
Abstract
Introduction:
Delirium is a common, severe neuropsychiatric syndrome in hospitalised older adults. We evaluated use of validated delirium assessment tools, adherence to national guidelines and prevalence and management of delirium across Scotland, identifying barriers to effective care.
Methods:
Secondary analysis of national survey data, collected by participating clinicians on World Delirium Awareness Day (15 March 2023).
Results:
Among 120 responses (3,257 patients), the 4AT was the most frequently used assessment tool (75%), while 14% of units reported using clinical judgement alone. The delirium assessment rate was 74%, with a prevalence of 22% at 8 am. Management protocols varied, with frequent routine non-pharmacological interventions including pain management (88%), hydration (87%) and open family visiting (80%). Barriers to delirium care included insufficient staffing and training.
Conclusion:
While many hospital settings follow national delirium guidelines, some still rely on clinical judgement for assessment, with variability in management protocols and practices. We have highlighted key barriers to effective delirium care in Scotland.
Introduction
Delirium is an acute, severe neuropsychiatric syndrome precipitated by one or more medical conditions, interventions or medications. 1 It is associated with adverse outcomes, including higher mortality, transition to a nursing home, and a higher risk of future dementia.2 –4 Delirium is common in acutely hospitalised older adults, with occurrence rates of 23% in medical inpatients and 31% in intensive care units (ICU).5,6
Effective delirium management requires both that delirium is detected and that this is acted upon. Use of a validated tool for delirium assessment is better than clinical judgement alone. 7 Numerous tools have been developed for clinical practice with good sensitivity and specificity in research studies. 8 Several of these have been implemented at scale as part of routine care, with variation in tool completion and delirium detection rates. 9 However, less is known about the contextual factors surrounding tool use, such as staff discipline and grade and timing and frequency of use, and whether there is variation between wards and settings. There also remains significant heterogeneity in the protocols and processes in place for delirium management. Effective delirium management is challenging, for reasons including resource constraints, insufficient staffing and resources and lack of awareness, education and training, amongst others.10,11 Specific prevention initiatives have been demonstrated to be effective in research studies. 12 Hospital Elder Life Program (HELP) is an evidence-based model shown to reduce the incidence of delirium which involves a targeted multicomponent strategy to prevent cognitive and functional decline in hospitalised older adults. 13 Similarly use of the ABCDEF bundle (Assess, prevent and manage pain; Both spontaneous awakening and breathing trials; Choice of analgesia and sedation; Delirium assess, prevent and manage; Early mobility and exercise; Family engagement/empowerment) in ICU settings has demonstrated improved outcomes for patients including lower likelihood of delirium. 14 However, these multi-component non-pharmacological interventions are complex, resource intensive and may require adaptation for other settings.
This substudy analysed national Scottish data collected as part of a global delirium point prevalence study on World Delirium Awareness Day (WDAD) 2023. 15 That study reported data from 44 countries on 36,048 patients and demonstrated that validated delirium assessments were used in 66.7% of wards/units and that 66.8% of wards/units used delirium management protocols, with significant variability between countries. The study also reported that a protocol for delirium management is associated with improved non-pharmacological interventions and suggested that implementation of delirium protocols could reduce existing barriers to effective delirium management.
In Scotland, acute care is delivered through the National Health Service and national guidelines set the standard for delirium risk reduction and management. 16 This study’s main aim was to describe the use of validated delirium assessment tools and adherence to national guidelines across Scotland. The secondary aims were to describe the prevalence of delirium, the protocols, processes and interventions used as part of delirium management and barriers to effective delirium assessment and management.
Methods
This was a secondary analysis of national Scottish data collected as part of a worldwide, cross-sectional, 1-day point prevalence study on WDAD, 15th March 2023. Methods of the primary study have been published previously. 15 The study was performed as audit of recommended best practice and each site followed local routes for approvals. The questionnaire of staff and data handling was approved by the University of Glasgow College of Medical, Veterinary and Life Sciences (MVLS) ethics board (application 200220143).
All health boards in Scotland were contacted to identify potential hospitals that could contribute. We limited data collection to hospitals with over 100 acute inpatient beds. From the list of eligible sites, the team contacted leads who may wish to participate and the local leads organised data collection at site. Participating clinicians reported the number of patients with and without delirium in their wards/units on WDAD, 15 March 2023, at 8 am in the morning and 8 pm in the evening. All patient data were fully anonymised, and no identifiable information was collected. Contextual data collected included numbers of patients, name of delirium assessments, presence of specific delirium management protocols, responsible clinicians, delirium awareness activities, non-pharmacological and pharmacological interventions, and ward/unit specific barriers to delirium assessment and management.
Settings and population
All in-patients in acute hospitals, rehabilitation facilities, prolonged-ventilation weaning centres, palliative centres or nursing homes were eligible for inclusion. Included patients were of all age groups, from all disciplines, and all types of wards/units, including emergency departments, ICU, high acuity units, intermediate care units and general wards. Excluded were patients from the anaesthesia/operation theatre, home care and ambulatory care.
Data collection
The survey consisted of 14 sections containing 39 questions about the country, sociodemographic information of participants, hospitals and ward/unit-specific data (Supplemental Appendix 2). It also included questions about the presence of delirium-related protocols; delirium awareness interventions such as posters, lectures, providing pocket cards and others; non-pharmacological interventions for prevention and therapy applied for >50% of delirious patients; pharmacological interventions applied for >50% of delirious patients; pharmacological management; and perceived barriers to delirium management. Respondents reported delirium assessments from a list of 21 assessments, including Confusion Assessment Method (CAM), 4AT (4 ‘A’s Test) and other validated assessments, no/subjective assessment or other.
Analysis
The analysis of nominal data has been reported as frequency (n) and percentage (%). Due to non-normal distribution, numerical data have been reported as the median and inter-quartile range (IQR). Ordinal data have been reported in its modus. Given the descriptive nature of the study, no adjustments were made for confounding factors.
95% Confidence intervals (CI) were calculated using the normal approximation to the binomial calculation. Chi-squared test of independence was used to analyse the association between categorical variables with statistical significance level set at 0.05.
Results
Data collection
One hundred twenty-two survey responses were received from 13 hospitals across mainland Scotland (Figure 1 and Table 1), including information on 3,257 patients at 8 am and 2,436 patients at 8 pm on 15th March 2023.
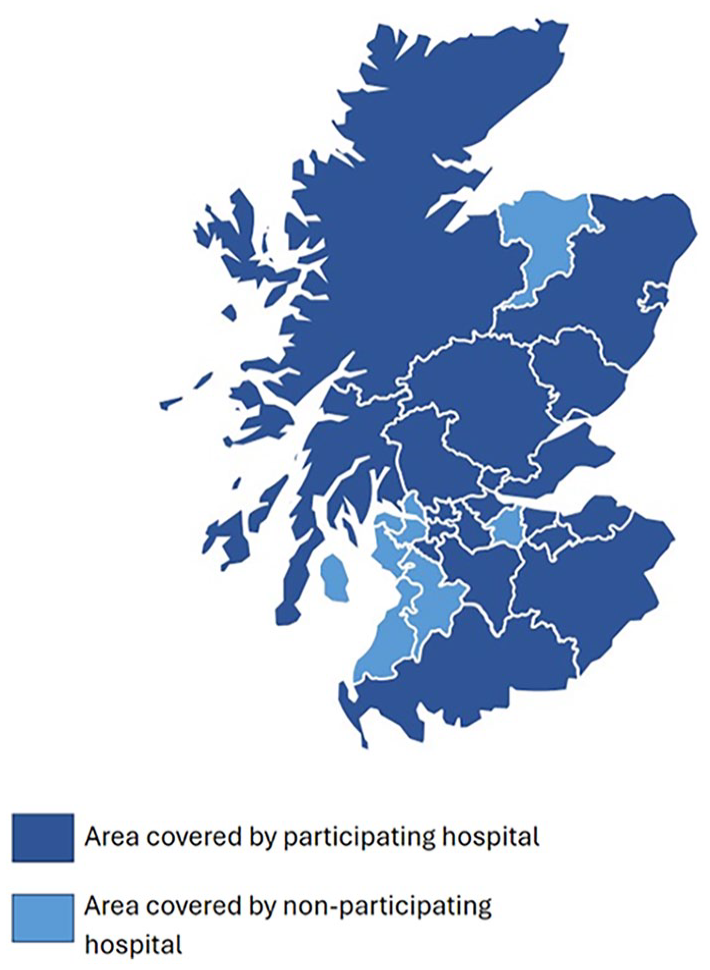
Survey coverage across mainland Scotland by region.
Proportion of unit types by specialty and acuity.
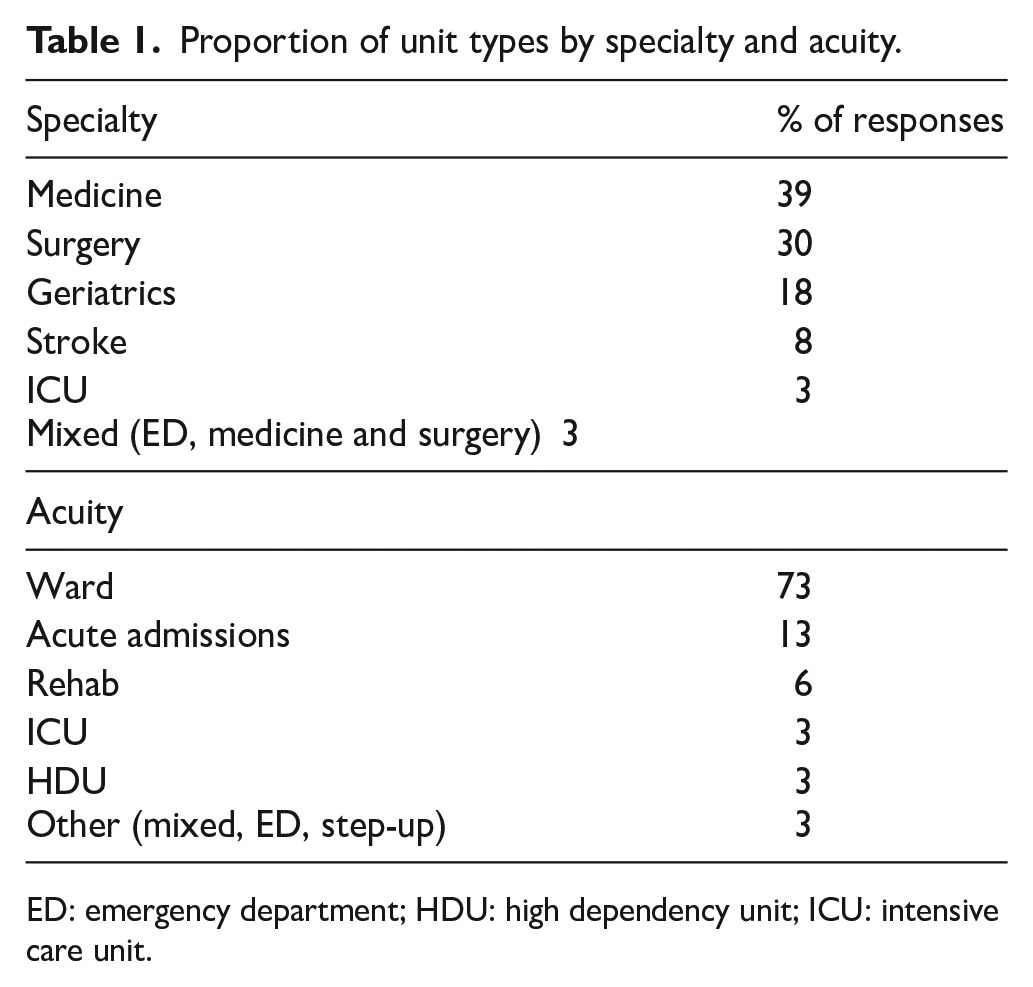
ED: emergency department; HDU: high dependency unit; ICU: intensive care unit.
Most survey respondents were physicians (73%, n = 87/120), with 51% of responders (n = 61/120) describing themselves as occupying a leadership position, or partly in a leadership position, on the unit. Most were working in a medical discipline (55%, n = 66/120) and on general adult wards (83%, n = 100/120).
Data were collected from university hospitals (48%, n = 58/120) or university-associated hospitals (52%, n = 62/120). The median number of hospital beds per unit was 27 (IQR 9) and most units reported on patients of mixed ages (44%, n = 53/120).
Delirium detection
The most frequently used validated assessment tool was the 4AT (75%, n = 90/120). Personal judgement was the second most reported assessment method (14%, n = 17/120). In the ICU setting, the CAM-ICU was the most frequently reported tool (75%, n = 3/4). The frequency of delirium assessment varied (Figure 2) with most responses (30%, n = 36/119) opting for ‘other’ and a free text response. A total of 19/36 free text responses indicated delirium assessment was required ‘on admission and sudden change in condition’.
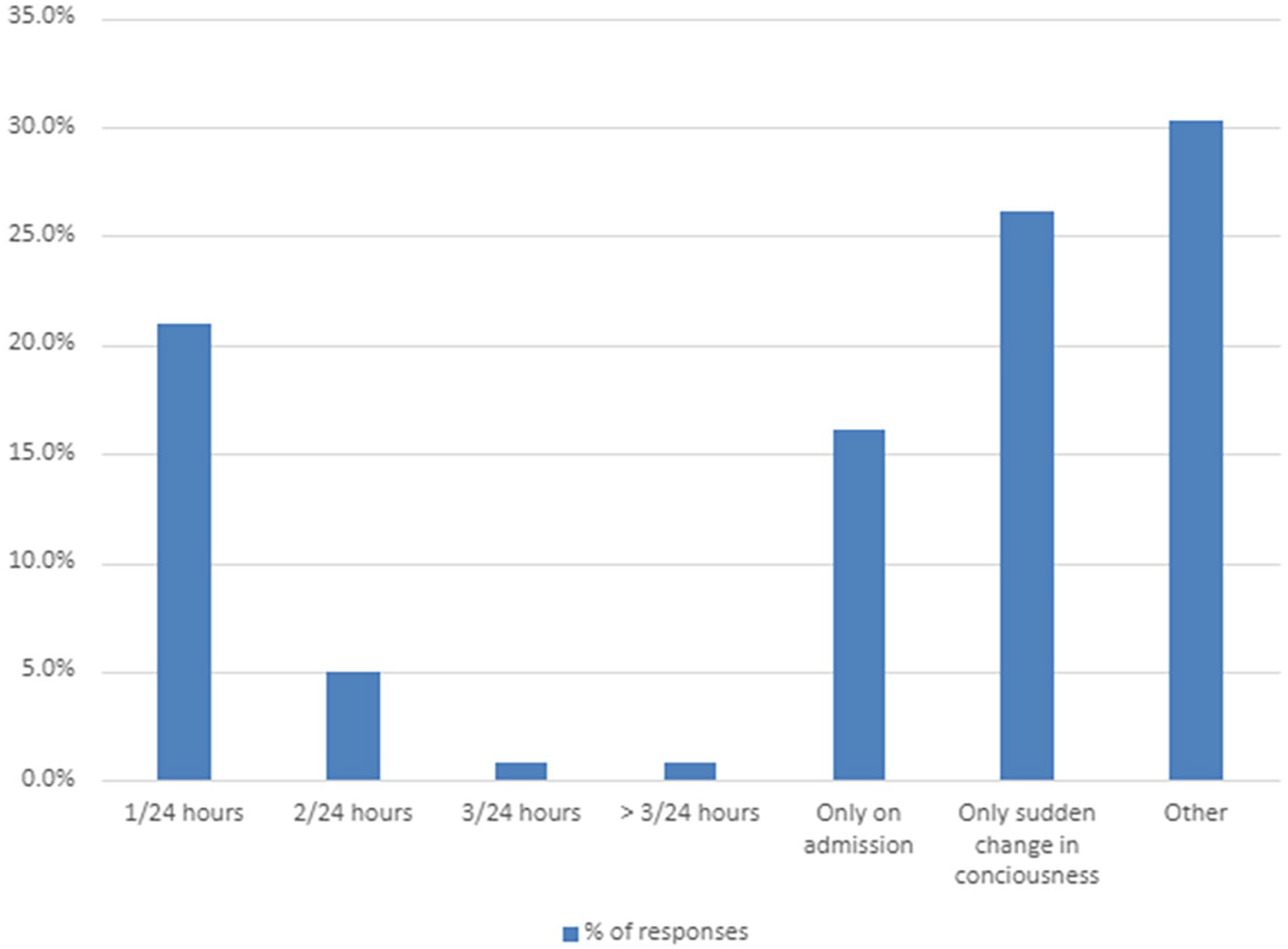
Reported frequency of delirium assessment.
The profession most commonly reported as primarily responsible for delirium assessment was nurses (48%, n = 57/120), followed by physicians (26%, n = 31/120). This was consistent amongst all specialties except ICU where physicians were most commonly reported to be responsible for delirium assessment (50%, n = 2/4).
Delirium prevalence
Survey responses suggested relatively high overall rates of delirium assessment with 74% (n = 2,424/3,257) patients assessed at 8 am and 79% (n = 1,914/2,436) assessed at 8 pm. The overall prevalence of delirium (as assessed using a variety of methods) was 22% (n = 540/2,424) at 8 am and 23% (n = 444/1,914) at 8 pm.
When compared by specialty, delirium prevalence was highest on geriatric medicine units at 8 am and 8 pm and lowest on surgery (Figure 3). A chi-square test of independence demonstrated the relationship between specialty and prevalence of delirium was significant at both 8 am; Χ 2 , (1, n = 2,411) = 184.68, p < 0.001 and 8 pm; Χ 2 , (1, n = 1,903) = 146.06, p < 0.001.
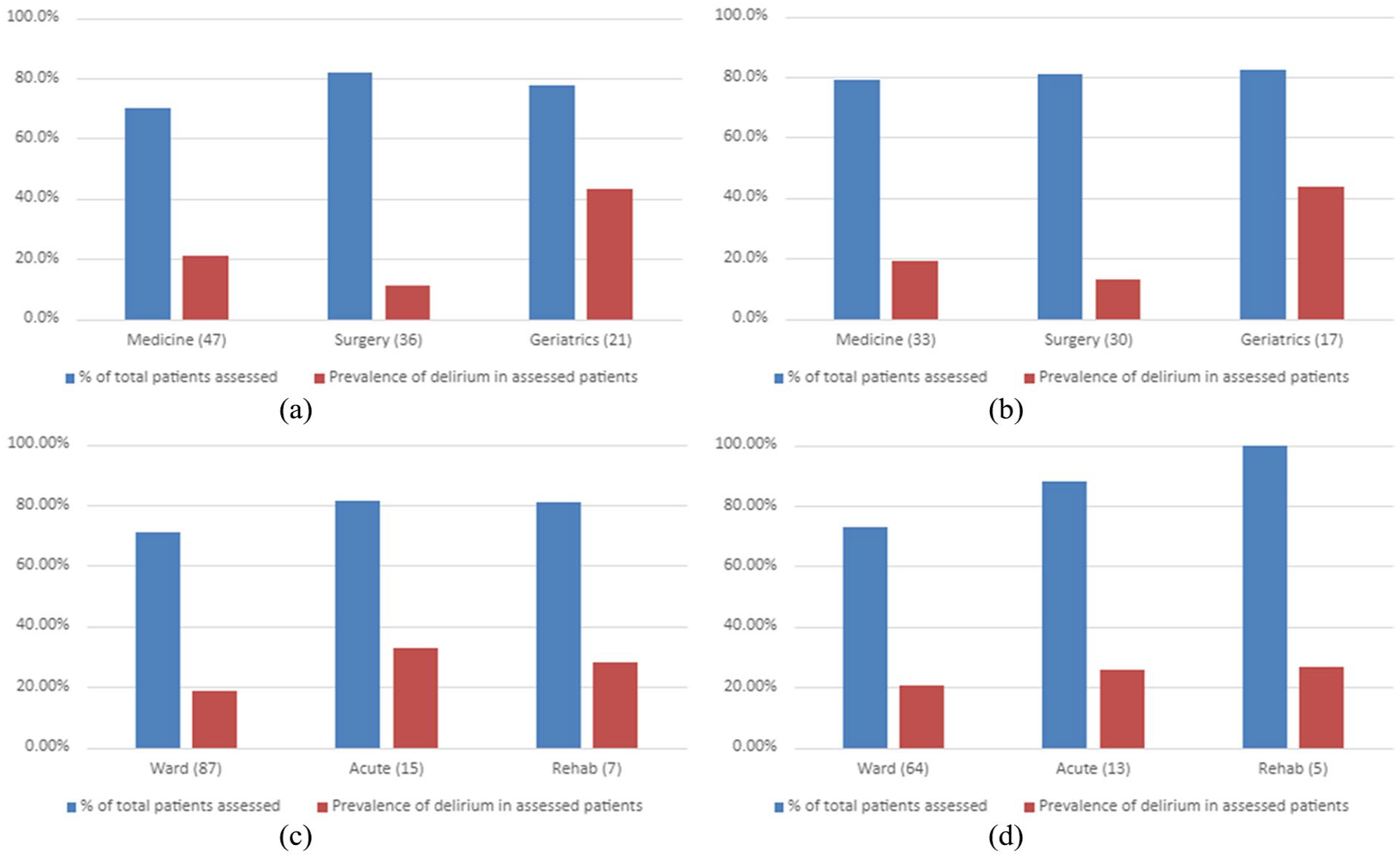
Delirium assessment and prevalence at (a) 8 am by unit specialty, (b) 8 pm by unit specialty, (c) 8 am by unit acuity and (d) 8 pm by unit acuity.
When compared by acuity, delirium prevalence was highest in acute receiving units at 8 am and rehabilitation units at 8 pm (Figure 3). A chi-square test of independence confirmed the relationship between acuity and prevalence of delirium was significant at 8 am; Χ 2 , (1, n = 2,327) = 47.22, p < 0.001 but not at 8 pm; Χ 2 , (1, n = 1,779) = 8.16, p = 0.09. Further data comparisons for all unit specialties and acuities are available in Supplemental Figure 1.
Delirium protocols and structures
Respondents were asked about written protocols on their units (Table 2). The most frequently reported written protocols included delirium management, pain management and nutrition management.
Written protocols present on the unit.
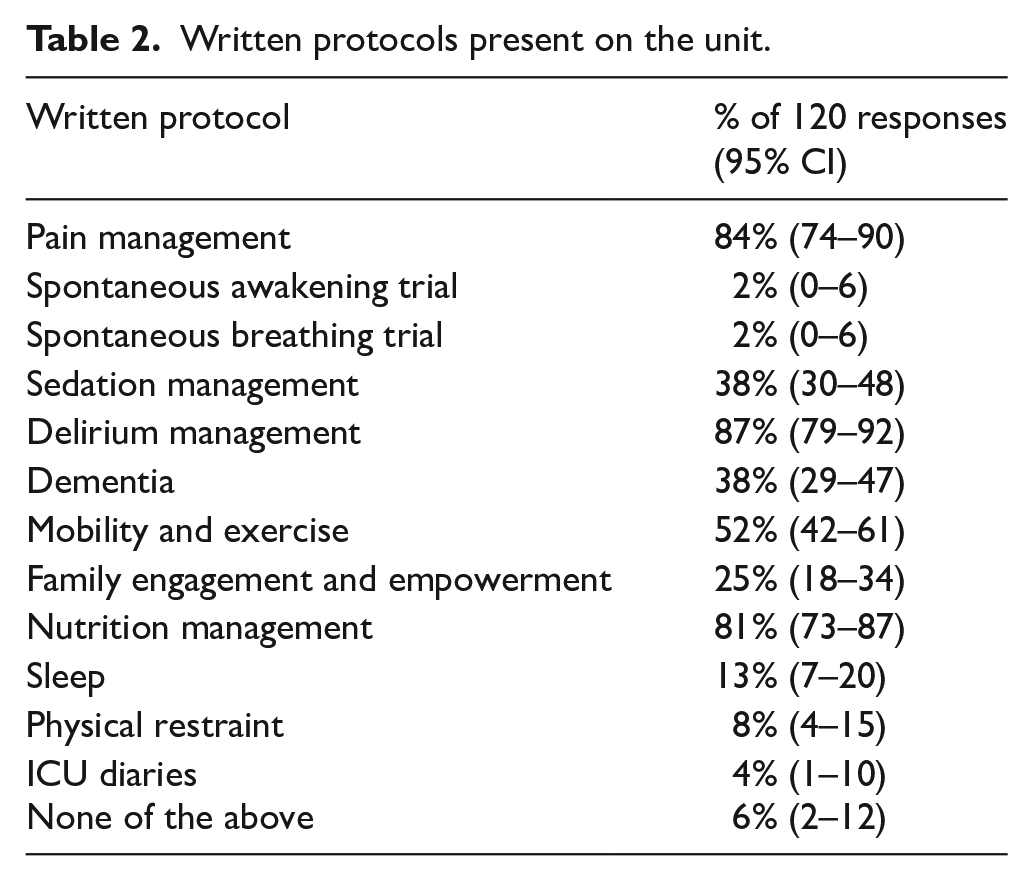
The most frequently reported delirium awareness interventions present on units included delirium being mentioned at handover (80%, 95% CI 71–87) and information posters about delirium (76%, 95% CI 68–84) (Supplemental Table 1).
Delirium interventions
The most common routine non-pharmacological interventions across all units were reported as pain management (88%, n = 106/120), adequate fluids (88%, n = 105/120) and open daytime visiting for families (80%, n = 96/120). Variation in the preferred non-pharmacological intervention was noted when comparing units by specialty and acuity (Table 3).
Most reported non-pharmacological interventions by specialty, including only units with >5 responses.
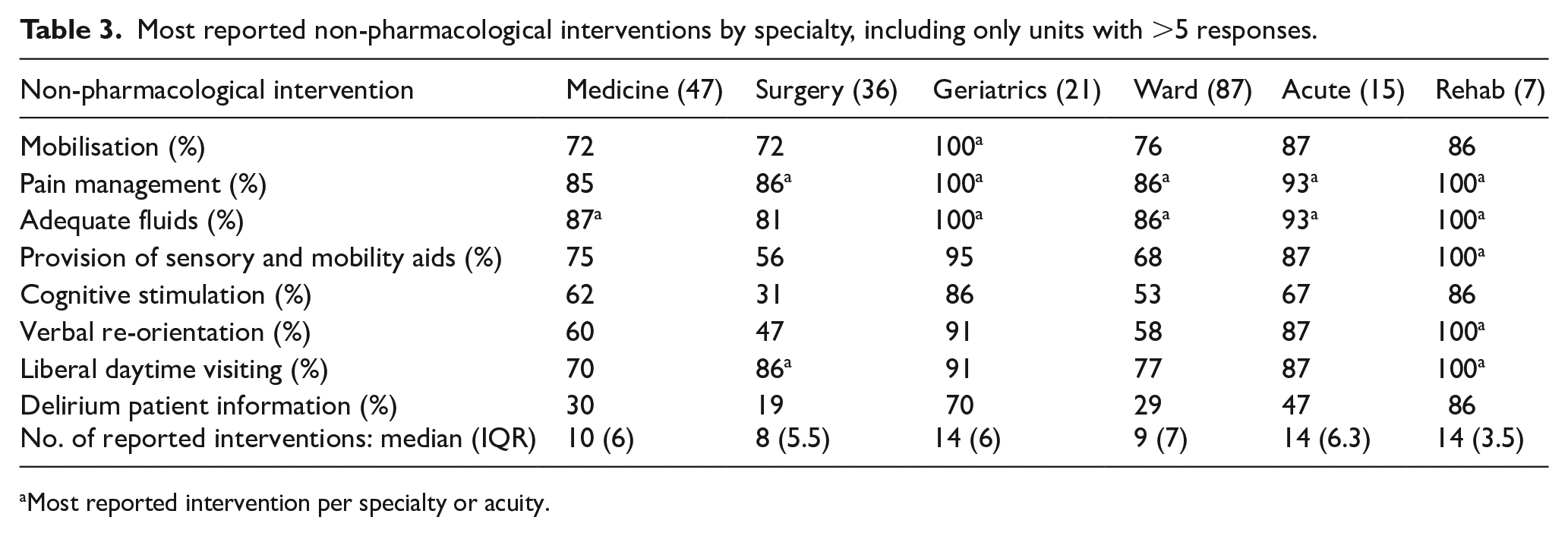
Most reported intervention per specialty or acuity.
The most common pharmacological interventions were reported to be evaluation of drugs by a specialist (57%, n = 68/120), reduction of drugs potentially contributing to delirium (48%, n = 58/120) and haloperidol (30%, n = 36/120). The pharmacological management of patients with delirium was most often reported to be based on an individual approach (74%, n = 89/120) and dependent upon specific symptoms of each patient’s delirium (71%, n = 85/120).
Delirium care barriers
The most reported barriers to implementation and/or use of evidence-based strategies in delirium assessment and management were staff shortages (86%, n = 101/117) and lack of time to educate and train staff (83%, n = 97/117). Only one geriatric medicine unit (5%, n = 1/21) and one ICU unit (25%, n = 1/4) reported no barriers to delirium assessment and management.
Survey respondents were asked for their opinions on issues that should be a high priority for future delirium care and research. For delirium care, the issues mentioned most often included increased awareness, increased education and improved staffing. Regarding delirium research, the issues mentioned most often included treatment of delirium, causes of delirium and special groups including those with frailty and younger people.
Discussion
This secondary analysis of data from an international survey-based study has led to valuable insights into delirium assessment and management practices and protocols in 13 distinct care settings across Scotland. We found that while the 4AT is the most widely used assessment tool, 14% of settings reported using clinical judgement alone. There was heterogeneity in the frequency of tool use and responsible profession by care setting and acuity. We also highlighted current processes and protocols for delirium care and specific barriers to effective assessment and management.
The prominence of the 4AT as the most widely used delirium assessment tool reflects national Scottish guidelines for delirium assessment, which recommends that the 4AT is used in acute hospital settings and considered in the community and other settings. 16 The 4AT is extensively validated, does not require specific training, is brief and easy to use and has wide applicability in various clinical settings.8,17,18 The current study only reported data from four ICU settings – however, most of these reported use of the CAM-ICU, a highly validated and effective tool for delirium assessment in ICU patients. 19 A recent systematic review suggested that the CAM-ICU may have a role in early identification of delirium in patients in ICUs, when applied by properly trained personnel. 20 However, it is of concern that 14% of units reported using clinical judgement, even though this may introduce variability and reduce the consistency of delirium detection as use of a structured assessment tool has been shown to be more effective than clinical judgement alone. 7
This study also highlighted heterogeneity in the frequency of and professionals responsible for delirium assessment across settings and levels of clinical acuity. This observation is supported by previous studies, which have highlighted diverse approaches to delirium care and by a systematic review demonstrating that delirium assessment tools are used at different timepoints and frequencies in the patient’s journey.9,21 Our observation may reflect variations in the infrastructure, staffing, and resources available across settings. However, if tools are used in in ways other than recommended, this may lead to lower delirium assessment and positive score rates than expected. 9
Most units (86.7%) reported having written protocols for delirium management on the ward. Again, this likely reflects the presence of national guidelines on risk reduction and management of delirium. 16 It would be useful to review the different protocols to determine alignment across settings. However, despite the widespread presence of written delirium management protocols, we found notable variation in reported interventions for delirium. A previous Cochrane systematic review found that multi-component non-pharmacological interventions reduced the incidence of delirium. 22 Although we found evidence that many units were implementing multiple non-pharmacological interventions, including pain management, mobilisation, hydration and provision of sensory and mobility aids, there was variation by unit and acuity, and some interventions including verbal reorientation and cognitive stimulation were not frequently used, despite evidence that these may be beneficial in delirium. 23 Around half of units reported specialist medications review and reduction of drugs potentially contributing to delirium – both recommended by national guidance. 16 Around 30% also reported use of haloperidol. Systematic reviews have not shown evidence of benefit for haloperidol for prevention of delirium and no antipsychotics are licensed for delirium prophylaxis in Scotland.16,22,24 Another Cochrane review concluded that antipsychotics (including haloperidol) did not reduce delirium severity, resolve symptoms or reduce mortality in the acute care setting, although no serious side effects were reported in the studies of haloperidol.25 –28 National guidelines suggest that if commenced, antipsychotics should be reviewed daily and stopped as soon as the clinical situation allows, typically within 1–2 days. 16 More detailed investigation is needed to determine if reported pharmacological interventions are being implemented within national guidelines.
Finally, we also reported barriers to implementation and/or use of evidence-based delirium assessment and management strategies. Many of the responses focused on insufficient staffing and time for staff training and education. This is supported by existing studies, which have also highlighted additional issues including organisational culture, competing clinical priorities, heavy workload and a discordance between perceived capabilities and knowledge.10,11 Identification of existing barriers is important to inform the design and delivery of future delirium assessment and management initiatives, to ensure that these are feasible and can be implemented effectively as part of routine clinical care.
Strengths and limitations
This study has demonstrated several strengths. Data were collected as part of a large national survey, incorporating responses from 13 different hospitals across Scotland representing the majority of the mainland population, with care settings including medicine, surgery and ICU. It provided information specific to guide development and improvement of delirium assessment and management practices in Scotland. The study was performed as part of a much larger study for WDAD and may contribute to increased awareness of delirium assessment and management.
We have noted limitations. All survey data were provided by participating clinicians, without verification of the data provided. Although we had good national coverage with many participating centres, there may be bias in centres which chose to participate which may be more focused on good quality delirium care. Findings may not be nationally representative, and more work is needed to understand barriers in other contexts. The original survey was not designed specifically for Scotland, there were few white space questions, and we were unable to ask for additional information to clarify or enhance survey data. We were therefore not able to assess adherence to many of the recommendations included in national delirium care guidelines. 16
Conclusion
This study has demonstrated that a significant number of acute care settings follow national guidance for delirium assessment and management. However, some still rely on clinical judgement for assessment rather than a validated tool such as the 4AT, and there is heterogeneity in non-pharmacological and pharmacological management practices by setting. Importantly, we have identified important barriers to effective delirium assessment and care, including lack of staffing and specific training, that can be targeted to improve delirium care practices and hopefully outcomes for acutely hospitalised patients in Scotland.
Supplemental Material
sj-docx-1-rcp-10.1177_14782715241301486 – Supplemental material for Delirium assessment, management and barriers to effective care across Scotland: A secondary analysis of survey data from World Delirium Awareness Day 2023
Supplemental material, sj-docx-1-rcp-10.1177_14782715241301486 for Delirium assessment, management and barriers to effective care across Scotland: A secondary analysis of survey data from World Delirium Awareness Day 2023 by Fariha Naeem, Rose S Penfold, Roy L Soiza, Rebecca Von Haken, Heidi Lindroth, Keibun Liu, Peter Nydhal and Terry J Quinn in Journal of the Royal College of Physicians of Edinburgh
Footnotes
Acknowledgements
Author contributions
F.N. and R.S.P.: investigation, project administration, writing original draft; R.L.S.: investigation, project administration, writing review and editing; R.V.H., H.L., K.L., and P.N.: conceptualisation, data curation, methodology, writing review and editing; T.J.Q.: data curation, methodology, supervision, writing review and editing.
Consent to participate
Not applicable. All patient data were fully anonymised, and no identifiable information was collected.
Consent for publication
Not applicable.
Data availability
For the purpose of open access, the author has applied a CC-BY public copyright licence to any Author Accepted Manuscript version arising from this submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. R.S.P. is a fellow on the Multimorbidity DTP for Health Professionals, which is supported by the Wellcome Trust [223499/Z//21/Z].
Ethical considerations
The study was performed as audit of recommended best practice and each site followed local routes for approvals. The questionnaire of staff and data handling was approved by University of Glasgow MVLS ethics board (application 200220143).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.