondary schools opened steadily in the following decades. In a few cases, we know that parents taught their daughters themselves or hired a tutor or a governess. One of these routes would have been almost a sine qua non for gaining sufficient education to be able to tackle the preliminary examinations for entry into a medical school.
Classifying the occupations of the fathers is not straightforward, since job titles were not standardised and some men reported more than one occupation. In the context of this paper, only a brief overview will be provided, using the categorisation for Victorian Scotland developed by Anderson. 38 The ‘old’ professions provided the largest group, 579 fathers, including 232 ministers of religion or missionaries, 133 doctors (including 2 medical missionaries), 89 lawyers (including solicitors and advocates), 41 teachers, 41 ‘gentlemen’ and 39 military officers. The ‘new’ professions contributed 144 fathers, of whom 54 were in government employment, 53 engineers, 20 accountants and 13 architects, scientists or surveyors, including 4 in journalism. From the 380 ‘commercial and industrial’ fathers, 123 were merchants, 101 manufacturers, 64 dealers, brokers or agents, 44 managers, 32 paramedical (including dentists and subordinate medical staff), 11 bankers, and 5 were ships’ captains. Two hundred fathers were in ‘intermediary’ positions, 146 shopkeepers (12 of whom were chemists), 54 clerks or minor officials. Ninety-nine fathers were reported as farmers (96) or in land-related activities. Forty-four fathers reported a named trade or skill in the skilled, semi-skilled or unskilled working class. The occupations of 35 fathers are not known. The most obvious differences from the analysis by Crowther and Dupree of male matriculates are that more women were daughters of ministers of religion (15.6% compared to 6.1%) and the ‘new’ professions (9.7% compared to 4%). Slightly fewer were the daughters of doctors (8.5% compared to 10.4%). 1
Very few scholarships were available to help see a woman through her medical training. A major exception to this generalisation is the full fee reimbursements provided by the Carnegie Trust for the Universities of Scotland between 1901 and 1914. A further paper will analyse paternal occupational data in more detail, when investigating whether this funding affected the social class distribution of women medical students in the UK. 39
Training and qualifications gained
Colleges for women
By the summer of 1914, 1,140 women had spent some time training at the LSMW, of whom 594 (40% of the total database) completed a registrable qualification while a student there. The remainder passed through its doors but completed their training elsewhere: for example, 32 women transferred to Durham/Newcastle between 1899 and 1914. Others withdrew, gave up study, were not entered for examinations, or already held a registrable qualification and came to take some additional courses or to prepare for an MD degree. The alumnae of the LSMW therefore dominate the overall population of women doctors, and they frequently appear in stories of those who breached some of the continuing professional barriers.
The Scottish medical schools were well placed to respond to the opportunity to train women because, by the middle of the 19th century, they had established themselves as leading suppliers of medical education in the UK and could accommodate the relatively small additional numbers of women students, though clinical opportunities could be in short supply. 40 For the whole database, Scottish medical schools trained 591 women (40%) but they did not begin to produce qualified doctors until 1890. Between 1890 and 1914, 622 England-trained women qualified. Using populations of women aged 15–34 in England, Scotland and Ireland in 1891, the odds ratio for women doctors qualifying from Scottish medical schools and colleges rather than from English ones from 1890 to 1914 was 6.95 (95% CI 6.21–7.78). The odds ratio for women doctors qualifying from Irish medical schools and colleges rather than from English ones was 1.03 (95 % CI 0.84–1.27).
The presence of medical colleges close to their homes was an important influence on women’s access to training, as can be seen from Table 4. Women born in Scotland were more likely to study in Scotland than those born in England or Ireland were to study in their home nations. Nevertheless, over one-third of women travelled long distances from their birthplaces. Despite doctors and medical institutions in Ireland possessing, ‘a positive attitude towards women in the medical profession’, 12 Ireland attracted relatively few women from elsewhere. Eleven women began their training in Cardiff or Aberystwyth and completed their studies elsewhere. Ninety women (6.1%) had most or all their training outside the UK, 54 (3.7%) of them in South Asia. Scotland and England were equally attractive to women born abroad, each taking about half of the 264 such women in the database who did most or all their medical training in the UK.
Country of main training institution attended by birthplace for women who qualified in medicine, 1877–1914.
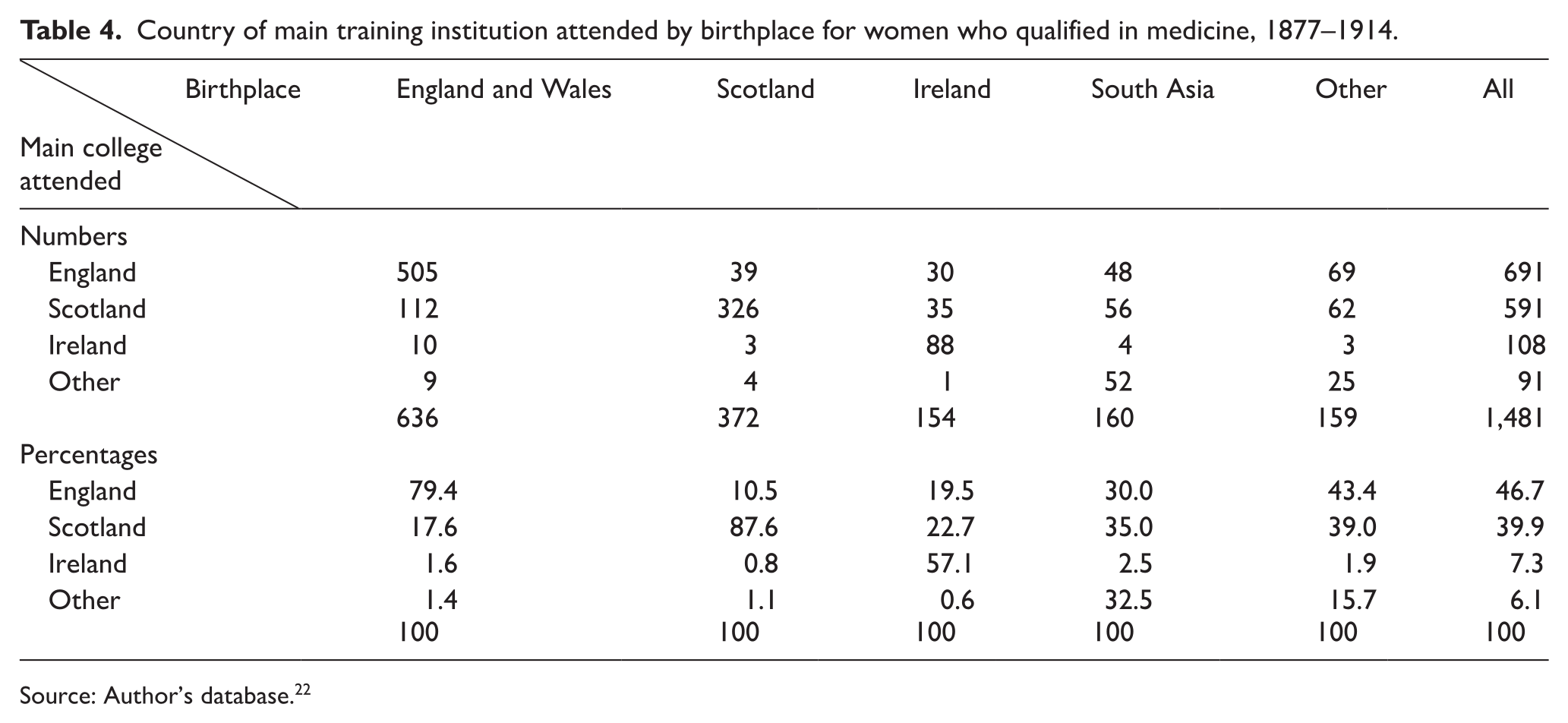
Source: Author’s database. 22
Qualifications taken
Table 5 shows the various qualifying examinations taken by women up to 1914. The University of London allowed women candidates to matriculate in 1882. The three Scottish medical colleges waited until the conclusion of a review of medical education before they established the TQ in 1884. In April 1886, they confirmed that ‘provided the curriculum and examination shall be of the same standard for both sexes’ they would open the TQ ‘to women equally with men’.41,42 The Worshipful Society of Apothecaries in London offered a Licence (LSA) to women from 1888.
Qualifying UK medical institutions by date of opening to women, date of first woman to qualify, and numbers qualified, 1877–1914.
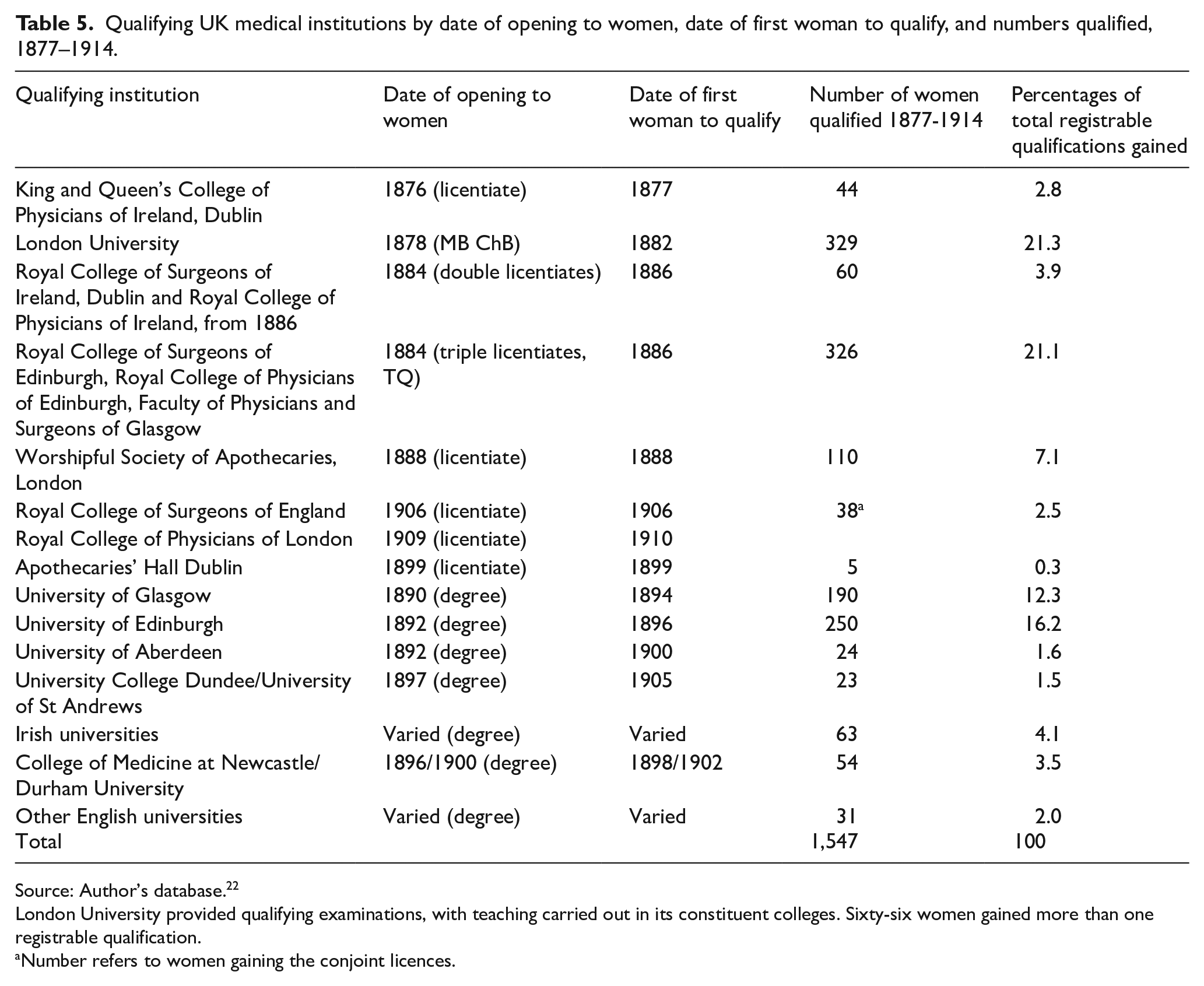
Source: Author’s database. 22
London University provided qualifying examinations, with teaching carried out in its constituent colleges. Sixty-six women gained more than one registrable qualification.
Number refers to women gaining the conjoint licences.
Scottish institutions initially prepared students mostly for the TQ, but as the university degrees were opened to women candidates, these were often the preferred options. Across the UK, university degree examinations were perceived to be more challenging, and some weaker students (and sometimes whole graduating classes) were entered into the TQ or the LSA as an insurance against failing in the other examinations they took. Other reasons could also be relevant, such as being able to qualify earlier. 26 The Royal Colleges in London had formed their own Conjoint Examining Board in 1884, but women could not attempt this until 1910. Some women doctors took a further qualification, at least 62 an MD from Brussels, for example. This was probably to enhance their employment prospects as well as to legitimise their using the title of doctor. Of all registrable qualifications gained before the end of 1914, 53% were from Scottish qualifying institutions.
Conclusion
This paper describes a new database that challenges the received picture of women’s medical education up to 1914. It is used here to analyse the nature and significance of birthplace and parentage in the early growth of the women’s medical profession in the UK. It demonstrates that women born in Scotland or with parents born in Scotland were remarkably over-represented in this cohort of qualified medical women. The paper also provides estimates for all the colleges and medical schools of the total number of women who qualified. It confirms the centrality of the LSMW as the largest single institution training women doctors. The LSMW also provided short-term support to women whose training was largely elsewhere, or who had graduated or qualified in other parts of the UK. The paper also shows, however, that in the final 25 years covered by this study, almost as many women qualified from Scottish medical schools (590) as from English ones (622). Overall, Scotland was a disproportionate source of recruits to medicine, of training opportunities and of examinations.
Only some general and somewhat speculative suggestions can be provided for why Scotland played such a major role. To some extent this could be path dependency: by the middle of the 19th century, Edinburgh and Glasgow, and to a lesser extent Aberdeen, had established high reputations for medical education. They had the infrastructure to teach large numbers of medical students. Further than this, the Scottish medical establishments were less hostile to women’s medical education than those in London. Access to hospitals for clinical training was arranged quite quickly in Scotland, and its Royal Colleges opened their licentiate examinations to women 24 years before those in London did. The London hospital medical schools were fiercely independent and competitive, and the rapidity with which they reverted to male-only admissions after the end of the First World War suggests that they were also more misogynistic than medical educators elsewhere in the UK. 8 It may also be the case that the dominance of the LSMW inhibited the growth of additional women’s medical training opportunities elsewhere in England. Further papers are planned to reflect on some of the issues raised here.
Footnotes
Acknowledgements
I am very grateful to Jacqueline Cahill at the RCSE archives for her assistance and to archivists in the Centre for Research Collections, University of Edinburgh and at the Royal College of Physicians and Surgeons of Glasgow; to Iain Macintyre and Juliet Gayton for timely and excellent advice; and to Caroline Gerard and Juliet Gayton for assistance with family histories. I have used digitised sources from Ancestry.co.uk, sourced from the National Archives and from the Welldome Collection, with permission.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author received no financial support for the research, authorship, and/or publication of this article, except for support from the Scottish Higher Education Digital Library Consortium to make it open access.